
Abstract

Significance Statement
Temporal pain is rare in the pediatric age group. In the presence of unilateral temporal pain, an underlying pathological cause should be investigated. Dermoid cysts in children generally do not cause pain. However, in cases of unilateral pain accompanied by swelling, dermoid cysts should be considered a rare pathological cause in pediatric patients. In such cases, intradiploic invasion of the dermoid cyst should be considered.
Four-year-old patient presented to the pediatric clinic with periorbital swelling and unilateral temporal pain. The patient had no known medical history, surgical history, or history of trauma. On physical examination, swelling was observed in the right frontotemporal region. A noncontrast brain CT scan was performed. Axial CT images revealed a lesion in the temporal bone causing diastasis in the intradiploic space, visible in both the bone (Figure 1A) and the brain (Figure 1B) windows. The lesion extended from the temporal bone to the frontal bone. In the periorbital region, the lesion caused minimal swelling under the skin with a cystic-fat density (Figure 1A and B, white arrows). The cystic lipomatous lesion extended approximately 17 mm within the temporal bone’s intradiploic space (Figure 1A and B, black arrows). The patient’s pain was believed to be due to the lesion’s extension into the intradiploic space. A 3D volumetric rendering CT showed remodeling of the frontal bone, creating a foramen (Figure 1C, black arrowheads). The patient underwent surgery performed by the neurosurgery department. The pathological examination of the surgical specimen was reported as a dermoid cyst. On postoperative follow-up, it was found that the patient’s temporal pain had resolved.
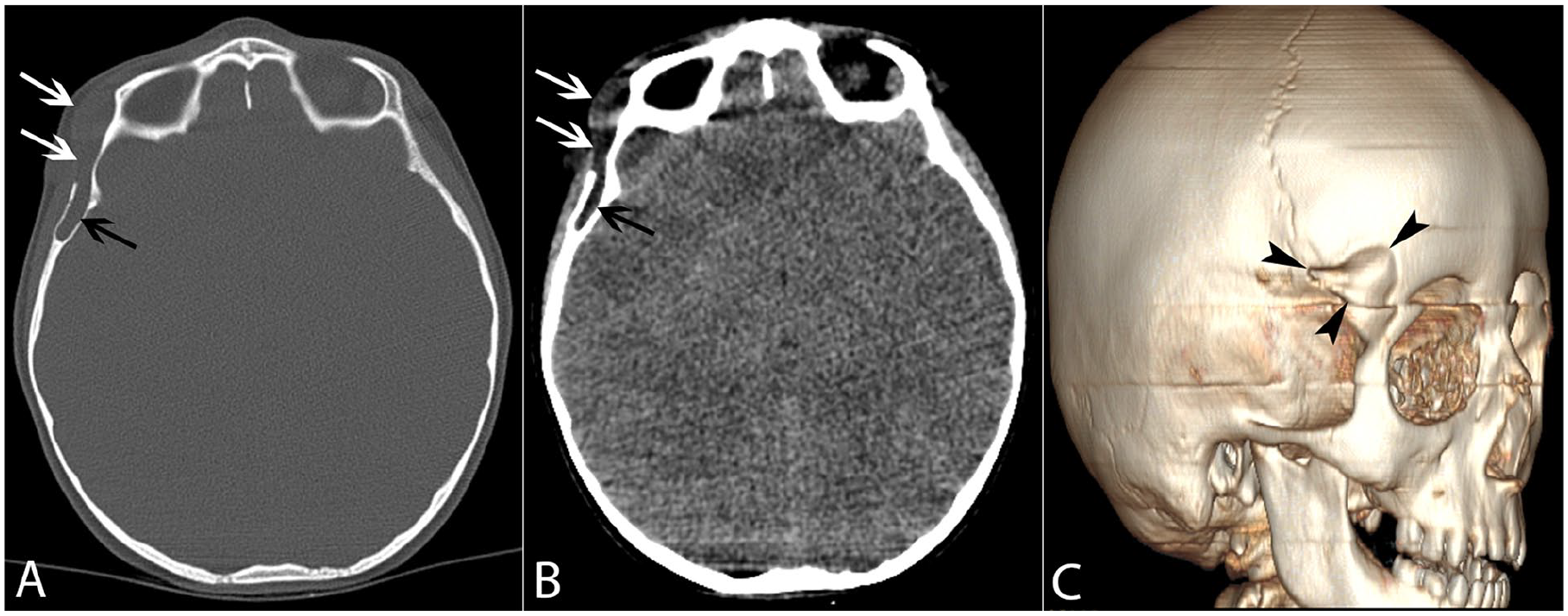
The patient’s axial noncontrast CT images are showing a fat-containing cystic lesion observed in both the bone (A) and brain (B) windows, extending from the intraosseous region of the right frontal bone to the periorbital area (white arrows). The lesion is extending into the intradiploic space, creating a foramen (black arrows). In the three-dimensional (3D) volumetric rendering CT (C), remodeling of the frontal bone is observed, creating a foramen (black arrowheads).
Dermoid cysts are cystic lesions, typically located along the midline, and are lined with squamous epithelium. They are benign lesions originating from the surface ectoderm.1,2 Dermoid cysts typically present with a complaint of painless swelling. 3 Dermoid cysts are slow-growing, rare congenital lesions. Although dermoid cysts can occur in various parts of the body, those in the head and neck region are typically located around the eyebrows or in the frontotemporal area. 4 Dermoid cysts can present as painless masses, but they may also be seen as palpable bone defects in some cases. 3 The differential diagnoses include dermoid cyst, Langerhans cell histiocytosis, eosinophilic granuloma, cavernous hemangioma, and fibrous dysplasia. 4 The patient group most commonly affected is children. Dermoid cysts are congenital in nature and typically present with symptoms in the early years of life. These cysts are usually located along the anterior fontanel or cranial sutures. Dermoid cysts acquire a cystolipomatous appearance by producing keratin and fat. The continued production of these substances can increase the cystic pressure, leading to a mass effect or may result in spontaneous rupture. These conditions can cause erosion of the cranial bones and/or expansion of the epidural space. 2 Because their growth is usually slow, dermoid cysts cause bone remodeling, resulting in swelling. While dermoid cysts are typically painless, the lesion in our patient, which caused intradiploic diastasis, was responsible for unilateral temporal pain. In our case, we demonstrated an intradiploic dermoid cyst as a rare cause of temporal pain. In pediatric patients presenting with unilateral temporal pain, an intradiploic dermoid cyst should be considered as a rare possibility.