
Abstract
Hemangiomas are benign tumors of the blood vessels. Although most commonly associated with the skin, it can also occasionally be found in mucous membranes, the brain, and the viscera. The tonsillar localization is uncommon and rarely reported in the literature. The risk of bleeding complications and its impact on the upper airway can make the management of these tumors more complicated. We report the case of a 28-year-old patient, with no pathological history, who was referred to us to manage a formation in the left tonsillar region. The patient was completely asymptomatic. Physical examination showed a tumor originating from the upper pole of the left tonsil. The cervical computed tomography scan showed an iso-dense tissue formation at the expense of the left tonsillar region. The patient was operated on under general anesthesia and a resection of the tumor mass was performed without a hemorrhagic incident. The histopathological examination confirmed the diagnosis of mixed capillary and venous hemangioma and the resection was complete. The outcome was favorable after a 12-month follow-up. Tonsilla hemangiomas are a rare clinical entity that all ENT surgeons should be familiar with to better choose the treatment course to avoid bleeding complications and recurrences.
Introduction
Hemangioma, a benign tumor of the blood vessels, 1 is the most common tumor found in infants. 2 It occurs in 60% of cases in the head and neck regions. 3 The most common sites of hemangiomas in the oral cavity are the lips, tongue, buccal mucosa, and palate, 4 although tonsillar involvement is rarely reported in the literature. An imaging plan is essential to assess the lesion, surrounding tissues, and potential complications. Vascular lesions are challenging to operate on due to difficulties in controlling bleeding. Although it is asymptomatic, its location and size may require timely and careful management. The aim of our work, by reporting a rare case of a mixed (capillary and venous) hemangioma of the palatine tonsil, is to describe its epidemiological features, diagnostic elements, as well as the therapeutic approaches and evolution of these tumors.
