
Abstract
A migratory fishbone is not a rare case in otorhinolaryngology clinics in Asia. Deep neck infection is a common complication, and several cases of preoperative vocal cord paralysis have been reported. However, postoperative vocal cord paralysis after the retrieval of a fishbone penetrating the recurrent laryngeal nerve has not been documented. Herein, we present such a case to improve related knowledge and emphasize the importance of preoperative evaluation, the prediction of prognosis, and the risk of postoperative unrecoverable vocal paralysis.
Introduction
Due to eating habits, cases of fishbone foreign bodies in the neck are commonly encountered in otolaryngology clinics in Asia. Migratory fishbones can cause various complications such as esophageal perforation, neck abscess, and carotid vessel and recurrent laryngeal nerve injury. In severe cases, it can be life-threatening.1,2 Several cases of preoperative vocal cord paralysis have been reported. However, postoperative vocal cord paralysis after the retrieval of a fishbone penetrating the recurrent laryngeal nerve has not been documented. Herein, we report a case of postoperative vocal cord paralysis after the retrieval of a fishbone penetrating the recurrent laryngeal nerve.
Case Report
A 45-year-old female patient presented to our institution due to symptoms of abnormal sensation of a foreign body for >1 year and aggravating odynophagia for 1 month after a history of accidentally swallowing a fishbone. Initial gastroscopy and fiberoptic laryngoscopy at a local clinic did not identify significant findings. The patient presented with pain on the left side of the neck, which was effectively managed with intermittent antibiotic therapy. However, she did not exhibit fever, evident local redness, and swelling. She then visited the Department of Otolaryngology at our hospital. Neck computed tomography (CT) scan revealed a strip-shaped high-density shadow measuring approximately 1.5 cm in the left tracheoesophageal groove with a slightly swollen esophageal wall in the localized area, and a blurred fat space around it (Figure 1). A migratory fishbone was highly suspected. The preoperative fiberoptic laryngoscopy findings were normal. The patient underwent assessment using the transverse cervical approach to explore the foreign body under general anesthesia. Diffuse adhesion from the right lobe of the thyroid gland to the left carotid sheath was noted. After the left lobe of the thyroid gland was elevated, a swollen recurrent laryngeal nerve at the segment entering into the throat was observed. The inferior pharyngeal muscle over the cricoid joint was cautiously dissected, and the fishbone with a length of approximately 15 mm was withdrawn from the swollen recurrent nerve and surrounding tissue. Granulation tissue was found in the fishbone bed after the fish bone was extracted (Figures 2 and 3). Pathologically, the granulation tissue presented with hyperplasia with inflammatory exudation and necrosis (Figure 4). The symptoms of foreign body sensation and odynophagia, except for a slight hoarseness of voice, subsided several days after the surgery. Re-examination via laryngoscopy revealed left vocal fold fixation, and the restoration of vocal cord movement did not reach after 1 month of surgery. Despite the presence of slight hoarseness, the voice of the patient was gradually improving.
