
Abstract

Significance Statement
We present a patient with acute onset pulsatile bleeding from a right neck wound discovered to be a facial artery pseudoaneurysm with fistulisation to skin. Pseudoaneurysms of the head and neck are thought to be rare due to the small caliber of involved vessels. Consideration of vascular etiologies for head and neck masses is crucial for prompt diagnosis to minimize the risk of hemorrhage in the context of an evolving injury or hasty bedside intervention.
Introduction
A true aneurysm is characterized by a vascular dilation involving all 3 blood vessel wall layers: the intima, media, and adventitia. They are most frequently associated with atherosclerosis but can also be caused by trauma and infections. 1 In contrast, a false or pseudoaneurysm is formed by perivascular fibrous tissue. It typically arises following blunt trauma, which results in the partial disruption of the vessel wall and subsequent extravasation of blood into the surrounding tissues, followed by tamponade and clot formation. The interval between the initial injury and the clinical manifestation of a pseudoaneurysm can range from days to several years, often presenting as a pulsatile mass with an associated bruit. 2 Diagnosis is most commonly achieved via imaging modalities such as computed tomography, arteriography, and occasionally ultrasonography.3,4 Observation, anticoagulation, endovascular embolization, intralesional sclerotherapy, and operative management via surgical ligation with and without resection remain the cornerstone of management.4,5
We present the case of a ruptured pseudoaneurysm of the right facial artery in a previously-healthy 21-year-old woman without evidence of significant blunt trauma or operative history. To the authors’ knowledge, this represents the second case of facial artery pseudoaneurysm without traumatic origin, the sixth such case involving the proximal facial artery, and the first presenting with rupture and formation of a fistula to the skin.
Case Description
A 21-year-old female with no relevant past medical history presented to the emergency department of a community hospital with complaints of acute onset pulsatile bleeding from a wound in the right neck. The bleed was initially controlled with compression, and the patient required transfusion for stabilization prior to transfer to an academic center. The patient denied a history of trauma to the head and neck other than a small abrasion from her domestic cat, and physical exam revealed no stigmata of acute or resolved blunt or penetrative injury in the head and neck region.
A computed tomography angiography (CTA) of the neck revealed an 11 mm dilation of the right facial artery, with signs of rupture and bleeding into the ulcerated skin area (Figure 1).

(A) Demonstration of an 11 mm vascular dilatation (arrow) at the level of the proximal right facial artery with fistula formation to skin. (B) Computed tomography angiography, coronal view of the neck showing the right facial artery pseudoaneurysm (arrow). Skin and subcutaneous tissue defect overlying the pseudoaneurysm consist with an open wound (double arrow).
Of note, the patient presented with a normal white blood cell counts (8300/mL) and C-reactive protein levels (<0.20 mg/L). Bartonella serology was negative. Bacterial and fungal cultures of a swab of the wound were significant for Staphylococcus aureus and Peptosteptococcus anaerobius. The consideration of a mycotic aneurysm remained, albeit in the context of normal inflammatory and infectious markers.
Acute Intervention
The bleeding was initially managed with a compression dressing. Given the large right neck wound, the patient was referred to the interventional radiology team for acute intervention. The patient was admitted for fluoroscopic-guided angiography and endovascular coil embolization.
Right femoral access was obtained under ultrasound guidance and local anesthesia before the placement of a 5 Fr vascular sheath. The facial artery was selected with a 4 Fr Headhunter catheter (Cook Medical, Bloomington, IN, USA). A 2.4 Fr Progreat microcatheter (Terumo, Tokyo, Japan) was then advanced to the pseudoaneurysm feeding branch and selective coil embolization performed. Completion angiogram postembolization confirmed successful exclusion with no residual flow in the pseudoaneurysm (Figure 2). Following the procedure, the patient did not experience any further episodes of bleeding and was admitted for monitoring. Blood cultures were negative, and the bacterial culture of the skin lesion swab revealed the presence of S. aureus and P. anaerobius. Patient was discharged home with wound care, a 4 week course of amoxicillin clavulanate and doxycycline with delayed surgical intervention for wound management.