Case Report
We report a case of a 28-year-old patient with no significant medical history, referred by a general practitioner after the incidental discovery of a mass in the left tonsillar region. The patient was otherwise completely asymptomatic. Examination revealed a pedunculated mass, 2 cm in diameter, pink in color, and non-bleeding on contact, originating from the superior pole of the left palatine tonsil. The contralateral tonsillar region was normal, and there were no palpable cervical lymph nodes. The rest of the ENT examination was unremarkable. A computed tomography (CT) scan of the facial region (with and without contrast) revealed a tissue mass within the left tonsillar region, isodense, and narrowing of the oropharyngeal lumen while preserving the parapharyngeal fat spaces and showing no cervical lymphadenopathy (Figure 1).
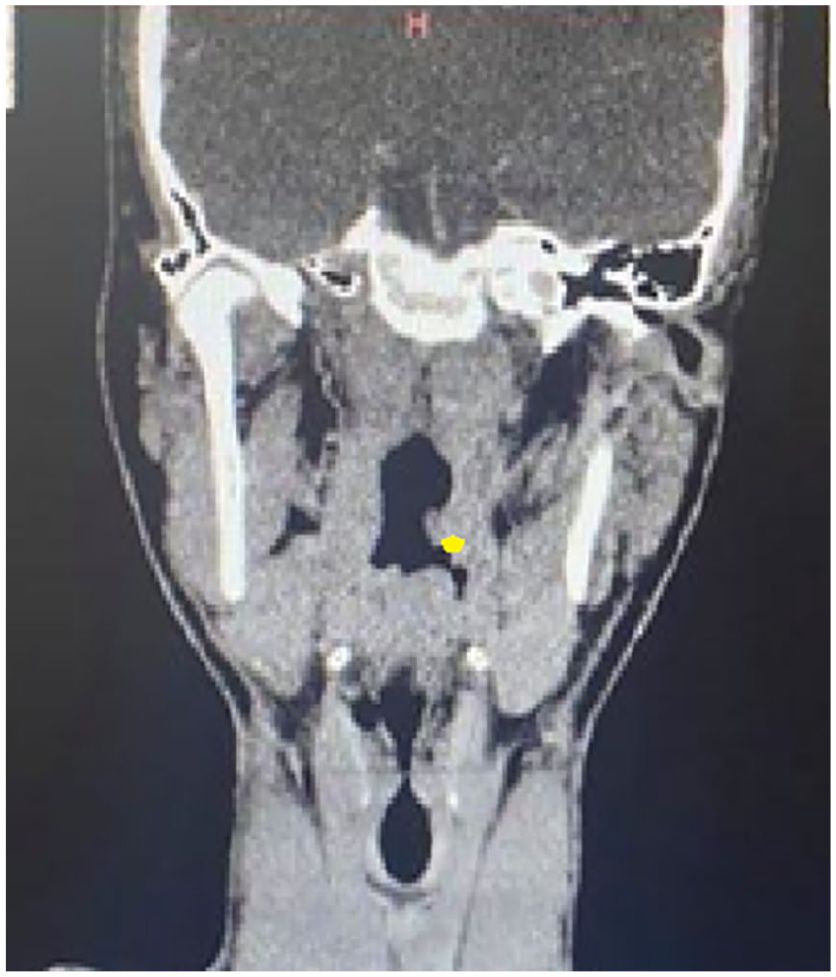
Coronal CT-SCAN showing the tumor in the left palatin tonsilla.
The patient underwent surgery under general anesthesia. Intraoperative exploration revealed a firm, non-pulsatile tissue mass, suspended by a pedicle from the superior pole of the left tonsillar region (Figure 2). We performed a complete excision of the tumor mass after double ligation and sectioning of its pedicle without any complications, particularly hemorrhagic (Figure 3). The patient was discharged home in good condition following the surgery. The histopathological report showed benign squamous mucosa with a vascular proliferation composed of thin-walled capillaries and thick-walled vessels with variable dilation (Figure 4). The diagnosis of a mixed capillary and venous hemangioma of the left tonsil was confirmed. The resection was complete.
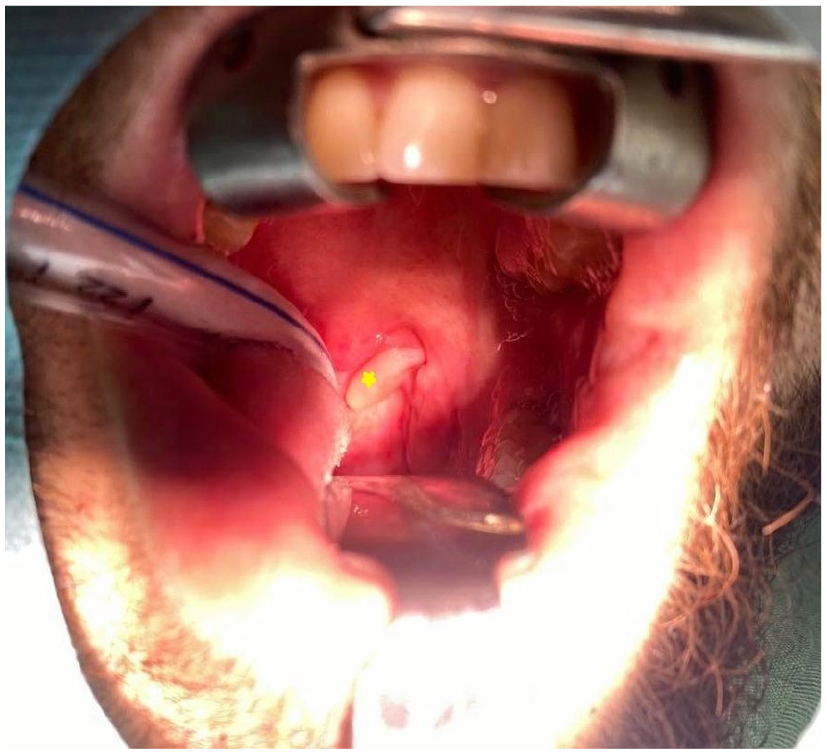
Intraoperative VUE: a firm, non-pulsatile tissue mass, suspended by a pedicle from the superior pole of the left tonsillar region.

