
Abstract
Significant statement
Congenital middle ear cholesteatoma is a benign but destructive condition involving the abnormal proliferation of keratinizing squamous epithelium. 1 The treatment of congenital cholesteatoma typically involves surgical removal to prevent complications. In the early stages, removal is relatively easy; however, if they occur multiple in the middle ear cavity, as in this case, there may be a risk of missing the other one.
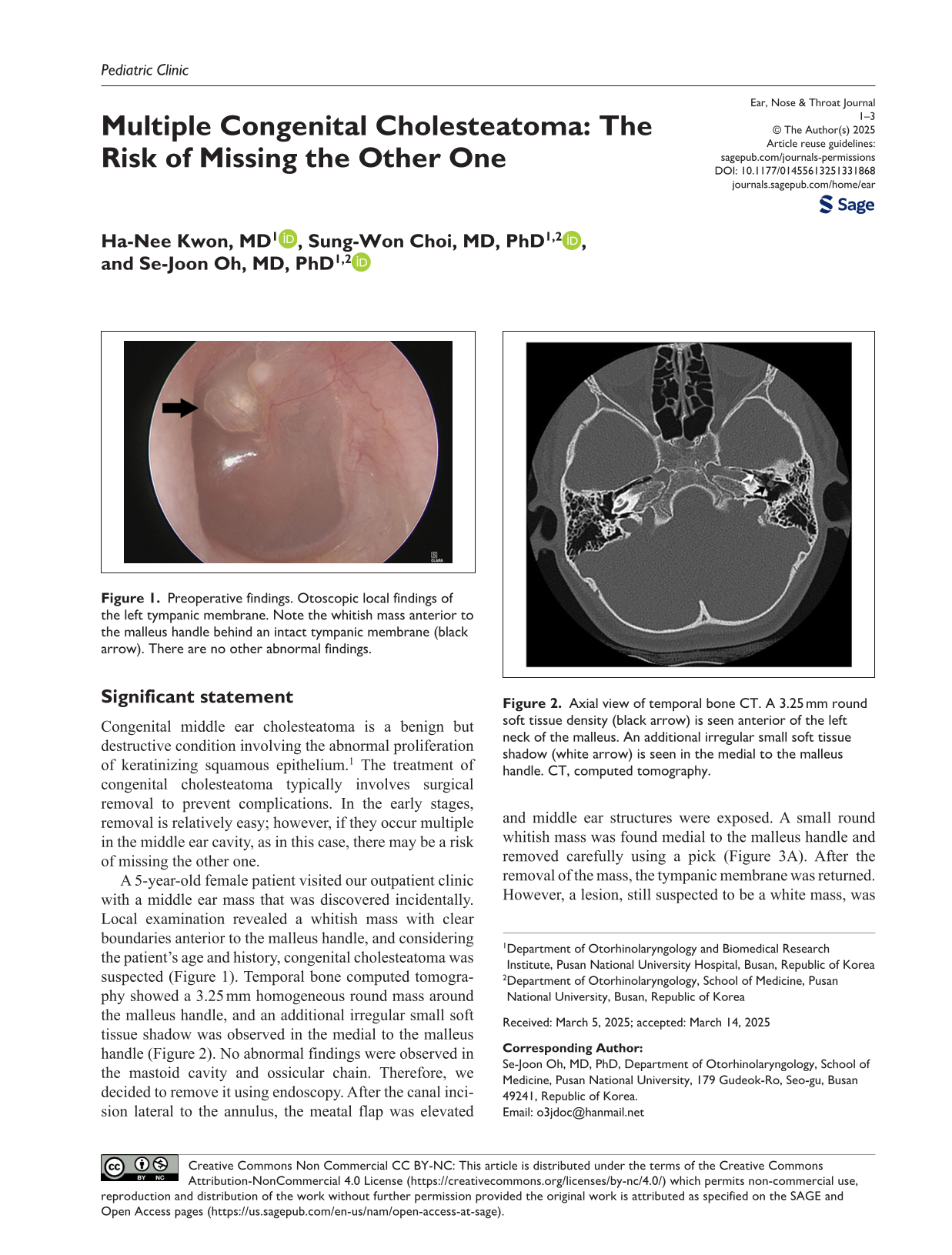
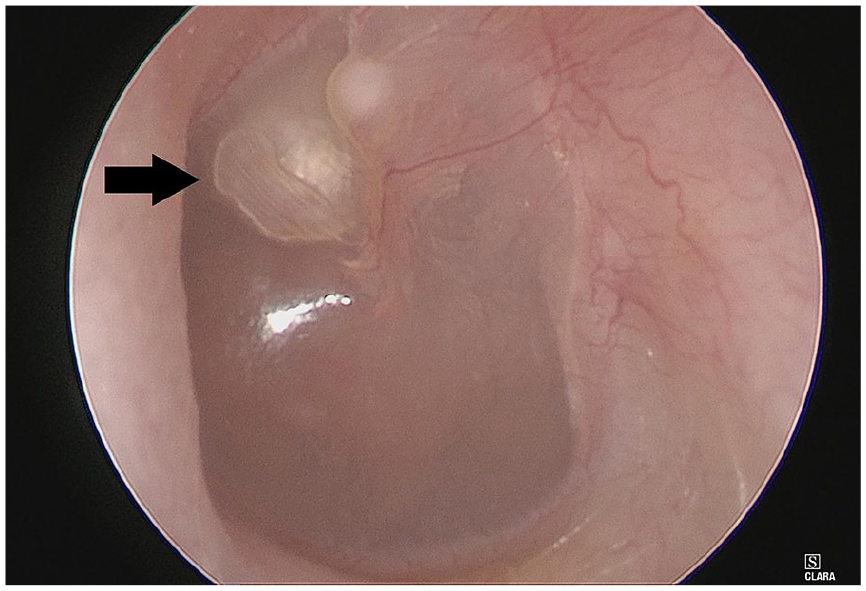
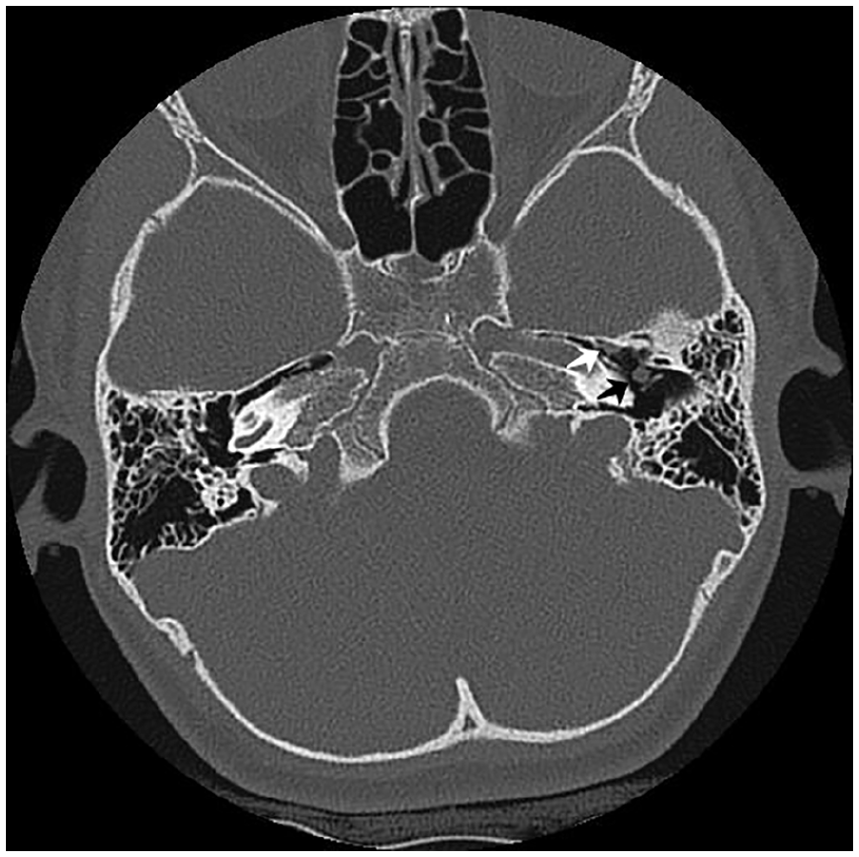
A 5-year-old female patient visited our outpatient clinic with a middle ear mass that was discovered incidentally. Local examination revealed a whitish mass with clear boundaries anterior to the malleus handle, and considering the patient’s age and history, congenital cholesteatoma was suspected (Figure 1). Temporal bone computed tomography showed a 3.25 mm homogeneous round mass around the malleus handle, and an additional irregular small soft tissue shadow was observed in the medial to the malleus handle (Figure 2). No abnormal findings were observed in the mastoid cavity and ossicular chain. Therefore, we decided to remove it using endoscopy. After the canal incision lateral to the annulus, the meatal flap was elevated and middle ear structures were exposed. A small round whitish mass was found medial to the malleus handle and removed carefully using a pick (Figure 3A). After the removal of the mass, the tympanic membrane was returned. However, a lesion, still suspected to be a white mass, was observed under the tympanic membrane (Figure 