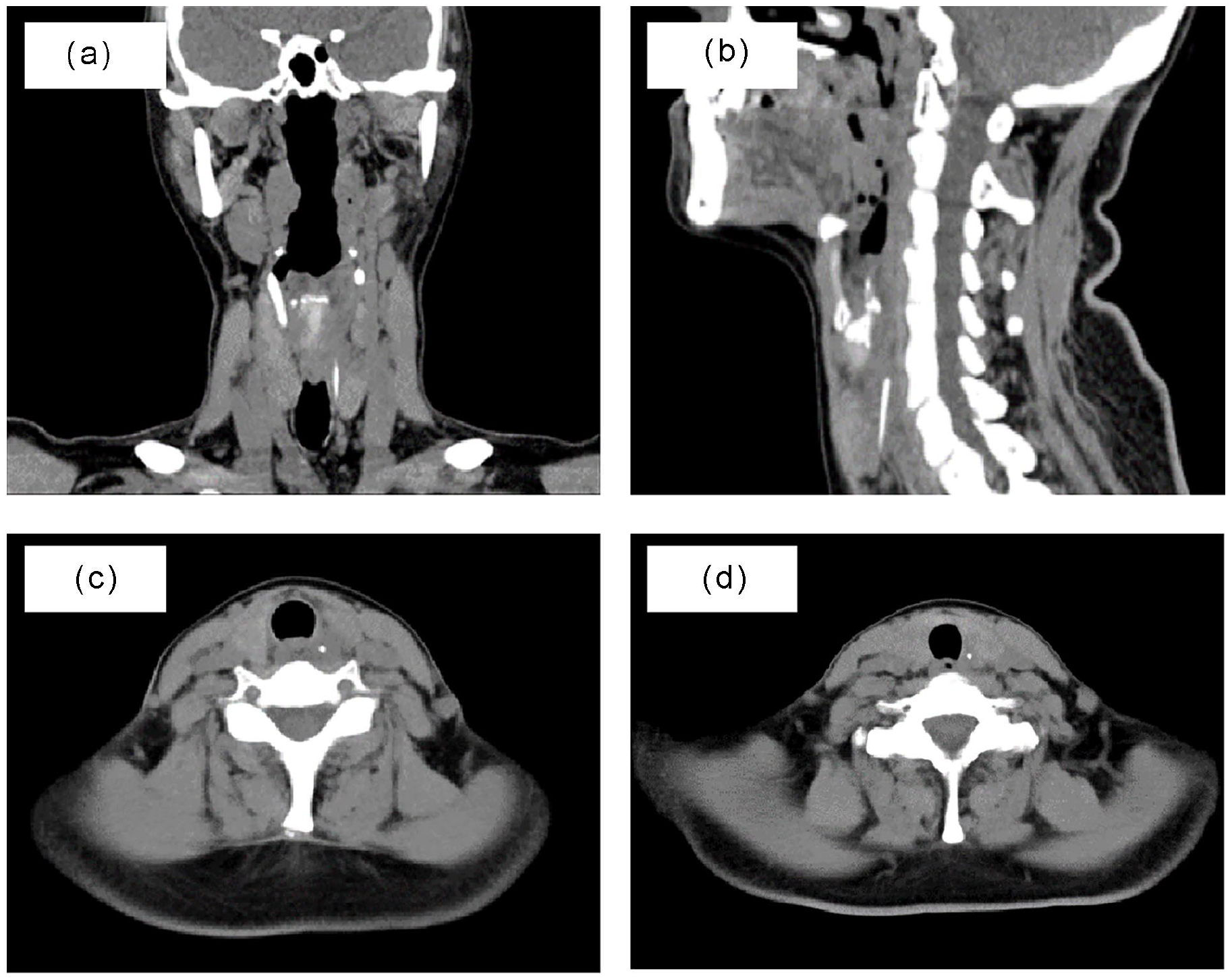
CT scan image of the neck shows a strip-shaped high-density shadow in the left tracheoesophageal groove in the coronal view (a), sagittal view (b), axial view near the swollen esophageal entrance (c), and axial view slightly farther from the esophageal entrance, which revealed a less swollen soft tissue (d).
