
Abstract
Purpose:
Hemithyroidectomy is an appropriate procedure that is recommended for a number of thyroid conditions to preserve the functional contralateral thyroid lobe, but patients who underwent a hemithyroidectomy still run the risk of developing hypothyroidism. This study aimed to determine the incidence of hypothyroidism following a hemithyroidectomy as well as predictive risk factors.
Methods:
A retrospective analysis was carried out on all patients who underwent hemithyroidectomy between 2016 and 2022. Age, gender, preoperative and postoperative thyroid stimulating hormone (TSH) and free thyroxin (FT4), side, and volume of the remaining lobe, as well as the histologic diagnosis, were all examined in the patients. To identify the predictors of hypothyroidism, statistical analyses, both univariate and multivariate, were conducted.
Results:
Out of 224 patients, 18.25% had hypothyroidism following surgery. This complication appeared within the first year in 88% of the cases. Patients with thyroiditis (P = .036), preoperative TSH levels greater than 1.72 mIU/L (P < .001), right side hemithyroidectomy (P = .017), and residual lobe volume less than 3.57 cm (P < .001) had a significantly higher risk of developing hypothyroidism.
Conclusion:
After hemithyroidectomy, hypothyroidism is a major complication that should be carefully evaluated preoperatively based on risk factors of hypothyroidism. Furthermore, our results confirm the need for routine serum TSH monitoring for a minimum of 1 year following hemithyroidectomy.
Introduction
Since the emergence of neck ultrasonography, the prevalence of thyroid nodules has increased drastically. Most of these nodules are benign. 1 Hemithyroidectomy consists of resecting a single thyroid lobe and the isthmus while preserving the integrity of the contralateral lobe. This technique is increasingly used to treat unilateral benign thyroid nodules and infracentimetric differentiated thyroid carcinoma. Complications of this surgery include hematoma, infection, recurrent laryngeal nerve injury, and hypothyroidism. 2 In the past, most patients undergoing hemithyroidectomy were systematically prescribed levothyroxine to prevent nodular recurrence in the unresected lobe. However, this approach is no longer recommended due to its long-term adverse effects on the cardiovascular and skeletal systems.3,4 However, the incidence of hypothyroidism after hemithyroidectomy is approximately 30% in published literature. 5
This study aimed to determine the incidence of hypothyroidism after hemithyroidectomy and identify the predictive factors for this complication.
Methods
Setting and Design
We conducted a retrospective study in the otorhinolaryngology department of Charles Nicolle Hospital in Tunis. We included in our study, all adult patients who underwent hemithyroidectomy between 2016 and 2022 (7 years), with no history of cervical irradiation, a normal preoperative thyroid workup, and a postoperative follow-up of at least 12 months. We excluded from our study patients who were treated with levothyroxine or antithyroid drugs prior to surgery, and patients whose anatomopathological study of the resected tissue showed a malignant lesion requiring thyroid re-operation.
Euthyroidism was determined by the presence of normal serum TSH and free T4 levels. The reference range for normal serum TSH is 0.55 to 4.78 μIU/mL using chemiluminescence (Atellica® Siemens Healthineers) and the reference range for normal serum-free T4 is 0.89 to 1.76 ng/dL using chemiluminescence (Atellica® Siemens Healthineers). Subclinical hypothyroidism was defined as an elevation of serum TSH levels (between 5 and 10 μUI/mL) with a normal level of free T4. Overt hypothyroidism was identified as an increase in serum TSH (above 5 μUI/mL) with a decrease in free T4 level. Some subclinical hypothyroidism returned to normal, while others evolved into overt hypothyroidism.
The reference values for TSH and free T4 concentrations were set between 0.35 and 5 μUI/mL and 0.7 and 1.48 ng/mL respectively, in accordance with the values of our biochemistry laboratory.
Data Collection
We analyzed patients’ medical records and operative reports to extract the following data: age, gender, medical, history, preoperative serum TSH and free T4 hormone level, resected side, and volume of the remaining lobe, as well as the histologic diagnosis.
Statistical Analysis
SPSS (IBM, Armonk, NY, USA) version 27 software was used for statistical analysis of the data collected.
For quantitative variables, we calculated means, standard deviations, and medians, and determined extreme values (minimum and maximum). For qualitative variables, we calculated frequencies and percentages.
Our population was divided into two groups: those who developed hypothyroidism postoperatively (overt or subclinical hypothyroidism) and those who maintained euthyroidism postoperatively.
The statistical significance of the difference between these two groups was analyzed using Student’s t-test for quantitative variables and chi-square test for qualitative variables.
