
Abstract
A 66-year-old female patient presented with a pulsating right-sided neck mass which had been present for several years, but then greatly expanded in size with coughing episodes secondary to COVID-19 infection. A chest computed tomography (CT) scan ultimately revealed the cause to be apical lung herniation. This case is unique as the herniation may have been present for years, but treatment was not sought until its size increased with the patient’s chronic coughing.
Introduction
Apical lung herniation is a rare form of lung herniation, as most lung hernias are thoracic or diaphragmatic. 1 In previously reported cases, apical herniations are often associated with elevated intrathoracic pressure, which can occur with coughing paroxysms, the Valsalva maneuver, or continuous positive airway pressure devices. Additionally, there is an association with weakening of Sibson’s fascia, an extension of the endothoracic fascia that covers the apex of the lung medial to the first rib. 4 Causes of such weakening can include neck trauma or congenital connective tissue disorders.2,3 Apical lung herniation stands out among the differential diagnoses for neck swelling due to its ability to fluctuate with changing pressure inside the lungs. Because of this unique characteristic, dynamic CT scan before and after a Valsalva maneuver is the definitive diagnostic test for apical lung herniation.
Case History
We present the case of a 66-year-old woman who presented to the emergency department with the chief complaint of an anterior neck mass. The patient had a history significant for hypertension and type II diabetes. The patient also had a history of neck trauma due to a whiplash injury sustained during a fall several years ago. At the time the patient was seen in the hospital, her neck mass had already been present for years, although at a much smaller size. The patient did not seek any treatment until coughing paroxysms associated with a recent COVID-19 infection exacerbated the swelling and caused it to greatly increase in size. The swelling expanded sharply during coughing episodes and was also observed to have a pulsating nature. The patient also noticed that her neck swelling increased in size with increased salt intake.
The neck swelling, although present bilaterally, was noted to be more prominent on the right. This is in accordance with prior literature which has observed apical lung herniations to be more common on the right and more prominent on the right when occurring bilaterally. 4 The pulsatile nature of the neck mass led to the initial consideration of jugular vein distention as a possible diagnosis. A CT angiogram was done to rule out jugular vein distention or aneurysm, which showed an incidental finding of left vertebral artery occlusion.
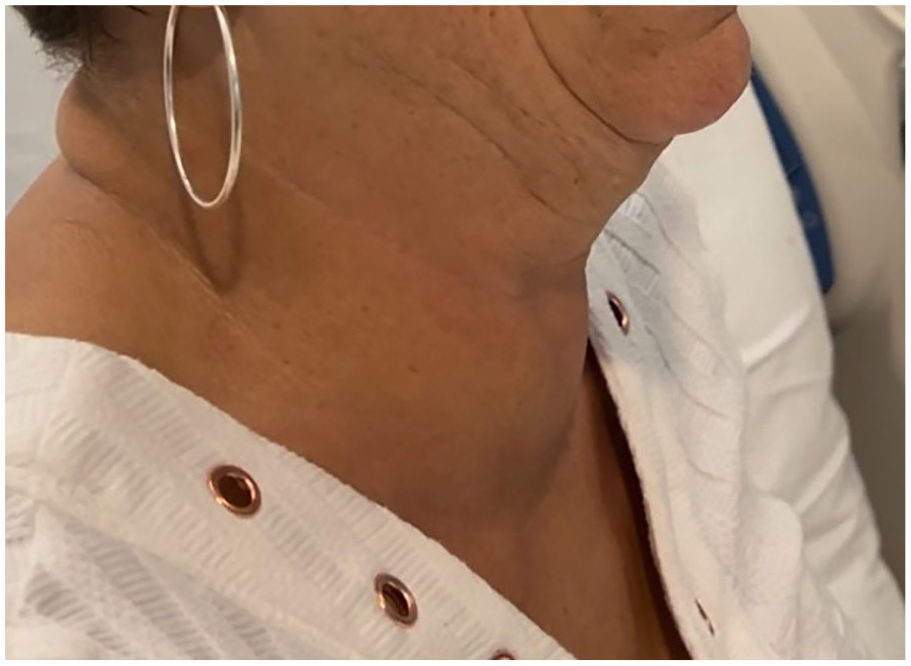
Physical examination of the neck revealed that the swelling expanded when the patient coughed or performed the Valsalva maneuver. The images in Figures 1 and 2 show the patient’s neck at rest, and after a cough, respectively. The presence of a right-sided apical lung hernia was ultimately confirmed by a chest CT performed during a Valsalva maneuver (Figure 3), which is often used to diagnose apical lung herniation.4,5 After the diagnosis was made, no further treatment of the hernia was performed. Surgical treatment, while a possibility, is seldom needed for cases of apical lung herniation.