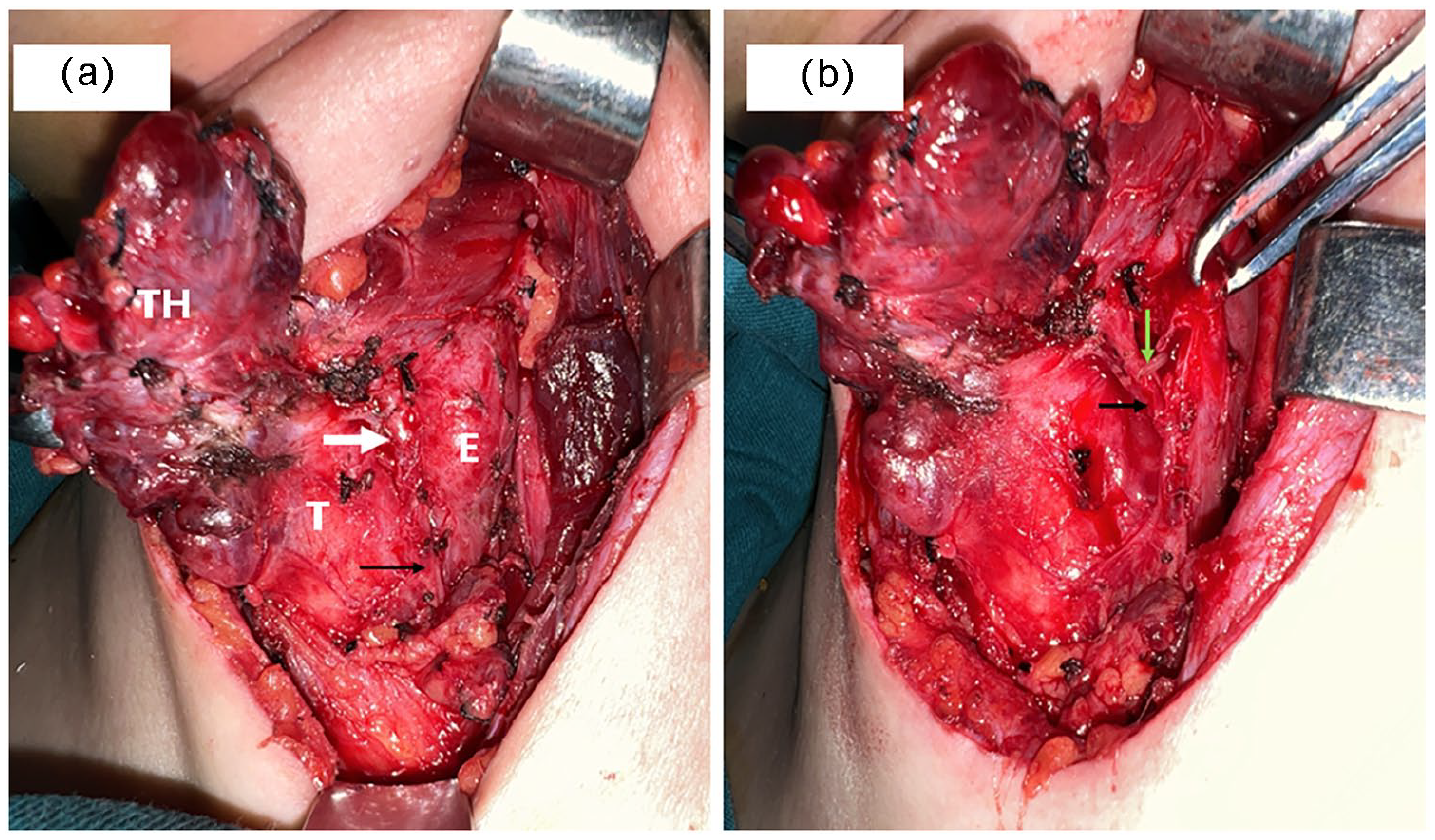
Surgical field after the left thyroid lobe (TH) was elevated. (a) The fishbone was embedded within the swollen recurrent laryngeal nerve and near the esophageal wall (white arrow—E: esophagus, T: trachea; black arrow—the recurrent laryngeal nerve with a normal appearance). (b) Exposed fishbone (green arrow) and a broken, swollen recurrent laryngeal nerve peritoneum (black arrow).
