
Abstract
Introduction:
Tracheotomy is a common procedure in otorhinolaryngology, aimed at bypassing upper airway. Various surgical techniques exist, including the Bjork flap method and the window technique, each with distinct advantages. The study aimed to compare early complications between these techniques.
Materials and Methods:
This retrospective study analyzed 164 patients over 18 years old who underwent tracheotomy. Patients were divided based on the technique used: Bjork flap (28.7%) or window (71.3%). Data collected included demographics, comorbidities, and early complications within 7 days postsurgery.
Results:
The median age was 68 years, with no significant age difference between the techniques. The Bjork technique involved ligation of the thyroid isthmus in 66.0% of cases versus 20.5% in the window technique (P < .001). Early complications occurred in 69.1% of patients: 12.8% for Bjork and 7.7% for the window technique, with no significant difference (P = .370). Types of complications varied, with cannula displacement, surgical site infection noted in Bjork cases and bleeding, subcutaneous emphysema, false pouch formation, and pneumothorax in window cases.
Conclusion:
Although complication rates are similar, subcutaneous emphysema, false pouch formation and pneumothorax have been seen in the window technique. This may indicate that the flap sutured to the skin in the Bjork technique may be useful in preventing the formation of false passage.
Introduction
Tracheotomy is one of the most commonly-performed procedures in the field of otorhinolaryngology. During tracheotomy, a surgical opening is created in the anterior tracheal wall to bypass the upper respiratory tract and the larynx to ensure the safety of the lower respiratory tract. The indications for tracheotomy are upper airway obstruction, prolonged endotracheal intubation, bronchopulmonary toilet, and airway protection in head and neck cancer surgery. Various techniques have been defined for tracheal incisions in tracheotomies. These are horizontal incision between the tracheal rings, vertical incision, cartilage window removal, inferior-based cartilage flap (Bjork), and percutaneous methods.1,2 Open surgical methods were popularized by Chevalier Jackson in 1909. 3 Each technique has advantages and disadvantages.
Bjork flap was first described in 1960. 4 In this method, a U-shaped incision is made through the second, third, or fourth tracheal ring. The flap pedicle is located in the inferior part of the trachea. The U-shaped tracheal flap is sutured to the skin or subcutaneous tissue, creating a connection between the skin and the tracheal lumen. This approach is considered to reduce the likelihood of tube dislodging from the trachea, causing false passage or early-tube displacement.
Tracheotomy complications are divided into intraoperative, early, and late stages. Complication rates ranging from 5% to 40% have been reported in the literature.5,6 The early complications develop mostly within the first 7 days. Intraoperative and early complications include bleeding, thyroid injuries, apical pleural damage, pneumothorax, airway obstruction, false passage formation, and cannula/tube displacement.
This study aimed to compare the early complications of the window tracheotomy and Bjork flap techniques. Our hypothesis was that since the tracheal cartilage is sutured to the skin in the Bjork flap technique and there is no gap between the tracheal lumen and the skin, the risk of false passage may be lower during tube replacement or follow-up of the patient.
Materials and Methods
Following the Institutional Ethical Board approval (2024-TBEK 2024/02-05, Number: E-31234050-514.99-266782974), this study was conducted retrospectively on 164 patients >18 years of age who underwent tracheotomy in the ear, nose, throat, head, and neck surgery department of a tertiary training and research hospital between December 2020 and December 2024. Tracheotomy was performed in the operating room for all patients. The open surgical tracheotomy began with a horizontal skin incision approximately 2 cm above the sternal notch. After passing through the platysma, the raphe of the stretch muscles was found and dissected at the midline, and the muscles were retracted laterally. At this stage, the thyroid gland isthmus was observed.
The window technique or the Bjork flap technique was performed in all patients. In the Bjork flap technique, a U-shaped cartilage flap with an inferior base, including the second and third tracheal rings, was designed and sutured to the skin (Figure 1). In the window technique, 2 cartilage rings were removed from the trachea and an opening was created in the anterior wall of the trachea. In some cases, the thyroid isthmus was cut and ligated depending on its location.
