
Abstract

In 1886 Pierre Marie, a neurologist at La Salpêtrière Hospital in Paris, described 2 patients with severe headaches, visual loss, and enlargement of the limbs and skull which he termed “l'acromégalie.” 1 Within a decade, physicians in Europe and America had observed the relationship between acromegaly and neoplastic enlargement of the pituitary gland at autopsy. The quest for a surgical treatment of pituitary tumors was on.
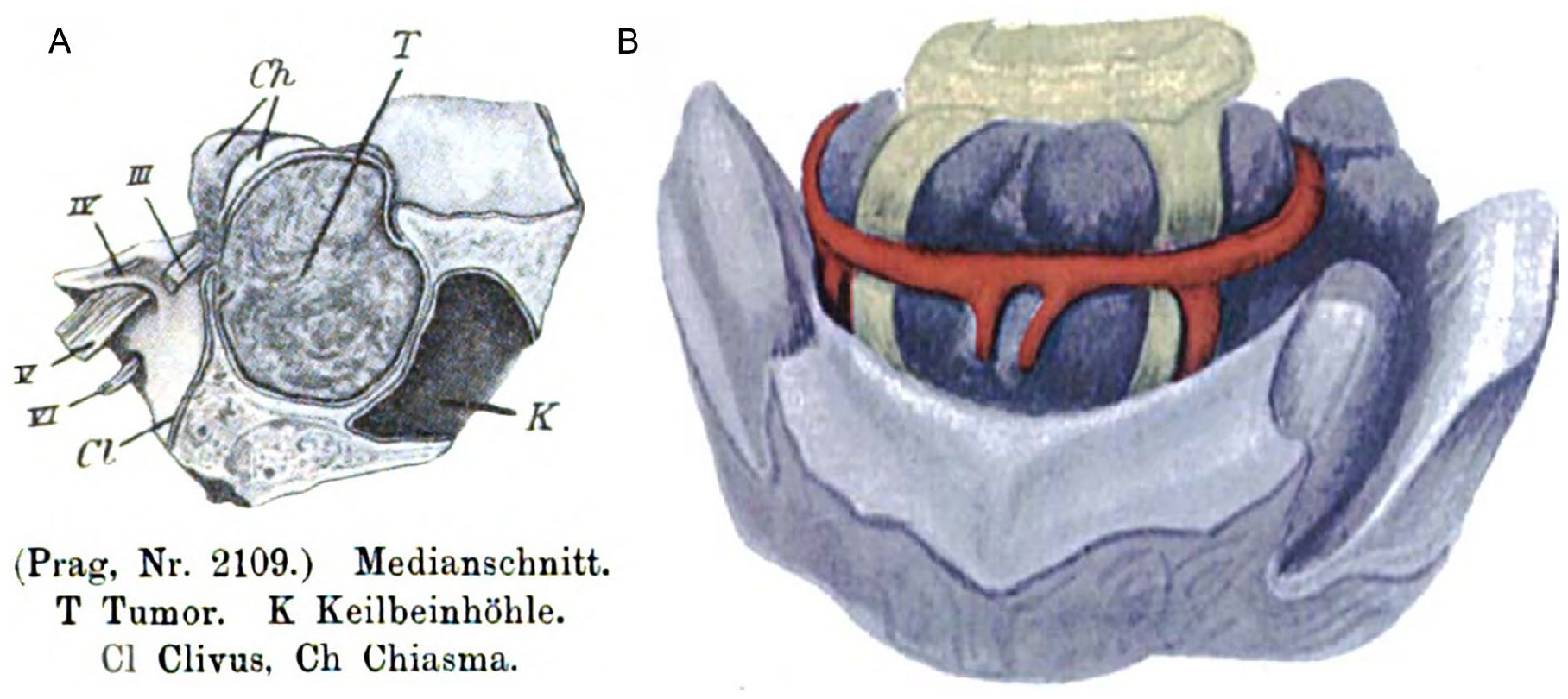
Within 7 years, Caton and Paul 2 of the Liverpool Infirmary had conceived a 2-stage procedure to treat acromegaly for a young woman with severe headache and bitemporal blindness. In the first step, Paul performed a temporal craniectomy to relieve increased intracranial pressure. This decreased the patient’s head pain, but, over the ensuing weeks, her brain herniated through the opening, leaving the tumor inaccessible. At autopsy, a pituitary mass, “the size of a Tangerine orange,” had expanded the sella turcica and projected half an inch above the lesser wings of the sphenoid (Figure 1). Others approached the pituitary fossa through temporal or frontal openings in the skull. Mortality approached 50% and no one was cured.
