
Abstract

Significance Statement
Nasopharyngeal necrosis is a rare but life-threatening complication and should be cautioned in such adenoid cystic carcinoma case with surgery and postoperative radiotherapy. Early endoscopic surgical debridement with the combination of nasal irrigation and hyperbaric oxygen therapy are crucial to improve outcomes for patients suffering from this debilitating condition.
Head and Neck Clinic
A 69-year-old female patient presents with vertigo for months and accidently found with nasopharyngeal lesion by brain computed tomography (CT). Nasopharyngoscopy revealed an exophytic mass arising from posterior nasal septum to left nasopharyngeal wall (Figure 1A). The biopsy was proved as adenoid cystic carcinoma. MRI and positron emission tomography (PET)/CT showed a 2.7 cm mass on the nasopharynx (Figure 1C-E). The patient received endoscopic transnasal resection of the lesion totally (Figure 1B and video) and postoperative radiotherapy (RT) 1 week later after the surgery. The dose of RT was delivered 70 Gy in 35 fractions to previous tumor site, and 60/50 Gy to the nodal region by 20 times within 2 months (Figure 2A). However, severe dysphagia, odynophagia, and dysphonia were presented after 4-month post definitive RT. Flexible laryngoscopy showed diffuse debris and necrotic tissue with odorous smell over nasopharynx (Figure 2B) and right-sided vocal palsy. On