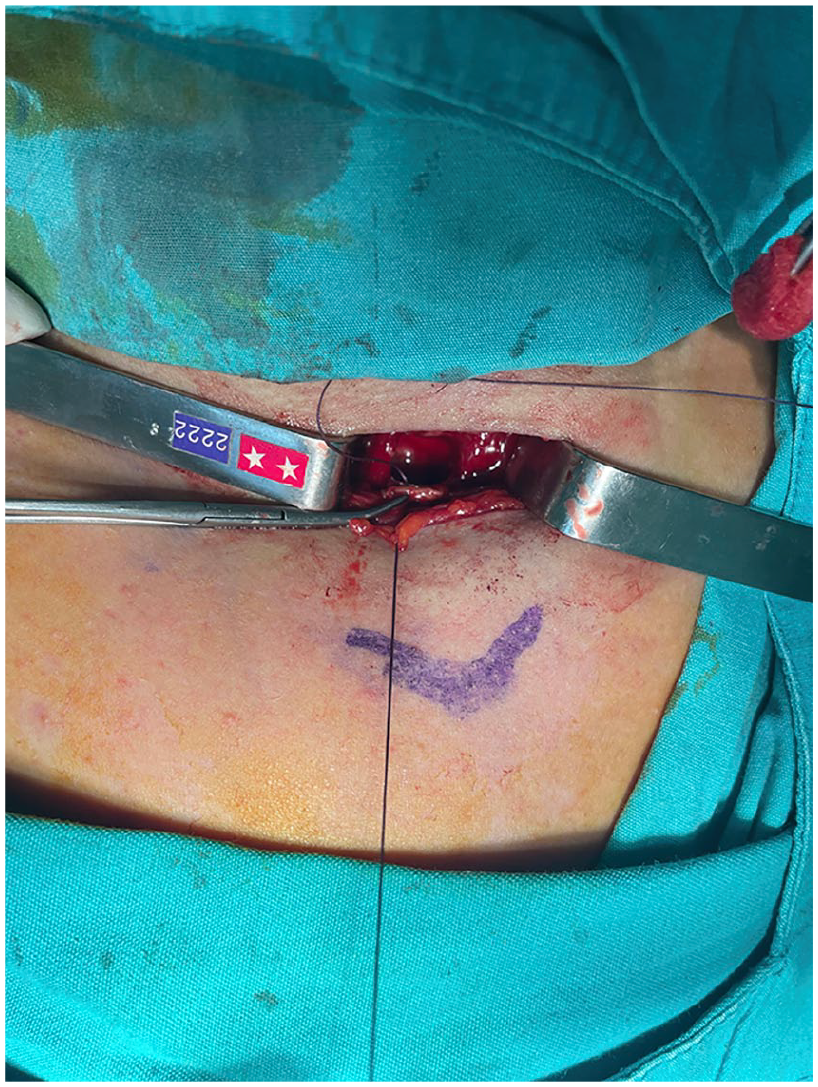
Bjork flap was sutured to the skin.
In the Bjork flap technique, the thyroid isthmus is ligated more frequently to increase the field of view of the trachea and the flap is sutured to the skin, so the operation time is slightly longer than that in the window technique (Figures 2 and 3).