3B); therefore, further dissection was performed anterior to the malleus handle, and another white mass was observed near the entrance of the Eustachian tube and removed (Figure 3C). There were no intraoperative and postoperative complications, and the patient showed excellent healing.
Preoperative findings. Otoscopic local findings of the left tympanic membrane. Note the whitish mass anterior to the malleus handle behind an intact tympanic membrane (black arrow). There are no other abnormal findings.
Axial view of temporal bone CT. A 3.25 mm round soft tissue density (black arrow) is seen anterior of the left neck of the malleus. An additional irregular small soft tissue shadow (white arrow) is seen in the medial to the malleus handle. CT, computed tomography.
Interoperative endoscopic findings. (A) A small whitish mass medial to the neck of the malleus. (black arrow) (B) Otoscopic finding shows that there remains a whitish mass lesion (white arrow) after removal of the first whitish mass. (C) Another whitish mass (white arrow) anterior to the malleus handle.
The incidence of congenital cholesteatoma varies, occurring in approximately 1 in 10,000 to 15,000 live births. It accounts for approximately 2%-24% of middle ear cholesteatoma, depending on the population studied. 2 The condition is typically diagnosed in early childhood, between the ages of 2 and 5, during a routine ear examination or if symptoms, such as hearing loss, are investigated. The Potsic staging system is commonly used to classify the stages of congenital cholesteatoma; stage I involves the disease being limited to a single quadrant, stage