Multivariate analysis was performed using logistic regression to determine independent factors associated with the occurrence of hypothyroidism, considering variables significantly associated with hypothyroidism (P < .05) in univariate analysis, borderline variables (P < .2), as well as age and gender.
The cutoff value of quantitative variables statistically significant in predicting the onset of hypothyroidism was estimated using receiver operating characteristic (ROC) curves.
A P-value below .05 was considered significant.
Retrospective studies are exempt from ethics committee approval in our institution.
Results
A total of 224 patients were included. The mean age was 48.65 ± 12.9 years. Our population was predominantly female, with 199 women (88.8%), for a gender ratio of 0.125 (Table 1).
General Characteristics of Studied Patients.

After surgery, hypothyroidism was diagnosed in 42 patients, with an incidence of 18.75% among them 88% were diagnosed within the first year. Among those 42 patients, 25 had subclinical hypothyroidism and 17 had overt hypothyroidism. Only five patients in the subclinical hypothyroidism group regained euthyroidism.
The association between clinical, biological, and pathological findings and the occurrence of hypothyroidism after hemithyroidectomy is outlined in Table 2. Preoperative TSH level, right-side hemithyroidectomy, volume of unresected lobe, and the coexistence of lymphocytic thyroiditis were found to be significantly associated with the onset of hypothyroidism after hemithyroidectomy in the univariate analysis.
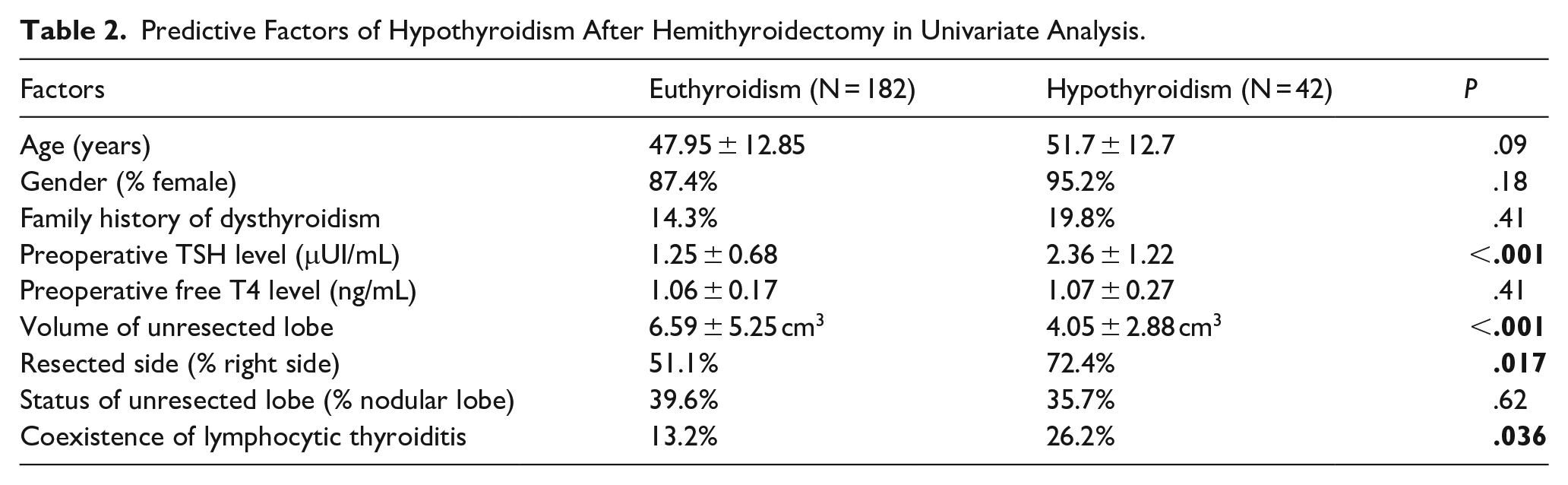
Predictive Factors of Hypothyroidism After Hemithyroidectomy in Univariate Analysis.
In this study, preoperative TSH levels was higher in patients who developed hypothyroidism than those who did not (P < .001). The threshold limit determined by the ROC curve was 1.72 IU/mL (Figure 1).