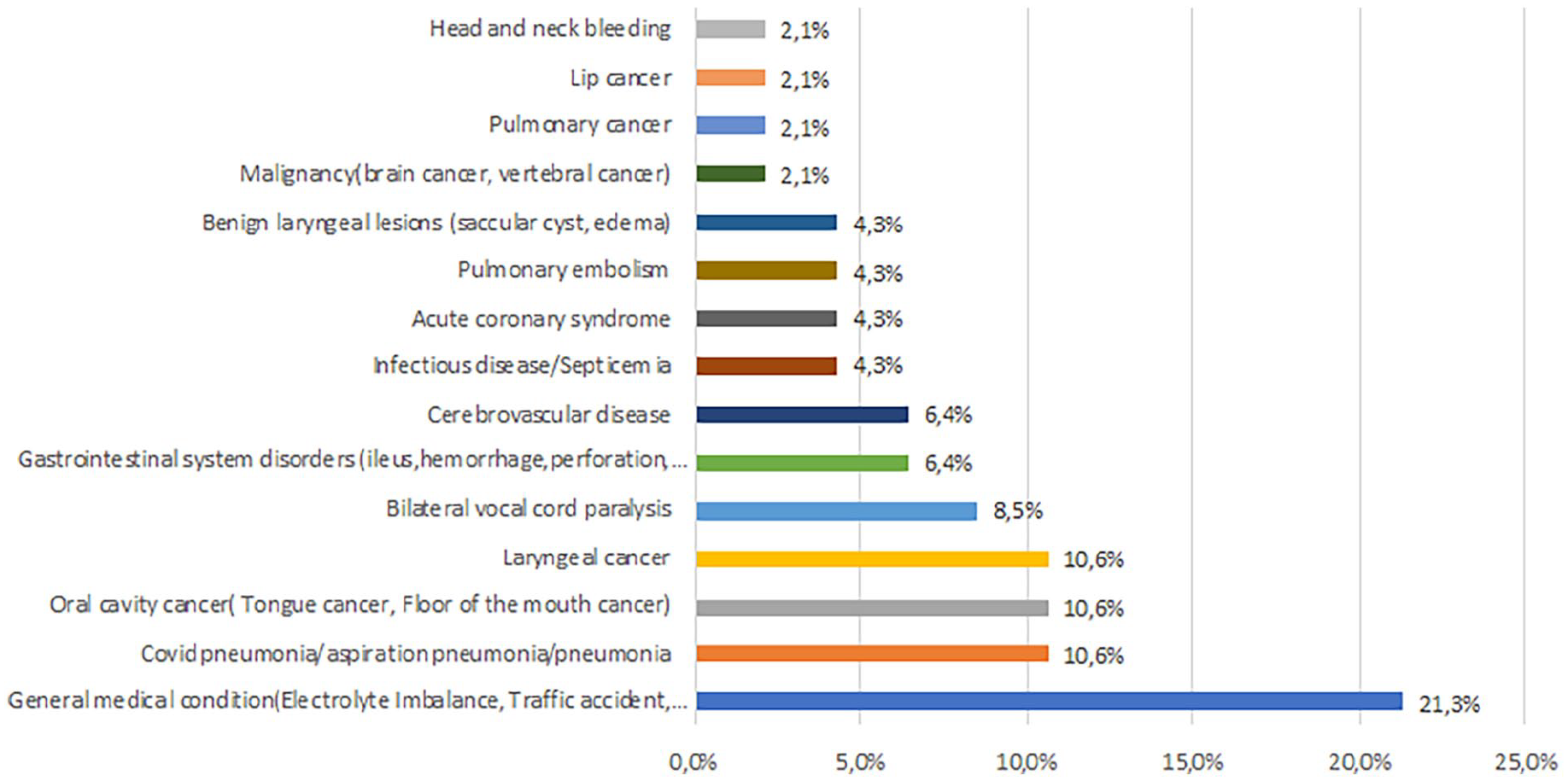
Detailed tracheotomy indications for those undergoing the Björk flap technique.
