
Abstract
Significance Statement
This case highlights the importance of considering laryngeal neurofibroma in the differential diagnosis of submucosal smooth laryngeal masses. It underscores the challenges of biopsy due to the tumor’s firm consistency and bleeding risk, emphasizing caution with preoperative sampling. Additionally, the nonspecific symptoms — dysphonia, odynophagia, and unintentional weight loss — may mimic malignancy, complicating diagnosis.
Case Report
A 75-year-old male presented with a 2 month history of sudden-onset dysphonia, which initially showed a slight improvement with antibiotic therapy prescribed by his primary care physician but subsequently worsened. He also reported left lateral cervical pain radiating to the ipsilateral ear and left-sided odynophagia. Additionally, he experienced an unintentional weight loss of 3 kg over 1 month. He denied any other complaints and had no history of alcohol or tobacco use.
Physical examination revealed a submucosal swelling of the left arytenoid with preserved bilateral vocal fold mobility. Magnetic resonance imaging (MRI) demonstrated a well-defined mass localized to the left arytenoid region, with no evidence of cervical lymphadenopathy. The lesion exhibited high signal intensity on T2-weighted images, iso-intensity on T1-weighted images, and mild contrast enhancement following gadolinium injection.
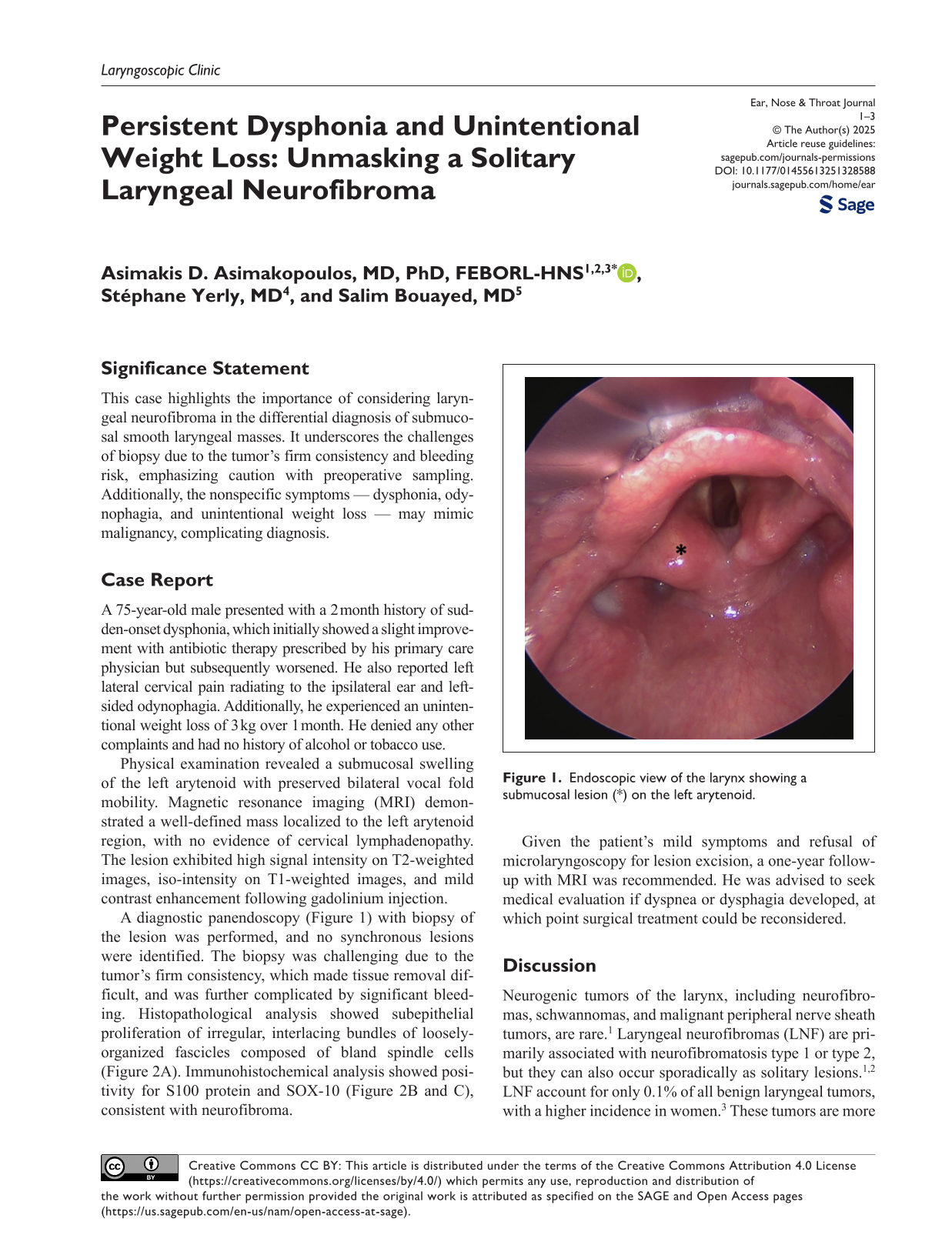
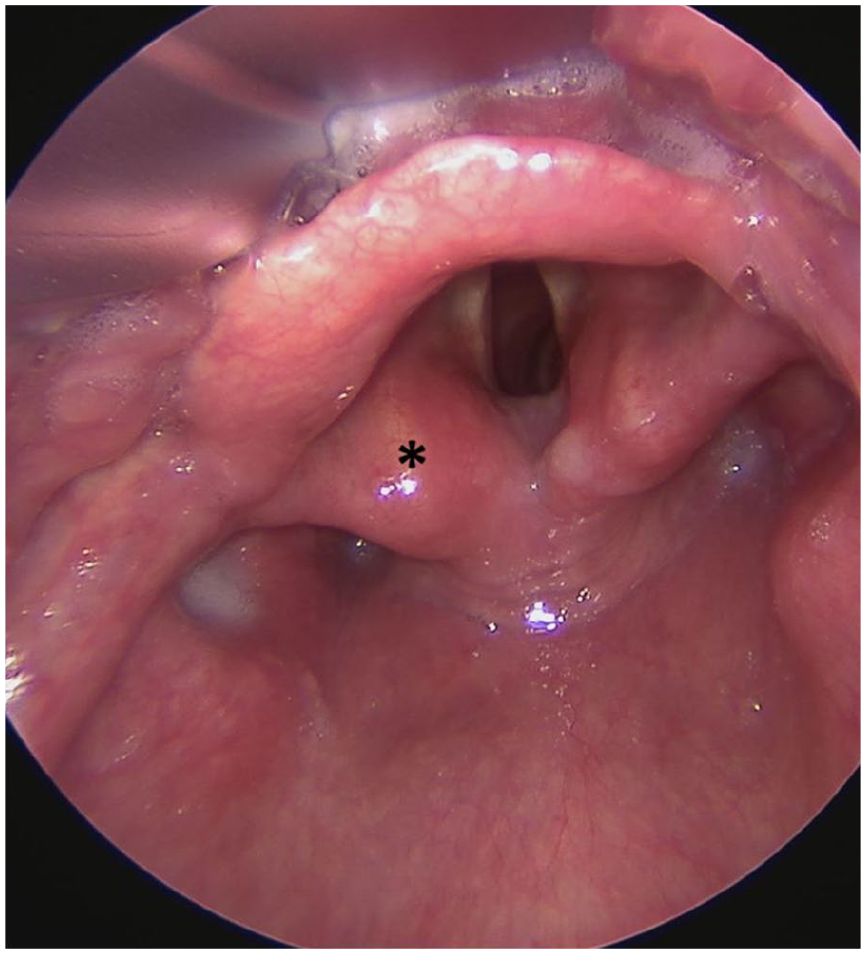
A diagnostic panendoscopy (Figure 1) with biopsy of the lesion was performed, and no synchronous lesions were identified. The biopsy was challenging due to the tumor’s firm consistency, which made tissue removal difficult, and was further complicated by significant bleeding. Histopathological analysis showed subepithelial proliferation of irregular, interlacing bundles of loosely-organized fascicles composed of bland spindle cells (Figure 2A). Immunohistochemical analysis showed positivity for S100 protein and SOX-10 (Figure 2B and C), consistent with neurofibroma.