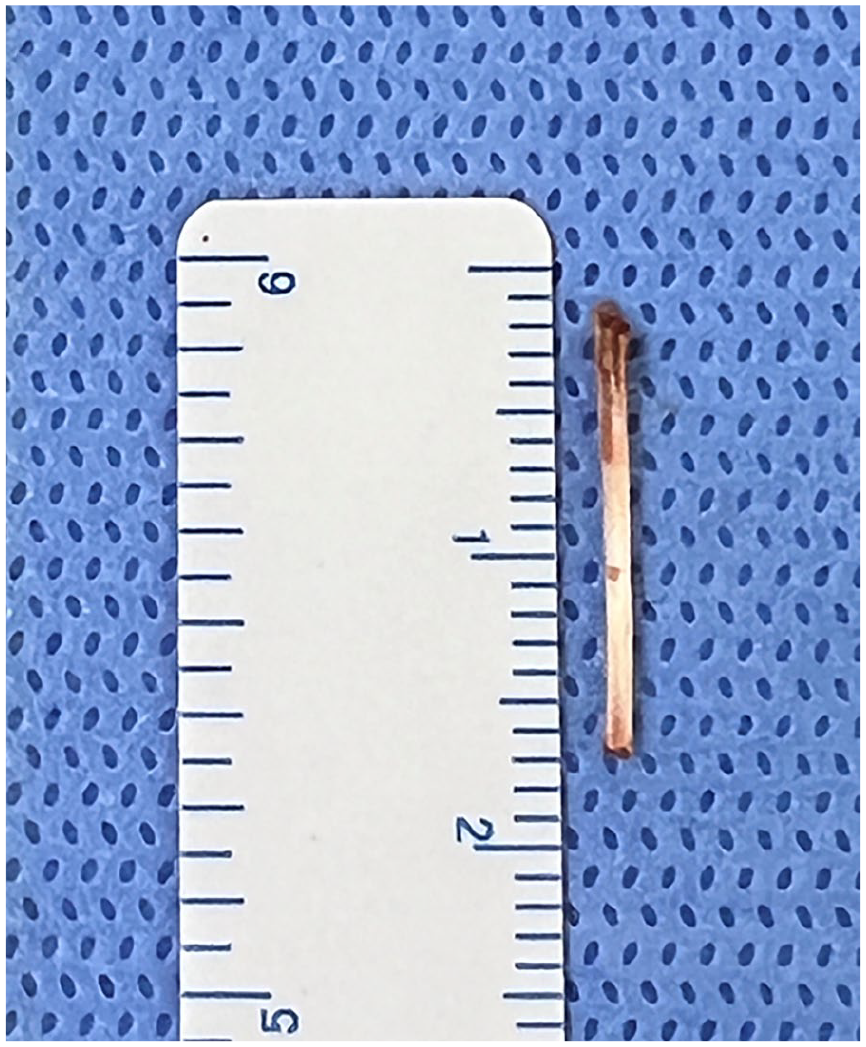
The length of the fishbone was 1.5 cm.
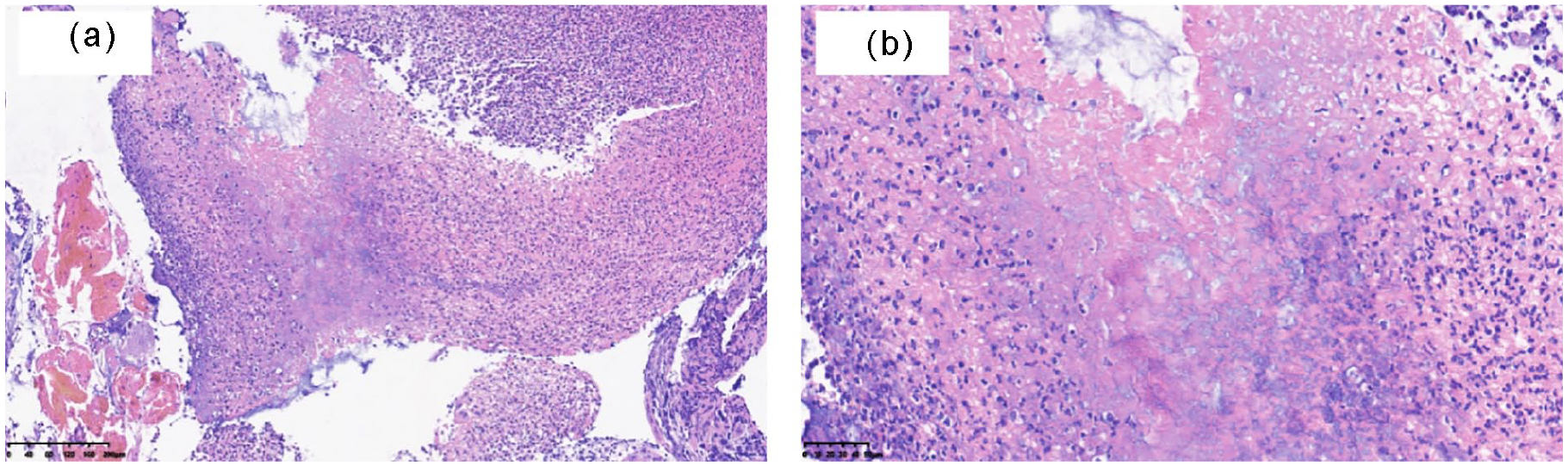
Pathological findings revealed granulation tissue hyperplasia with inflammatory exudation, necrosis, and infiltration of plasm cells and lymphocytes (Figure 4a and b; hematoxylin and eosin staining: (a) magnification × 100, (b) magnification × 300).