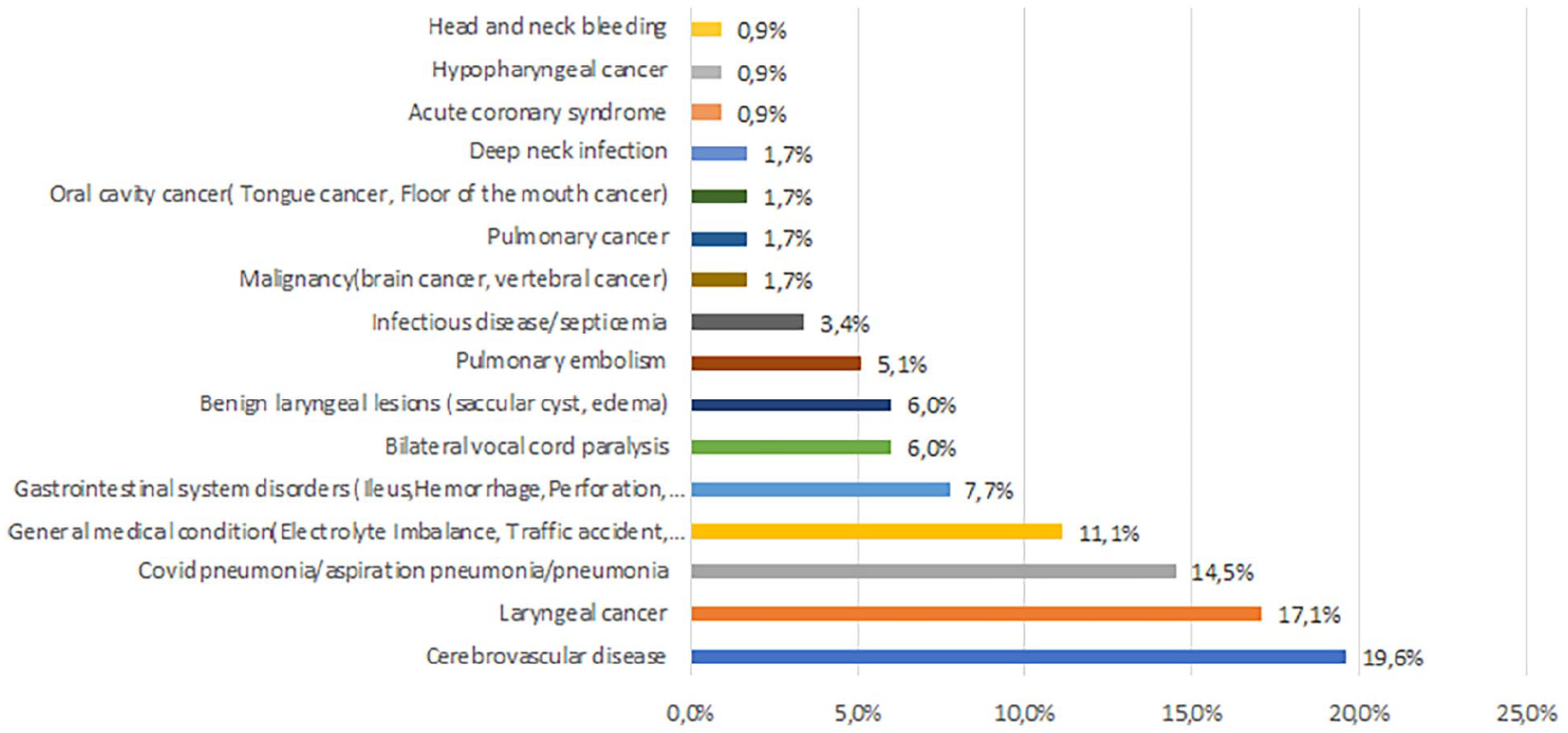
Detailed tracheotomy indications for those undergoing the window technique.
In our clinic, 2 different tracheotomy techniques are applied. Since the Bjork flap technique has been used in our clinic for the last 2 years, asymmetry has emerged between the numbers. The choice of technique varied according to the surgeon’s decision.
The patients’ age, sex, comorbidities, tracheotomy indications, the use of anticoagulant agents, and thyroid isthmus status were recorded. Early complications that developed within 7 days after surgery were recorded.