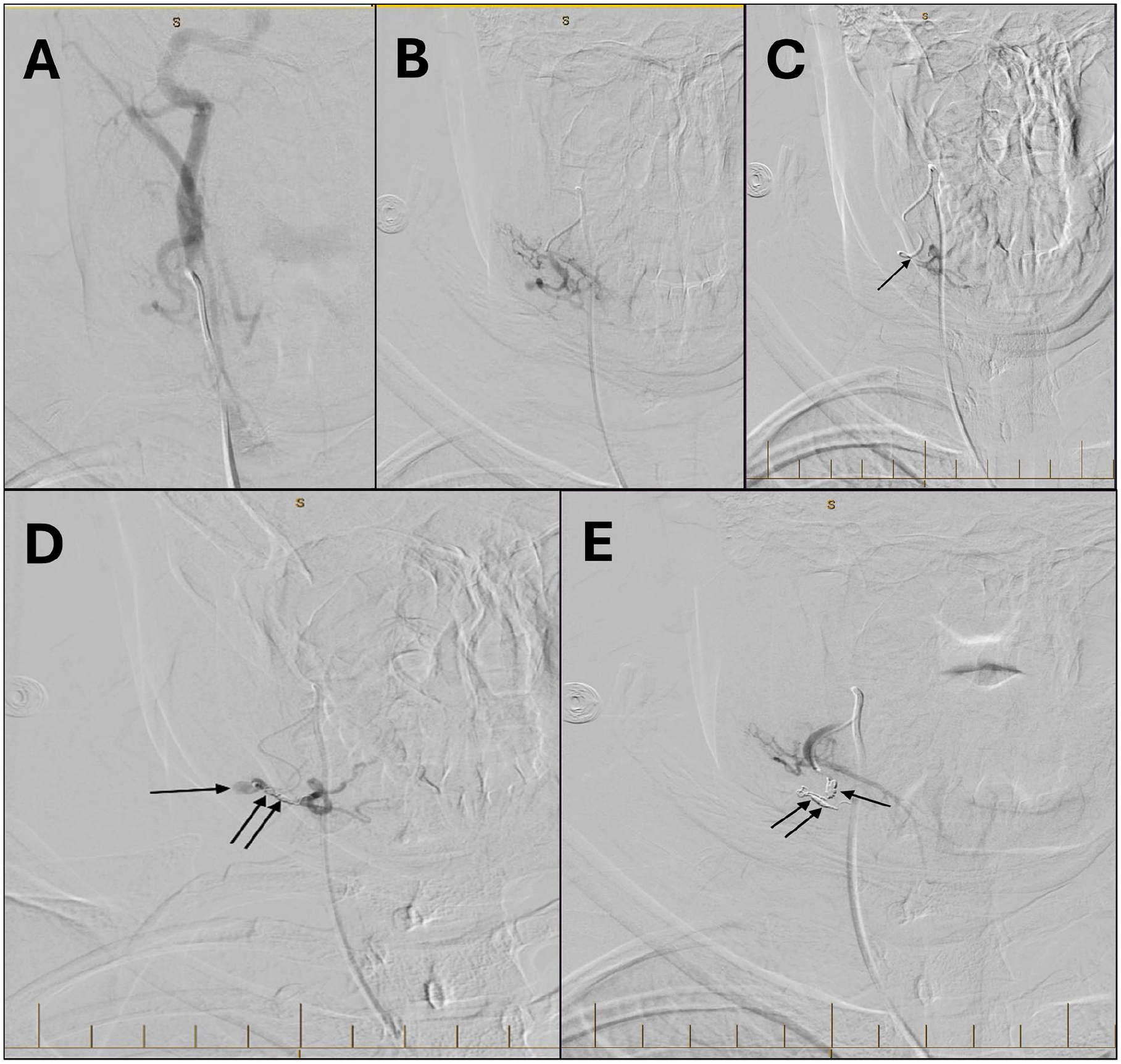
(A) X-ray angiography of right facial artery pseudoaneurysm before embolization. (B) X-ray angiography of right facial artery pseudoaneurysm before embolization demonstrates absent flow within the pseudoaneurysm. (C) A coronal view of digital subtraction angiography showing the catheter tip (arrow) advanced distally beyond the pseudoaneurysm (not visualized) to assess additional vascular anomalies, none of which were observed. (D) A coronal view of digital subtraction angiography showing the right facial artery pseudoaneurysm (arrow). Coils (double arrow) were inserted distal to the pseudoaneurysm as the first part of the sandwich technique. (E) A coronal view of digital subtraction angiography showing proximal (single arrow) and distal (double arrows) coils. The angiographic image demonstrates the resolution of the previously-observed right facial artery pseudoaneurysm.