Endoscopic view of the larynx showing a submucosal lesion (*) on the left arytenoid.
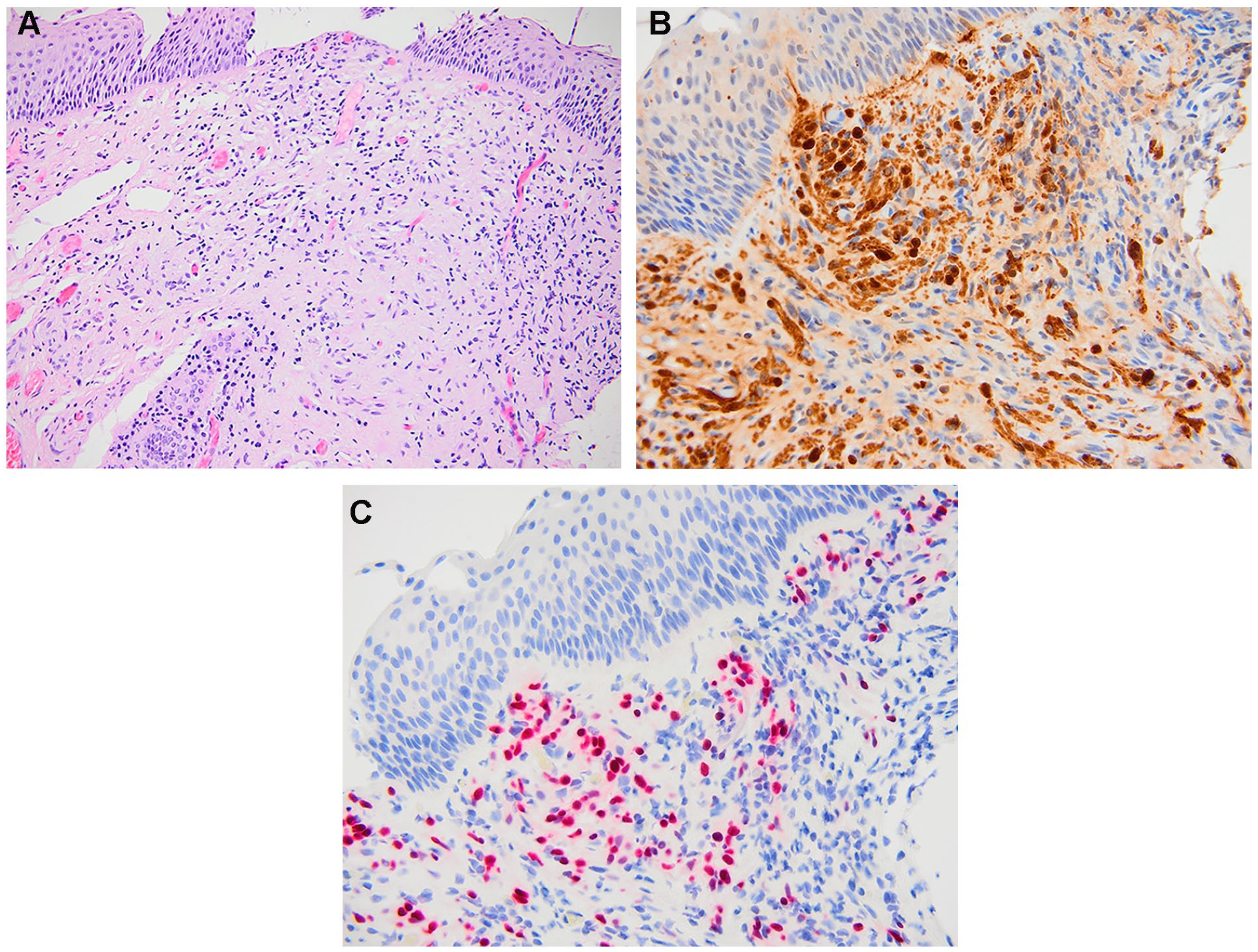
Histologic cross-sections. (A) Subepithelial proliferation of irregular, interlacing fascicles of bland spindle cells with wavy, dark nuclei and thin cellular processes (hematoxylin and eosin, ×200). (B, C) Immunohistochemical positivity for S100 protein (×400, B) and SOX-10 (×400, C).