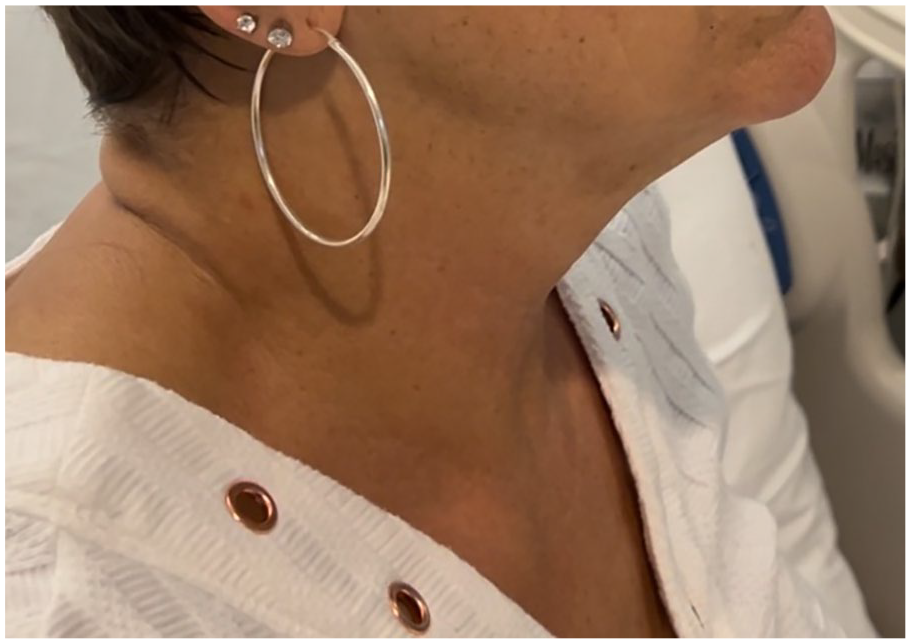
Picture of the patient at rest, with no neck mass visible.
Picture of the patient after a cough, with neck swelling visible anterolaterally.
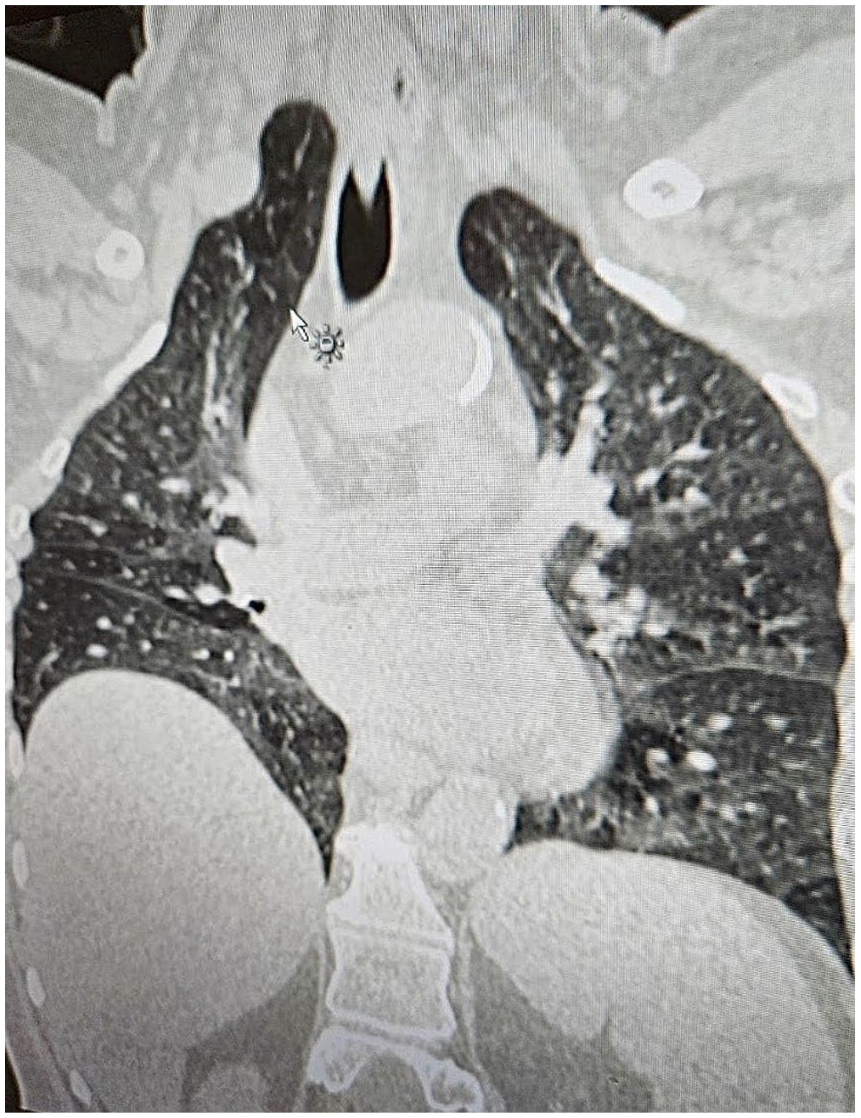
CT chest showing apical lung herniation into right neck with Valsalva.
Discussion
A factor which distinguishes this case from others is that the lung herniation was likely present and stable for years before treatment was sought. The swelling was noted to increase dramatically in size with coughing episodes, which served as a critical diagnostic clue in this instance. The patient also observed that her neck swelling expanded after periods of high sodium intake, an observation which has not been previously reported with apical lung herniations. Also unique to this case was the pulsatile nature of the swelling, which initially led vascular etiology to be considered as a diagnosis.
This case highlights the importance of recognizing the potential for multiple contributing factors in cases of lung herniation. In this case, both a distant history of neck trauma and elevated intrathoracic pressure due to coughing episodes were present. There is also the possibility of an underlying congenital defect of the Sibson’s fascia, which is often seen in cases of apical herniation. 5
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.