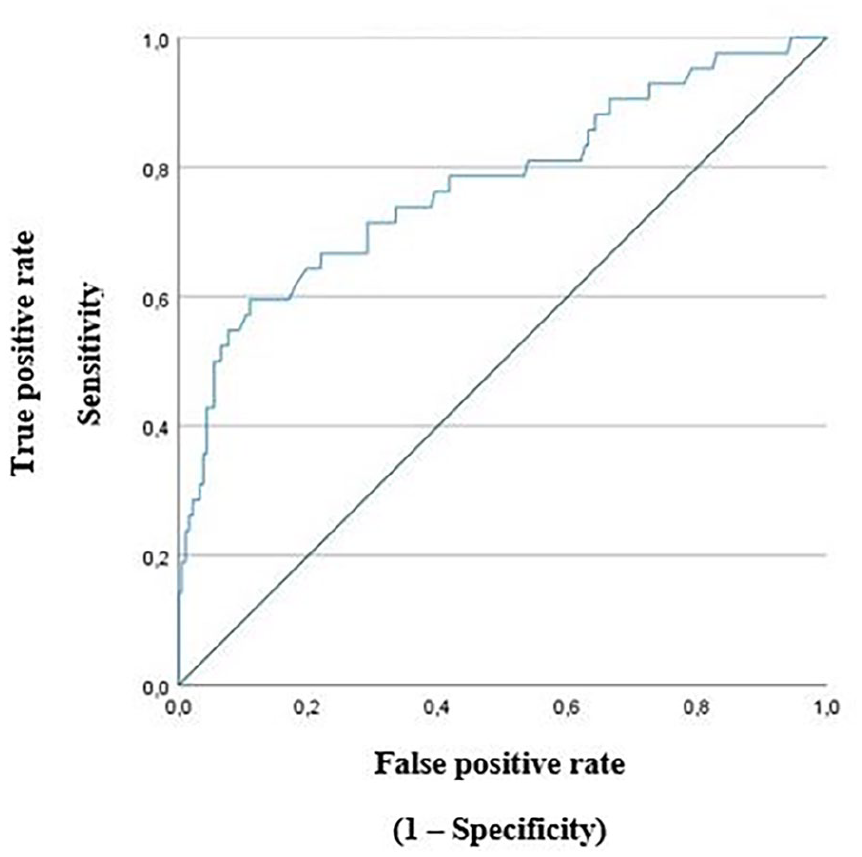
ROC curve of preoperative TSH level.
Regarding the volume of the non-resected lobe, the cutoff point determined by the ROC curve was 3.57 cm3. Below 3.57 cm3, patients were 5.16 times more likely to progress to hypothyroidism (Figure 2).
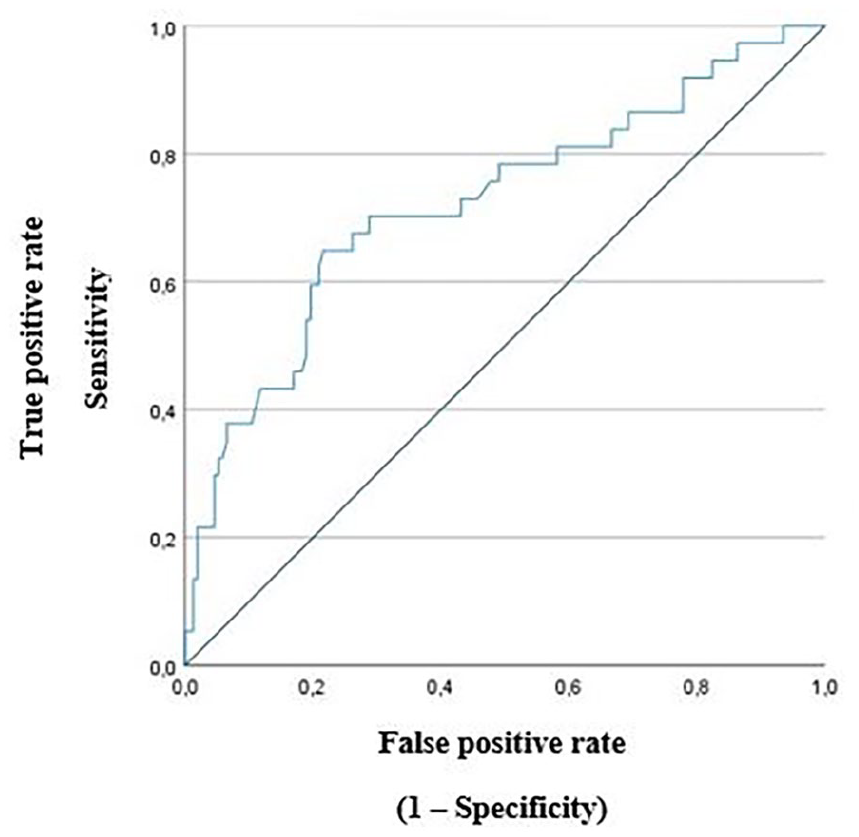
ROC curve of unresected lobe volume.