Given the patient’s mild symptoms and refusal of microlaryngoscopy for lesion excision, a one-year follow-up with MRI was recommended. He was advised to seek medical evaluation if dyspnea or dysphagia developed, at which point surgical treatment could be reconsidered.
Discussion
Neurogenic tumors of the larynx, including neurofibromas, schwannomas, and malignant peripheral nerve sheath tumors, are rare. 1 Laryngeal neurofibromas (LNF) are primarily associated with neurofibromatosis type 1 or type 2, but they can also occur sporadically as solitary lesions.1,2 LNF account for only 0.1% of all benign laryngeal tumors, with a higher incidence in women. 3 These tumors are more common in younger patients, particularly in those with neurofibromatosis. 2
Neurofibromas can be classified as plexiform, diffuse, or both. 1 Plexiform variants, diagnostic of neurofibromatosis type 1, spread along nerve networks, grow slowly, and may remain asymptomatic. 1 The solitary cutaneous variant is most common in neurofibromatosis type 1, with plexiform tumors showing a “bag of worms” appearance.1,2 LNF are likely to cause airway obstruction and have an increase risk of malignant transformation, particularly in pediatric patients, who may present with low-grade fever.1,2,4
LNF most commonly affect the aryepiglottic folds and arytenoids, regions rich in terminal nerve plexuses, suggesting their origin from the superior laryngeal nerve or its anastomoses with the recurrent laryngeal nerve.1-4 Due to their slow growth and variability in size and location, LNF may remain asymptomatic for years or present with dysphagia, dysphonia, globus sensation, wheezing, stridor, or acute respiratory distress.1-4 Commonly-reported symptoms include coughing, choking, and unintentional weight loss. 2 Symptoms often persist for many months or years before diagnosis.1-4 Tumors located in the subglottis may originate from the superior laryngeal nerve, while those in the supraglottic region likely arise from the recurrent laryngeal nerve. 1
From a diagnostic perspective, flexible laryngoscopy typically reveals a highly-vascular, smooth submucosal mass, most often located in the supraglottic region. 4 Direct laryngoscopy, bronchoscopy, neck computed tomography (CT), MRI, and histopathological analysis are valuable diagnostic modalities. Due to the submucosal location, firm capsule, and high bleeding risk, preoperative biopsy is generally not recommended. 3 Holinger and Cohen reported significant bleeding following endoscopic biopsy in cases of LNF. 3 The definitive diagnosis relies on histopathological and immunohistochemical analysis, particularly positive S100 protein and S100 staining.1-4
Solitary LNF show variable signal intensity on T2-weighted images based on fibrous tissue content.1,3 Enhancement patterns on CT and MRI can be moderate and heterogeneous or homogeneous and intense.1,3 A study highlighted 4 MRI features—larger tumor size, peripheral enhancement, perilesional edema, and intratumoral cysts—that help differentiate malignant peripheral nerve sheath tumors from neurofibromas. 5 The presence of 2 or more of these features suggests malignancy, guiding the decision for biopsy or follow-up. 5
A minimally-invasive endoscopic approach aimed at preserving laryngeal function is recommended for localized lesions. Long-term follow-up is necessary due to the potential for recurrence over months to years and the risk of malignant degeneration, highlighting the importance of postoperative follow-up with endoscopic surveillance.1,3,4 Microsurgery and CO2 laser excision are effective in preventing recurrence. 3 For larger tumors, an external approach, such as lateral pharyngotomy, may be required.1,3,4 While CO2 laser techniques offer advantages of precision and reduced operative time, they may complicate tumor differentiation due to thermal tissue damage. 3 Tracheotomy may be necessary in cases of significant airway obstruction.1-3 A conservative approach is recommended when complete resection is not feasible, and the patient exhibits minimal symptoms. 1