The prospect of accessing the pituitary through the sphenoid sinus appealed to several surgeons at the turn of the 20th century. In 1907, Hermann Schloffer 3 partially resected a large pituitary adenoma through a lateral rhinotomy with a head mirror and sunlight for illumination. 6 The approach allowed adequate visualization but required resection of nasal septum and turbinates and left a disfiguring facial scar. By this time, Markus Hajek in Vienna had performed exquisite anatomic studies of the paranasal sinuses and described an intranasal, transethmoidal approach to the sphenoid sinus for suppurative disease. In 1910, Hajek’s former student Oskar Hirsch used a 5-stage intranasal approach to decompress a pituitary tumor into the sphenoid. 5 Hirsch later adopted Theodor Kocher’s method of submucous septal resection to reach the sphenoid in a single stage. 7
Harvey Cushing in Baltimore was well acquainted with the rapidly evolving European surgeries. Cushing experimented with transglabellar and middle fossa approaches while refining transsphenoidal surgery. He combined Albert Halstead’s sublabial incision for submucous resection of the septum with Hirsch’s transsphenoidal approach, improving proximal access. Rather than depending on topical cocaine alone, he chose general anesthesia, reducing the risk of the patient reacting to incision of the hypophyseal dura. Cushing devised a sturdy bivalve speculum to out-fracture the turbinates, rather than resecting them. Still, pituitary resection was difficult through this long, narrow access using a headlight and naked eye (Figures 2 and 3).
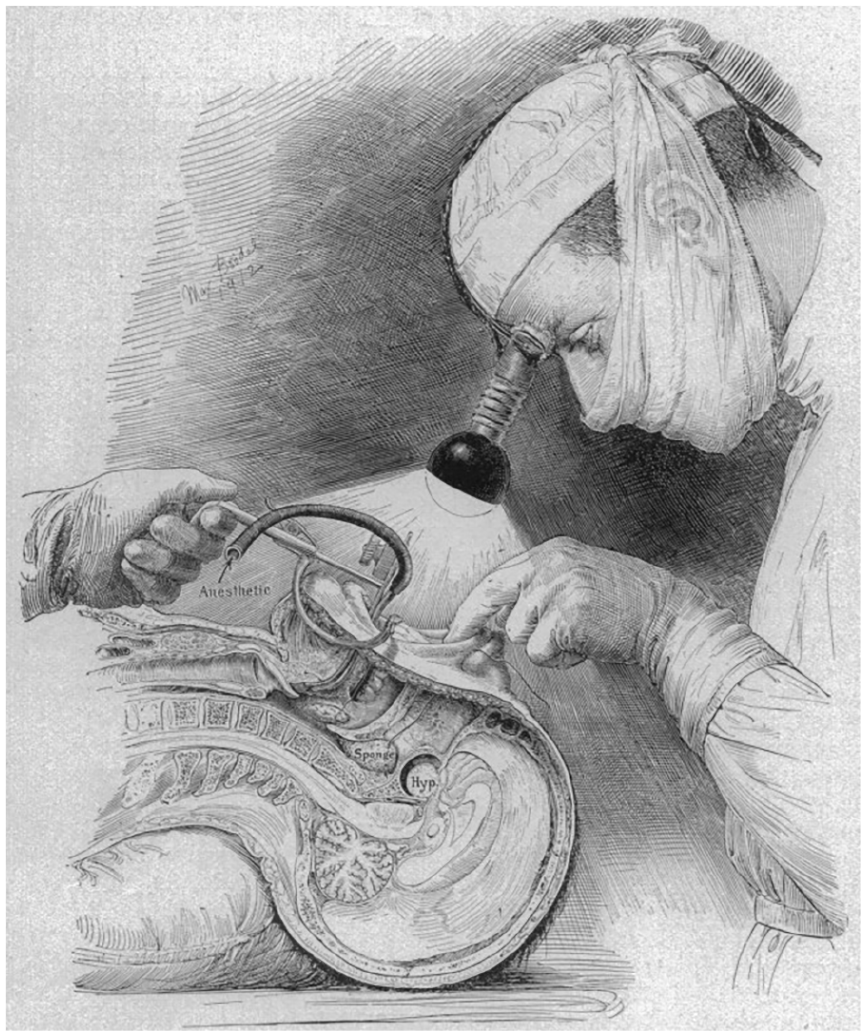
Drawing of Cushing using an electric headlight to illuminate the sublabial region (Cushing 8 ).