physical examination, her tongue movement was limited. CT of the nasopharynx showed the findings of osteoradionecrosis (ORN) (Figure 2C and D). The patient underwent endoscopic sequestrectomy, sphenoidotomy, and debridement of ORN (Figure 3A and video). The patient was also given with hyperbaric oxygen therapy (HBOT) and nasal irrigation with hydrogen peroxide (H2O2) for 3 months (Figure 3B). The wound got healed and no recurrence of cancer during a 2-year follow-up (Figure 3C-F).
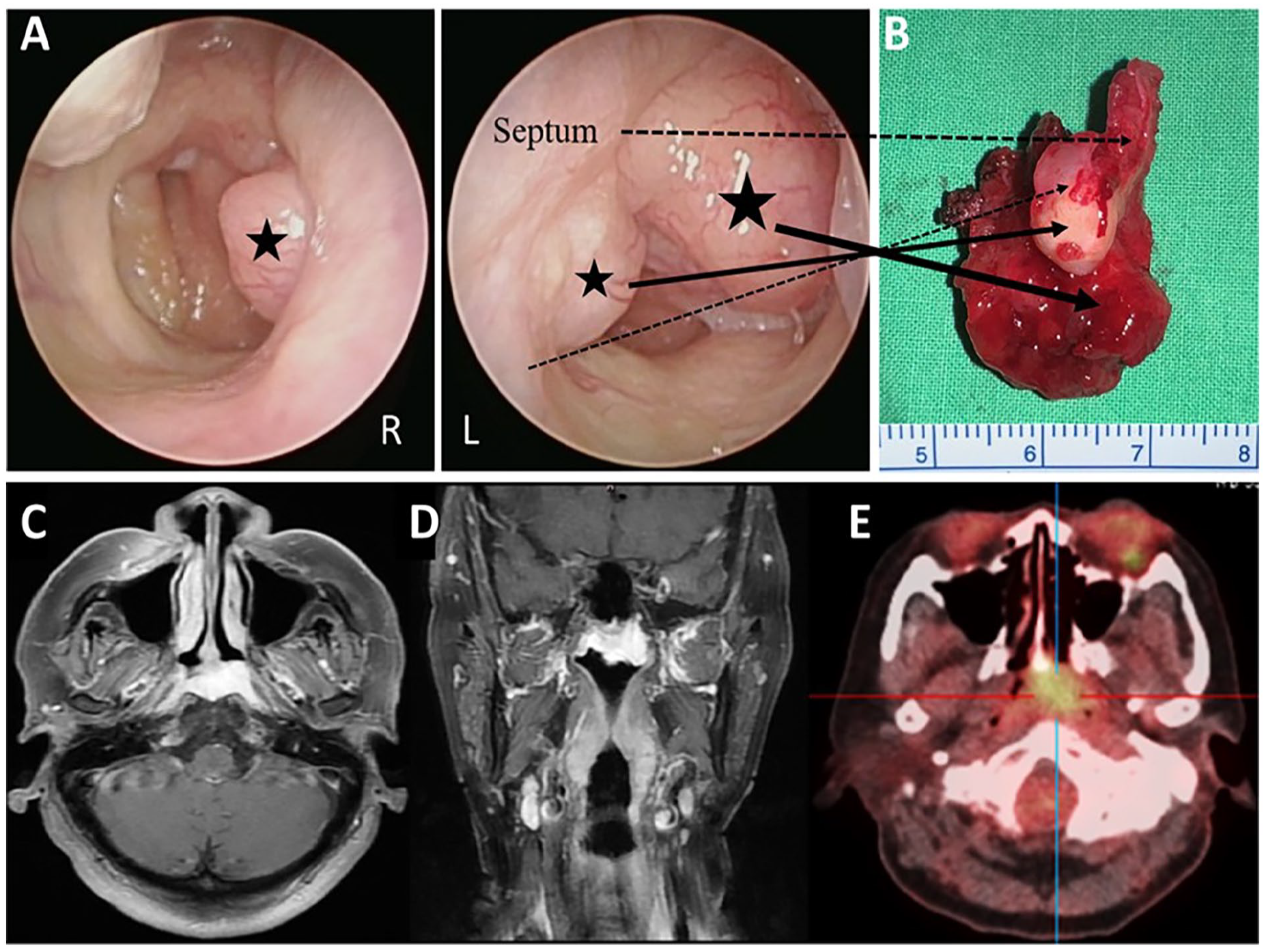
(A) Nasopharyngoscopy from the left side revealed an exophytic mass arising from posterior nasal septum (small star) to left nasopharyngeal wall (large star) and the lesion (small star) was visible from the right side. (B) Surgical specimen related to the corresponding anatomy. (C) Axial and (D) coronal view of MRI of the head and neck showed a 2.7 cm in size lesion on the left nasopharynx. (E) The PET-CT scan of the whole body showed intense metabolism over the nasopharynx without local nodal or distal metastasis.
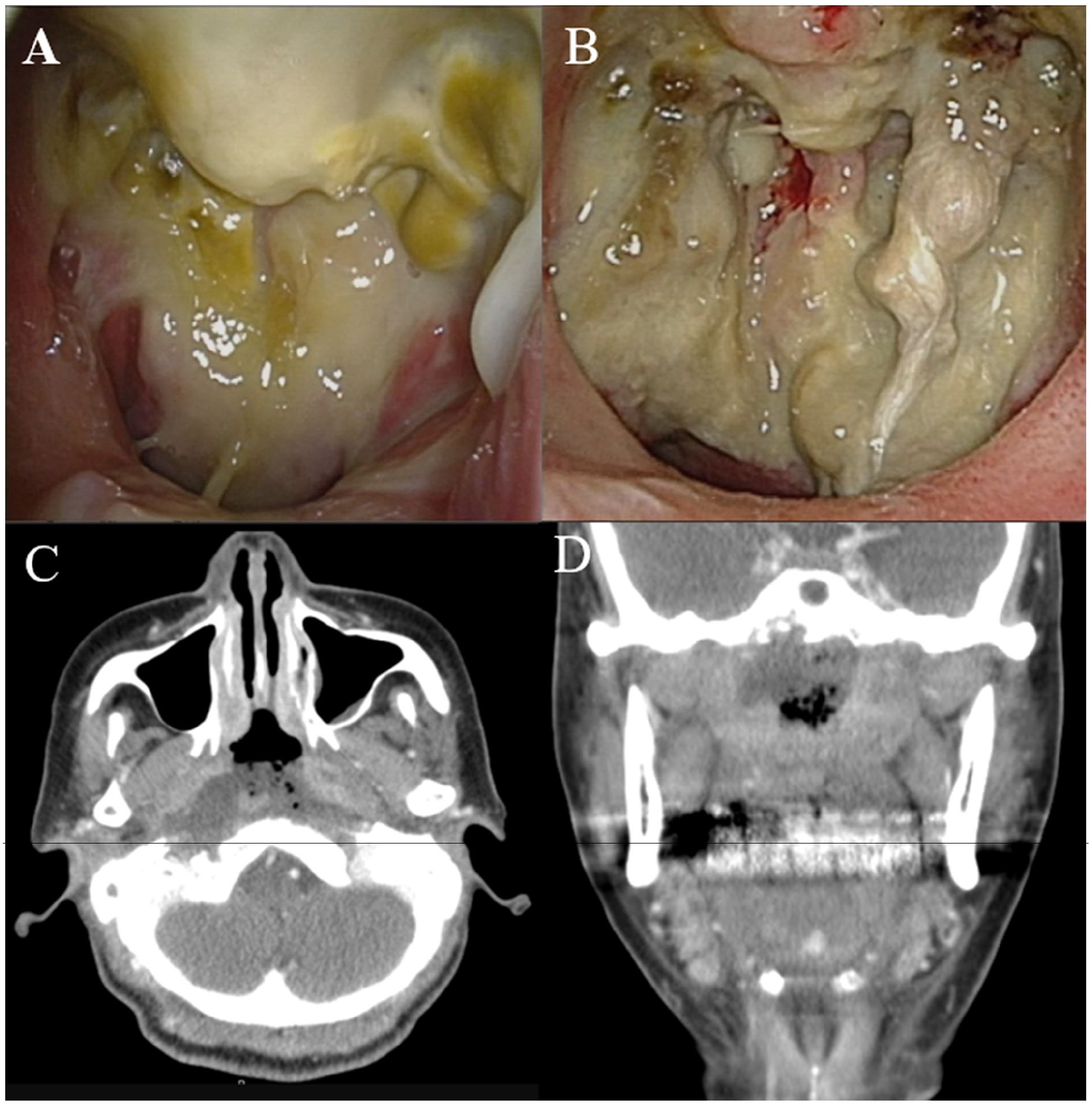
(A) The endoscopic view of the nasopharynx showed the condition after completion RT. (B) The endoscopic view of the nasopharynx showed the condition after 4-month postoperative RT. The axial view (C) and coronal view (D) of CT of the nasopharynx showed the imaging corresponding to the real view in (B). RT, radiotherapy.