Discussion
Fishbones, which are considered upper digestive foreign bodies, are commonly located in the tonsil, tongue base, vallecula, pyriform fossa, and even the esophagus, where they can be easily visualized, located, and eliminated via specialized procedures such as laryngoscopy and gastroscopy. 3 However, a migratory fishbone is not rare as it can be caused by the patient’s swallowing movements, esophageal peristalsis, and iatrogenic management. The migratory fishbone penetrates the upper gastrointestinal tract and enters the paralaryngeal space, retropharyngeal space, periesophageal space, and superior mediastinum resulting in abscess and recurrent inflammation. Furthermore, it can puncture the large artery leading to hemorrhage. In general, if the recurrent laryngeal nerve is involved, vocal palsy can occur. This is because the recurrent laryngeal nerve is the most vulnerable nerve when injured. To date, some studies have reported several cases of preoperative vocal cord paralysis.4 -6 However, postoperative vocal cord paralysis after the retrieval of a fishbone penetrating the recurrent laryngeal nerve has not been documented. In fact, recurrent nerve injury cannot be absolutely prevented in this case even though an incision was made in the inferior pharyngeal muscle to retrieve the fishbone without further damaging the nerve. This situation can also be observed during trauma and in other conditions such as recurrent or local advanced thyroid carcinoma, recurrent pharyngeal fistula, and associated scar adhesion. For example, in locally advanced papillary thyroid carcinoma, the recurrent laryngeal nerve can be involved. However, the nerve can still function well. 7
Positioning of the foreign body is challenging to perform and is the key to eliminate it before and during the surgery. Laryngoscopy and radiographic examinations, such as lateral neck radiography, neck CT scan, and ultrasonography, are commonly performed and required. Laryngoscopy may not identify evident abnormalities in the migratory foreign bodies. Detecting a fishbone in the neck using radiography is challenging due to limitations in two- or three-dimensional positioning. In addition, it may have a low sensitivity to fishbone of low mineralization degree. Ultrasonography and CT scans are more advantageous for diagnosing migratory foreign bodies in the neck. The combination of the two methods can significantly improve diagnostic accuracy. 8
Not all vocal cord movements can completely recover within 1 to 3 months after fishbone surgery. 6 A review of the relevant literature has shown that the mechanisms of fishbone-induced vocal fold paralysis can be categorized into mechanical articular fixation, direct neuropathy of the recurrent laryngeal nerve, or indirect neuropathy of the recurrent laryngeal nerve secondary to inflammation. 5 In this case, the recurrent laryngeal nerve was perforated to some extent, and the patient still had normal vocal cord movement before surgery. Hence, the injured nerve still had a normal electro-neuromuscular impulse to innervate the vocal cords. It is not questionable whether or not this surgery should be carried out. Nevertheless, some factors such as the risk of complications should be considered.
Conclusion
Foreign body surgery is not always completely successful. Retrieval of a migratory fishbone penetrating the recurrent laryngeal nerve in the tracheoesophageal groove can result in vocal fold palsy even under full exposure of the cervical segment of the recurrent laryngeal nerve and cautious extraction of the fishbone from a theoretically ideal direction. This emphasizes the need for preoperative communication between physicians and patients to reduce expectations regarding vocal restoration. 9 Furthermore, patients must undergo long-term follow-up.
Footnotes
Ethical Considerations
Ethical approval for reporting this case was obtained from the Biomedical Ethics Review Committee of West China Hospital, Sichuan University (approval no. 2024-1530).
Consent to Participate
A written informed consent for the conduct of this study, publication of this article, and use of their images was obtained from the patient.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Due to the nature of this research, the participants of this study did not agree to share their data publicly. Thus, supporting data are not available.