Statistical analyses were performed using the SPSS software version 25, (IBM, USA). The Kolmogorov-Smirnov analysis was used to determine whether the variables were normally distributed. Descriptive analyses were presented using median, minimum, and maximum values or percentages (number). The chi-squared test or Fisher’s exact test (when the values observed in the cells did not meet the assumptions of the chi-squared test) was used to compare the proportions in different groups. The Mann-Whitney U test was used to compare the variable measured between the groups. The significance level was accepted as P < .05.
Results
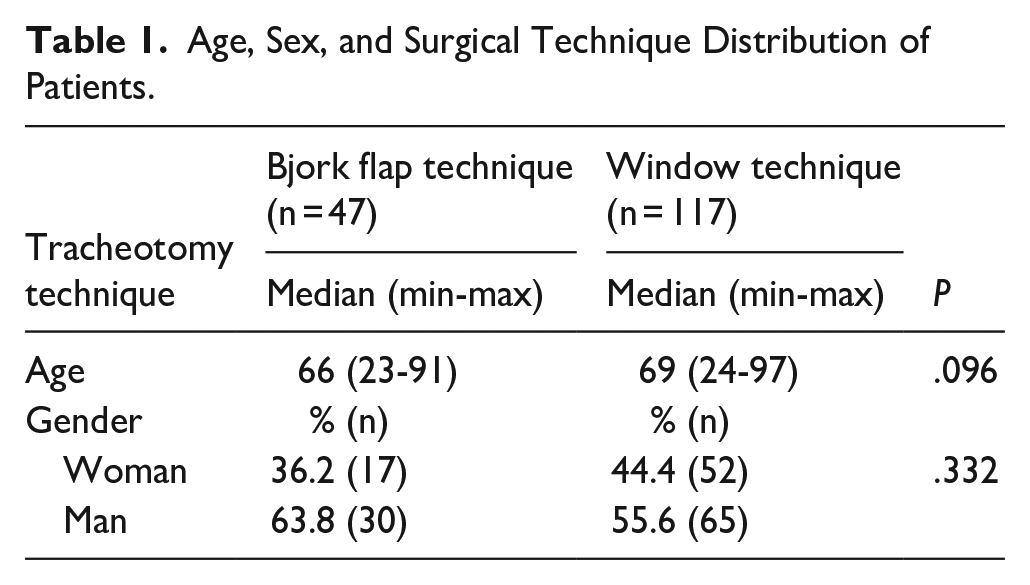
In total, 164 patients were included in this study. A total of 57.9% (n = 95) of the patients were male, and the median age was 68 (minimum value: 23, maximum value: 97) years. The Bjork flap technique was applied in 28.7% (n = 47) of the cases, and the window technique was applied in 71.3% (n = 117). The age and sex distributions of the patients who underwent Bjork and window techniques are presented in Table 1. Although the median age of 117 patients that underwent the window technique was higher than those who underwent the Bjork technique, there were no significant differences between the groups (P = .096) (Table 1).
Age, Sex, and Surgical Technique Distribution of Patients.