II indicates the presence of cholesteatoma in multiple quadrants, but without affecting the ossicles or extending into the mastoid, stage III includes ossicular involvement without mastoid extension, and stage IV is characterized by mastoid diseases. 3 With the advances in endoscopic ear surgery, endoscopy could be conducted for congenital cholesteatoma in the early stage, such as small-to-medium-sized cholesteatomas, which did not extend into the mastoid or antrum.
There have been a few cases of congenital cholesteatoma reported on both sides.4,5 However, multiple congenital cholesteatoma cases have not yet been reported. This case is significant not because it is rare, but because there is a possibility that a residual cholesteatoma may still remain clinically. A residual cholesteatoma observed through the tympanic membrane may be unclear immediately after the first cholesteatoma removal; thus, although it is believed to have been successfully removed, residual cholesteatoma may remain. Therefore, we must carefully examine the less visible areas of the middle ear, particularly the entrance of the Eustachian tube, epitympanum, and sinus tympani, which becomes easier by endoscopy.
Congenital cholesteatoma usually occurs as a single mass, but 2 completely separate cholesteatomas can occur in different locations. Therefore, although the exact extent of the cholesteatoma should be determined through careful otoscopic examination and imaging studies preoperatively, it is equally important to thoroughly check for any residual cholesteatoma perioperatively to ensure no remnants remain in the tympanic cavity.