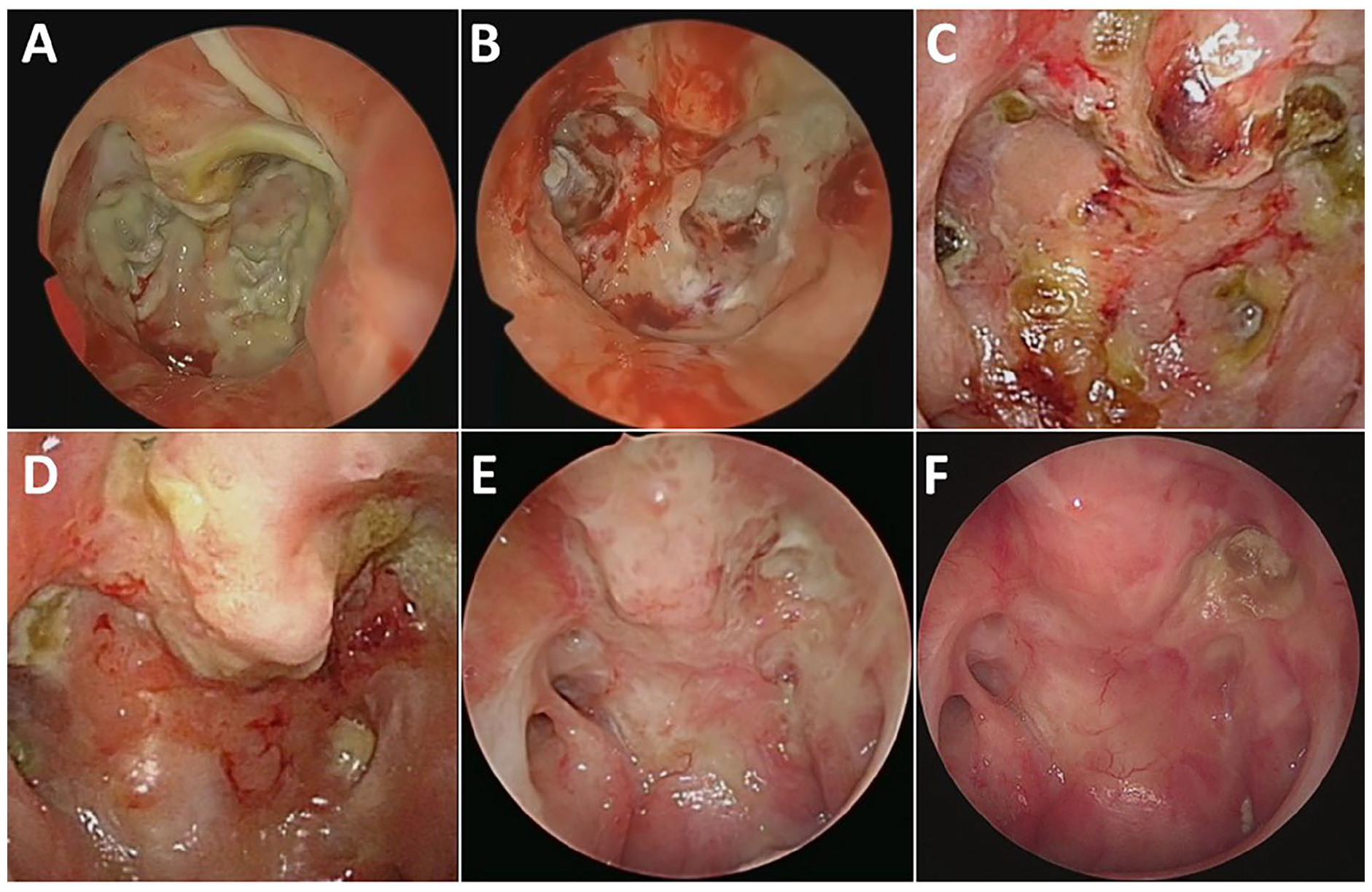
(A) The endoscopic view of the nasopharynx was shown after the surgical debridement. (B) 1-month, (C) 3-month, (D) 6-month, (E) 12-month, (F) 16-month view post (A).