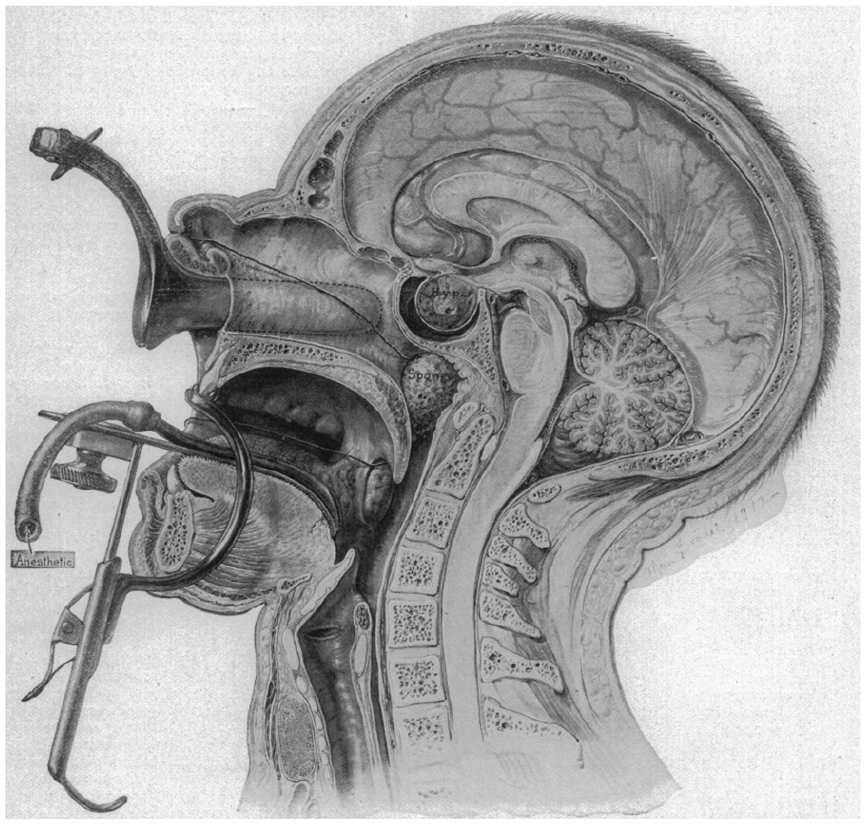
Drawing of the sublabial, transseptal, and transsphenoidal approach to the sella turcica—retractors in place. General anesthesia is delivered via a tube in the oral retractor (Cushing 8 ).
Cushing’s fastidious technique reduced operative mortality to 5.6% with 231 tumors operated between 1910 and 1925. By 1929, however, he had abandoned the transseptal transsphenoidal approach in favor of open intracranial resection which he felt decreased the risks of meningitis and allowed more complete tumor resection. His powerful sway in the American neurosurgical community relegated transsphenoidal surgery to obscurity for almost 50 years. 9
Over the ensuing decades, Norman Dott in Edinburgh and Gerard Guiot in Paris kept the transsphenoidal approach alive. Researchers gained a greater appreciation of pituitary anatomy and endocrinology. Pneumoencephalography improved diagnosis and antibiotics were developed to control infection. Finally, in 1967, Jules Hardy of Montreal incorporated the newly developed Zeiss OPMI-1 microscope into transsphenoidal surgery, making resection of pituitary microadenomas a reality.