Surgical Intervention
Approximately 6 weeks following the embolization, a right neck exploration with facial artery ligation, resection, and local flap reconstruction was performed. The facial artery was isolated and ligated proximally, and the pseudoaneurysmal sac resected along with the surrounding scar and coiled feeding vessel (Figure 3). The patient recovered well with no complications, specifically no marginal mandibular nerve weakness.

Aneurysmal sac seen with visible endoluminal coiling material within the feeding vessel.
Discussion
Facial artery pseudoaneurysms are rare, especially in the absence of a clear trauma history. The branches most frequently involved include the superficial temporal artery, internal maxillary artery, and distal facial artery, particularly at locations where they traverse bony structures such as the zygoma or mandible. 2 In rare cases, factors such as infection, atherosclerosis, cystic medial necrosis, and fibromuscular dysplasia can lead to pseudoaneurysms of the external carotid artery itself. However, it remains unclear whether these conditions can also give rise to pseudoaneurysms of smaller branches. 2
Clinical signs such as bruit and pulsatile masses suggest a vascular origin for the lesion, potentially indicating a true or false aneurysm or an arteriovenous fistula. Color Doppler ultrasonography is commonly used as a screening tool, while CTA confirms the diagnosis. Treatment is generally considered necessary due to the instability of the pseudoaneurysm wall, which carries the risk of expansion and rupture. Treatment options include observation in select cases, anticoagulation, ligation, surgical removal, or endovascular interventions such as embolization or stenting. 2
Traditionally, pseudoaneurysms have been treated surgically by ligating the affected vessel and excising the lesion, especially when it is superficial and accessible, with minimal impact on tissue perfusion. However, surgery carries risks such as external scarring, anesthesia-related risks, bleeding, wound infection, lymphocele formation, radiculopathy, prolonged recovery time, perioperative myocardial infarction, and death. 6 Pseudoaneurysms at the level of the head and neck are thought to be rare due to the small caliber of involved vessels, as well as their deep position under overlying fat and subcutaneous tissue. This makes injury of these vessels relatively uncommon, and complete transection is more likely than partial injury of the vessel wall when sufficient penetrating trauma does occur. Blunt trauma is thought to cause pseudoaneurysms through arterial wall contusion and subsequent breakdown, leading to blood extravasation into surrounding tissues 7 . Endovascular embolization is a less invasive alternative, particularly effective for pseudoaneurysms that are difficult to access surgically. It reduces risks like delayed bleeding and revascularization through collateral circulation. However, complications such as neurological injury or soft tissue necrosis can occur due to the reflux of embolization material or damage to adjacent structures. This technique also requires specialized equipment and a skilled interventional radiologist. 6
Dediol et al. presented, to our knowledge, the first and only case of facial artery pseudoaneurysm without a history of trauma or connective tissue disease. 2 Proximal facial artery involvement—defined as the region between the external carotid and the lower border of the mandible—is also exceedingly rare, with all other associated case reports involving significant trauma or surgical intervention to the neck prior to presentation. 4
Besides traumatic causes of pseudoaneurysm formation in the proximal facial artery, we suggest that infectious causes might represent a rare inciting event. The possible introduction of infection through a superficial skin wound to a superficial facial artery remains a possible cause of mycotic pseudoaneurysm formation. 8
We do, however, suggest that vascular lesions remain an important consideration when presented with soft tissue lesions, given the elevated risk of hemorrhage in the context of accidental injury or rupture, which can be precipitated by hasty bedside intervention. This further highlights the crucial nature of point-of-care ultrasound with Doppler analysis in the investigation of all soft tissue lesions of the head and neck prior to intervention.
Footnotes
Data Availability Statement
Statements regarding data availability to not apply given the nature of the case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent for Publication
The patient provided written informed consent to publication of their case. All identifying data from the individual have been omitted in the interest of patient confidentiality.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Not applicable due to the current case report in the context of its nature.
Consent to Participate
Not applicable to the current case report in the context of its nature.