Adenoid cystic carcinoma (ACC) is commonly found in salivary gland but is rarely reported in nasopharynx, which accounts for only 0.13% to 4% of all nasopharyngeal carcinoma (NPC). Nasopharyngeal adenoid cystic carcinoma (NPACC) are common with clinical symptom of epistaxis, facial swelling, headache, tinnitus, and hearing loss. 1 NPACC is more recognized with advanced locally invasion and perineural spread. They usually extend along the cranial nerve canal, toward the orbital cavity and skull base, making all surgical approaches hard and delicate. 2
NPACC is a slow growing tumor with a long natural history, which is responsible for the delay in diagnosis and management. 3 Early diagnosis is challenging due to nonspecific symptoms, leading to treatment delays. The nasal endoscopic examination frequently shows a mass lesion in the nasopharynx. The diagnosis primarily relies on MRI and CT imaging to assess tumor extent and invasion, with endoscopic-guided biopsy providing histopathological confirmation. Histologically, ACC exhibits cribriform, tubular, and solid growth patterns. 3 The solid pattern has the worst prognosis and is also associated with the highest incidence of distant metastasis and perineural invasion. 3
Surgical resection is the mainstay but is challenging to get negative margin due to the complex anatomy of the nasopharynx. The endoscopic endonasal approach is safe and effective for selected NPACC cases, with better prognosis and lower morbidity than with the external approaches. 1 Postoperative RT, particularly intensity-modulated radiotherapy improves local control rates and overall survival. Chemotherapy has limited efficacy and is typically reserved for metastatic or recurrent cases. 3
Radiation‑related nasopharyngeal necrosis (RRNN) is a severe and often fatal complication in patients treated for NPC. The incidence of RRNN is relatively low in primary NPC patients (1%-2%) but significantly higher (30%-40%) in those undergoing reirradiation. 4 The risk factors include tumor stage, nutritional status during radiotherapy, and anemia. 5 This condition drastically impacts patient quality of life and is associated with symptoms such as foul nasal odor, persistent headaches, and recurrent epistaxis. In severe cases, RRNN can lead to cranial neuropathies and life-threatening complications such as massive nasopharyngeal bleeding due to internal carotid artery rupture. 1 The reported 2‑year overall survival in patients with RRNN is 51.6%. 4
Diagnosis of RRNN relies on clinical evaluation, nasopharyngoscopy, and MRI. The gold standard is pathological biopsy, although it is often challenging to obtain due to the risk of hemorrhage and the necrotic nature of the tissue. The management of RRNN can been treated conservative including nasal irrigation with 2% H2O2, systemic or topical antibiotics, intravenous nutritional support, and HBOT.4,5 However, the outcomes of these treatments are generally suboptimal. 4 HBOT plays a role on stimulating angiogenesis and increasing neovascularization, cellular levels of oxygen, fibroblast and osteoblast proliferation, and collagen formation in irradiated tissues; however, the true efficacy and evidence of HBOT was vague.5-7 The frequency and duration of irrigation regiment may be modified according to the actual condition.4,5 Surgical intervention, such as endoscopic or open surgery to remove necrotic tissue or complete resect the tissue followed by flap reconstruction, can be effective but is associated with high costs and requires significant surgical expertise. 5
The management of this case was conducted with extreme caution due to the high risk of internal carotid artery rupture. Subsequently, the patient underwent 3 additional debridement for nasopharyngeal osteoradionecrosis. The patient also received nasal irrigation with H2O2 diluent once a week for 3 months and 20 sessions of HBOT. Fortunately, the tongue movement and vocal function were recovered. We proposed the factors of anemia, early postoperative RT within 1 week and old age with poor nutrition contributed the RRNN in our presented case.
Footnotes
Author Contributions
The specific role and contribution of each author is as following: K.-Y.C.: first author and preparation of draft. H.-C.C.: corresponding author and editing of manuscript.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-A-114002 to Hsin-Chien Chen).
Ethical Statement
A written informed consent was obtained from the patient and was approved by Tri-Service General Hospital Institutional Review Board.
Patient’s Consent
The patient consent statement was informed and approved by Tri-Service General Hospital Institutional Review Board.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.