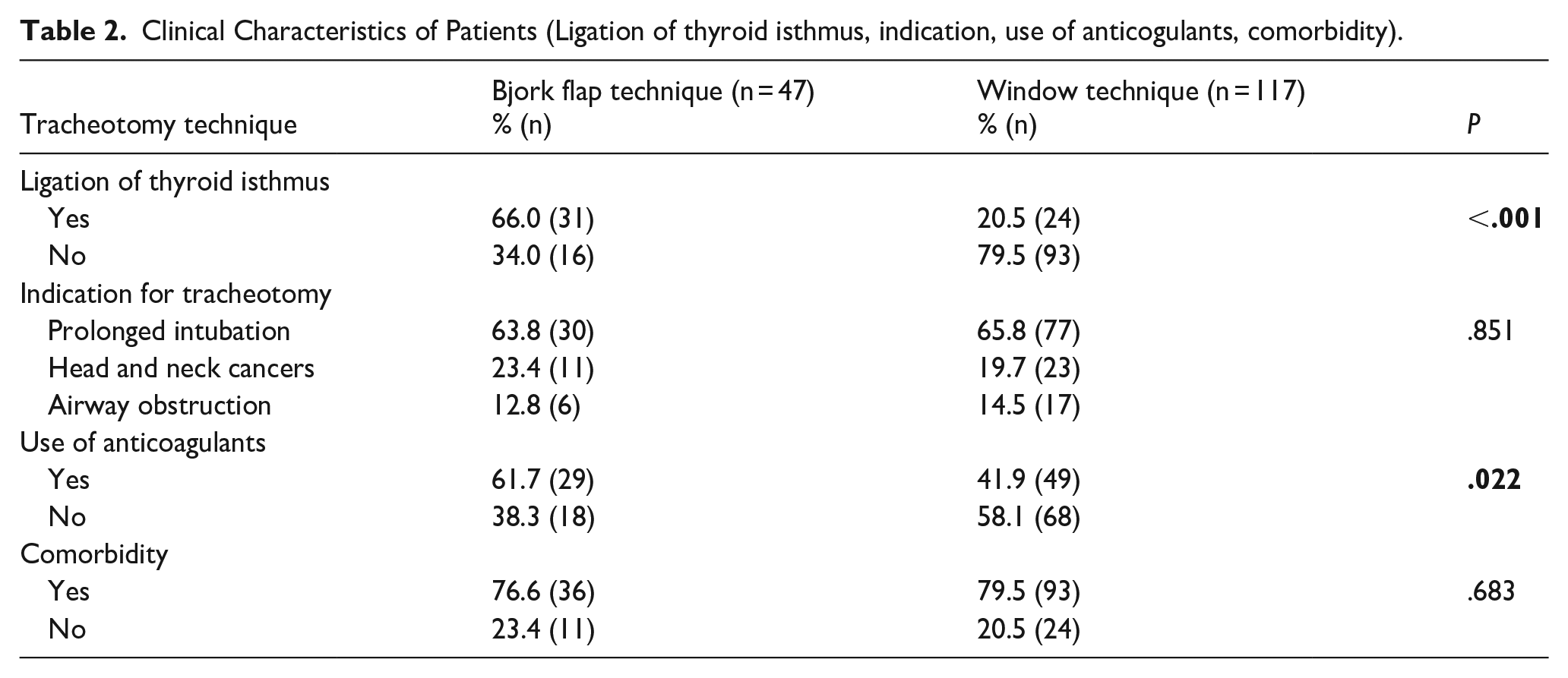
The thyroid isthmus was ligated in approximately 66.0% (n = 31) of the cases using the Bjork flap technique compared with approximately 20.5% (n = 24) of the cases using the window technique, and the difference was significant (P < .001). There was accompanying chronic disease in 78.7% (n = 129) of the cases. Ninety-three (79.5%) of those who underwent the window technique and 36 (76.6%) of those who underwent the Bjork technique had additional chronic diseases (Table 2). Hypertension, diabetes mellitus, and coronary artery disease were the 3 most common chronic diseases in the study group (49.4%, 29.3%, and 28.0%, respectively).
Clinical Characteristics of Patients (Ligation of thyroid isthmus, indication, use of anticogulants, comorbidity).
Among patients who underwent tracheotomy due to prolonged intubation, the median duration of intubation was 18 days in the cases in which the Bjork flap technique was applied and 16 days in the cases in which the window technique was applied. However, the difference between the groups was not statistically significant (P = .509). Complications developed in the early period in 9.1% (n = 15) of the patients. Early complications were observed in 6 patients (12.8%) who underwent the Bjork flap technique and in 9 patients (7.7%) who underwent the window technique (P = .370). Tube displacement was observed in 3 of the 6 cases and surgical site infection (n = 2), tracheotomy tube obstruction (n = 1) developed in 3 cases in which the Bjork flap technique was performed. Complications occurred in 9 cases in which the window technique was performed. These included tube displacement (n = 2), false pouch formation (n = 2), subcutaneous emphysema and pneumothorax (n = 2), bleeding (n = 1), infection (n = 1), and tracheoesophageal fistula (n = 1). There was no difference in early complications between the 2 groups (Table 3).