In multivariate analysis with adjustment, preoperative TSH level (P < .001), right-side hemithyroidectomy (P = .04), and volume of unresected lobe (P = .031) were confirmed as independent risk factors for the onset of hypothyroidism after hemithyroidectomy.
Discussion
In our study, the prevalence of hypothyroidism following hemithyroidectomy was 18.75%, with 88% of patients diagnosed within the first year following surgery. Four factors significantly associated with the occurrence of hypothyroidism were identified: a preoperative TSH level >1.72 μUI/mL, an unresected lobe volume <3.57 cm3, a right-sided resected lobe and lymphocytic thyroiditis.
One thyroid lobe theoretically contains enough thyrocytes to ensure a normal thyroid function. 5 However, hypothyroidism is an important complication after hemithyroidectomy with an incidence rate around 30%.2,5 Published studies report a wide range of incidences, from 0.6% to 68.1%. 5 The heterogeneity of these results can be attributed to cross-country genetic, environmental, and socio-economic variations,5,6 and to the diversity of biological definitions of hypothyroidism between studies.5,7
Since the half-life of TSH is approximately 7 days. It is recommended to wait 2 months, or for a minimum of four to five TSH half-lives, before measuring its level, to obtain an accurate assessment of the thyroid hormone produced by the residual thyroid tissue. 8
The onset of hypothyroidism often occurs within the first month after surgery. However, in some patients, hypothyroidism is not detected until 6 to 12 months after surgery and less often after the first year, requiring long-term follow-up.9-11
Patients with overt hypothyroidism are treated systematically. However, the management of patients with subclinical hypothyroidism will depend mainly on the presence of clinical symptoms and their follow-up or, for some authors, if the TSH level is greater than 10 mIU/L.11,12
The remission rate of hypothyroidism after hemithyroidectomy is over a third of patients and is associated with a lower preoperative TSH level.7,13
With regard to predictive factors of hypothyroidism, our results are fully consistent with the published literature. Preoperative TSH level is almost the most cited predictive factor of hypothyroidism, according to the majority of published studies and meta-analyses.2,5-16 TSH cutoff for increased risk ranges from 1.5 to 3 μIU/L. 2
Lymphocytic thyroiditis found in the resected side has also been associated with hypothyroidism in several series but this can only be diagnosed postoperatively.2,5,6,9-11,13,14,16 Patients with significant lymphocytic infiltration are at greater risk of developing postoperative hypothyroidism than patients with minimal infiltration. 17
Other factors were found only in a few series, such as older age, female gender, weight, preoperative free T4 level, higher serum thyroid antibodies, right-side hemithyroidectomy, smaller unresected lobe volume, and the presence of contralateral nodule.2,5,7,13,15,18,19
Female patients are more prone to thyroid autoimmunity, which increases with age. Over 80% of patients with thyroiditis and the resulting hypothyroidism have thyroid antibodies. The presence of thyroid antibodies may reflect abnormal activation of the immune system directed against thyroid cells. Thus, if remaining thyroid tissue is also the target of this autoimmune response, it may further compromise remaining thyroid function and thus lead to progression toward hypothyroidism.5,20
Based on the literature, the thyroid gland is irregular and asymmetrical in shape, and the right lobe is larger than the left which may explain the fact that some series and ours have found that right lobe resection is associated with hypothyroidism.7,21,22
The volume of unresected tissue can be easily calculated from cervical ultrasound data. Since thyroid volume is significantly correlated with body surface area, the volume of the remaining lobe should be adjusted to body surface area, according to some authors.10,23,24
Our study has its limitations; as with most retrospective studies, its retrospective nature restricted the precision of our results. Some patients’ records were missing data, and some could not be retrieved or were unexploitable and therefore excluded from our analysis. Furthermore, some of our patients were lost to follow-up and did not have a postoperative thyroid check-up. These patients were also excluded from the study. In some cases of subclinical hypothyroidism, levothyroxine replacement therapy has been initiated immediately; therefore, spontaneous recovery of thyroid function may go unnoticed.
Conclusion
While every patient undergoing total thyroidectomy will need a thyroid hormone replacement for life, only a proportion of patients undergoing hemithyroidectomy will require the same. Therefore, it is essential to identify these risk factors to improve preoperative counseling, management strategies, and patient follow-up. After hemithyroidectomy, all patients should be monitored especially during the first year of follow-up. Particular attention and frequent check-ups should be given to those with lymphocytic thyroiditis or elevated preoperative TSH levels.