Distribution of Early Complications.
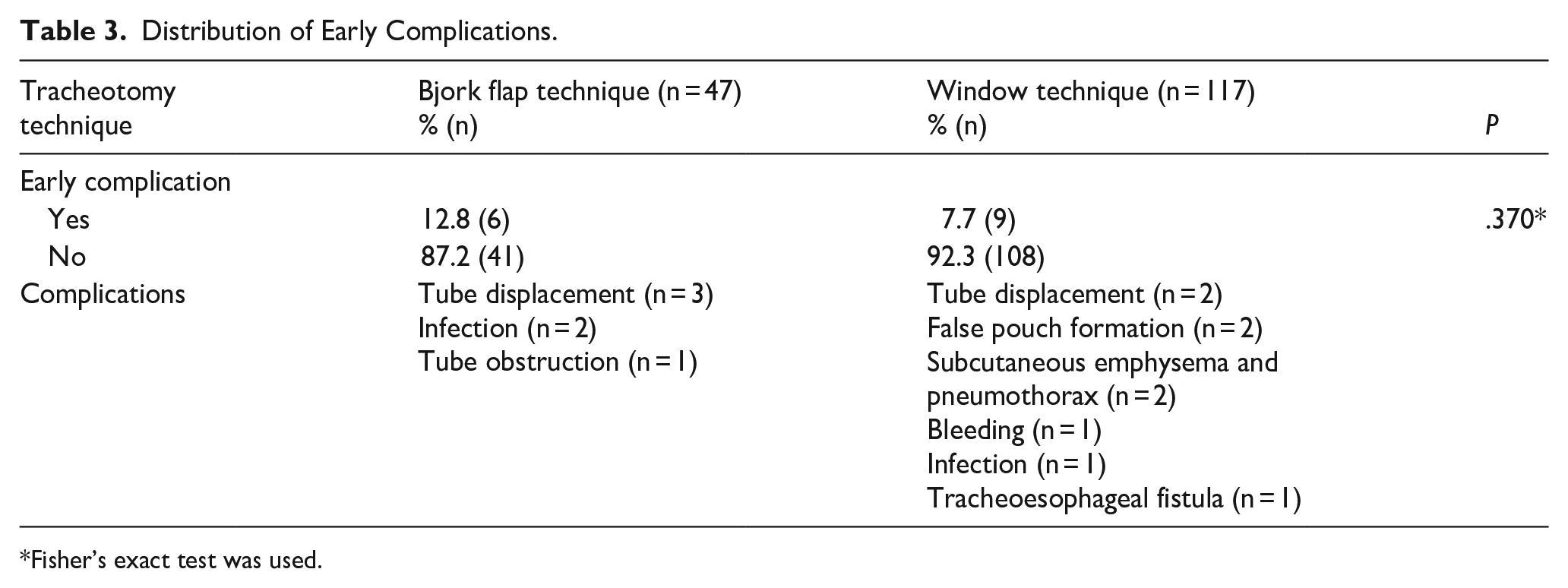
Fisher’s exact test was used.
Discussion
In a study comparing 30 patients with the Bjork flap and 30 incision tracheotomy patients, Chauhan et al 7 reported that early and late complications were less frequent with the Bjork flap method. They stated that intraoperative bleeding was significantly higher with the Bjork flap than with the traditional method. Postoperative bleeding was not observed in the Bjork group, while it was present in 26.7% of cases using the traditional method. Postoperative bleeding was not observed in our patients who underwent the Bjork flap method. This may be because the thyroid gland was ligated more frequently in this group of patients.
In their study evaluating 217 tracheostomy patients, Kennedy et al 8 applied the Bjork flap technique in 104 patients (47.9%) and the window technique in 113 patients. They applied the Bjork flap mainly to patients with a high body mass index, those who needed ventilator support, and patients with stroke. The window technique has been applied mainly to patients with a history of neck dissection or those who have received radiotherapy to the neck. They found no differences between postoperative bleeding, return to the operating room, and days of decannulation. The condition most frequently associated with postoperative bleeding was thrombocytopenia. In this study, the Bjork flap method was applied more frequently in patients with a high body mass index.
Janik et al 9 divided patients who underwent tracheostomy using the Bjork flap technique into 2 groups. In the first group, the thyroid isthmus was cut and ligated and a high tracheostomy was performed. In the other group (31.4%), the isthmus was retracted and a tracheotomy was performed. The complication rate was 7.7%, and the most common complications were persistent stoma (4.1%) and hemorrhage (2.7%). There was no difference between the 2 groups in terms of complication rates. However, the authors showed that the decannulation rate and the mortality rate were different between the 2 groups.
In another study, 518 patients who had undergone tracheotomy were examined. The Bjork flap was applied to 317 patients, and the incision and up and down suture technique was applied to 201 patients. 5 In half of the patients, the tracheotomy was performed during ablative or reconstructive oncological surgery. It may have been easier to apply these techniques in cases where the neck was opened more widely. There was no difference between the 2 groups in terms of complications, such as tracheal bleeding, infection, mucus plug, pneumothorax, and tracheostomy tube shifting into the false passage. Bleeding was observed in 8 patients, hematoma in 8 patients, pneumothorax in 5 patients, and rapid change of cannula at the bedside due to mucus plug in 3 patients. One patient died from decannulation.
Dislocation of the tracheal lumen of the Bjork flap has been reported to cause obstruction of the airway. 10 However, such complications were not observed in our series.
In a study of 100 patients, early complications related to tracheostomy were found in 53% of the patients. Although a single complication was observed in 35 patients, multiple complications were observed in 18 patients. The most common complications are tube blockage, cannula displacement, and bleeding. The most common tracheal incisions used were vertical (48%), T incision (39%), and Bjork flap (9%). Being <18 years old, performing a tracheostomy due to prolonged intubation, and performing a Bjork flap or vertical tracheal incision were associated with early complications of the tracheostomy. They reported that the Bjork flap increased the risk of early complications by 1.6 times. However, in the study, the number of patients with Bjork flaps was only 9% of the group. 11
In the Bjork flap technique, although the closure of the surgical site after decannulation can be delayed, in particular the decrease in the risk of false passages, an easier change of the tracheotomy tube, and the low risk of stenosis in cases with bulky thyroid disease or other head and neck cancers are important advantages. 12 Di Stadio et al 13 performed tracheotomy with the Bjork method in 23 patients with local anesthesia during the COVID-19 period. In the case they published, a tracheotomy with an inferior-based Björk flap was performed in a patient with giant histiocytic sarcoma in the thyroid gland and COVID-19 pneumonia. They did not ligate the isthmus and retracted it superiorly. In this way, the tracheotomy tube change could be performed more easily.
In the study of Holmes et al 14 in 174 patients, the most frequent indication for tracheostomy was the prolonged intubation group. Other indications were postoperative airway management, respiratory tract obstruction, spinal cord injury, and airway protection and secretion management. In our study, the most common indication was prolonged intubation. In this study, the complication rate was 14.9% in surgery. The most common complications were failed or accidental decannulation (6.96%), bleeding, and infection. In our group of patients, the most common complication was accidental cannula displacement.
Conclusion
In our study, the rates of early-term complications were similar in patients who underwent the Bjork flap and window techniques. However, subcutaneous emphysema, pneumothorax and false pouch formation have been seen, especially as a result of the displacement of the cannula into the false passage, in the window technique. This may indicate that the flap sutured to the skin in the Bjork technique may be useful in preventing the formation of a false passage. Both techniques can be applied to patients, depending on the surgeon’s experience and success. A limitation of our study was its retrospective design.