The tumor mass after excision.
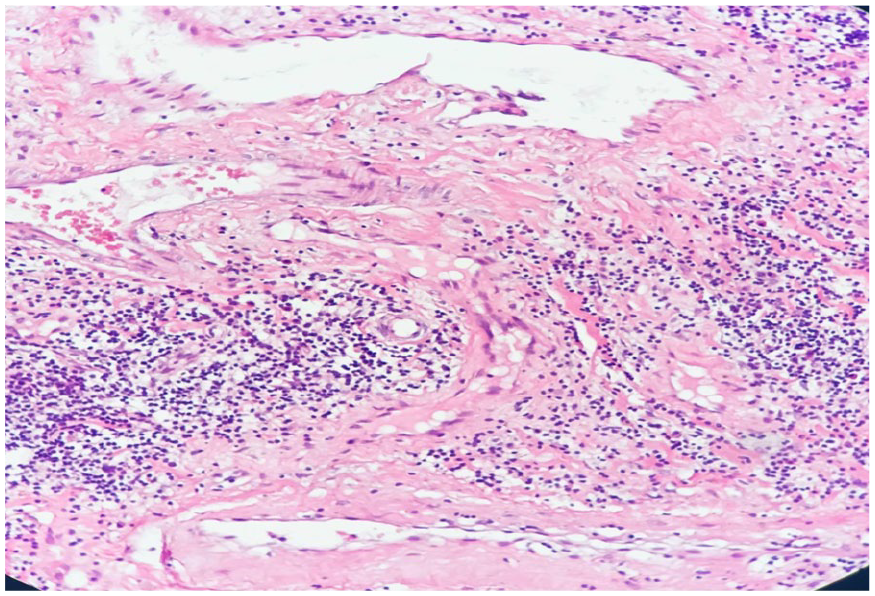
Histopathological VUE: benign squamous mucosa with a vascular proliferation composed of thin-walled capillaries and thick-walled vessels with variable dilation.
The postoperative course was uncomplicated, and the outcome was favorable after 12 months of follow-up. There were no clinical or radiographic indications of recurrence.
Discussion
The peculiarity of our case lies in the exceptional occurrence of this type of hemangioma in the tonsil. Hemangiomas are benign lesions characterized by the proliferation of blood vessels, and they do not progress into a malignant form. 5 They are classified into 5 types: capillary, cavernous, mixed capillary and cavernous, arterial, mixed arterial and venous. 6 In the literature, only 3 cases of cavernous tonsillar hemangiomas have been reported.7,8 The mixed capillary and cavernous tonsillar forms have never been reported. Some authors named this entity “pyogenic granuloma,” but we preferred not to use the term “pyogenic granuloma” and we opted for “ mixed hemangioma,” because the etiopathogenesis of these tumors is not yet clarified and as it was cited in the literature: The word pyogenic granuloma is a misterm since the situation is not related with pus and histologically does not exemplify a granuloma.9,10 Hemangiomas are more frequent in infants and children (10%-12%). However, their occurrence in middle-aged adults has been described, as a predilection for the extremities. Classically, hemangiomas have a ubiquitous distribution. They are frequently located in the skin. Oral hemangiomas typically appear on the gingiva and are less commonly found at other locations. They usually present as either the capillary or cavernous type, with the capillary type being more common. 4 Eighty percent of cases may be isolated, or less commonly, disseminated (multiple hemangiomas).2,4 Most recent studies have shown that cavernous hemangiomas are genetically determined and transmitted in an autosomal dominant manner. Genetic testing was not performed in our case since it involved an isolated tonsillar location without associated cutaneous vascular lesions. The causes of mixed hemangioma are unclear, some factors like: female sex hormones, chronic irritation, and trauma may pose a risk to its development. 11
The symptoms of tonsillar hemangiomas are varied and depend on the size of the tumor. Symptoms may range from mild pharyngeal discomfort, a sensation of a foreign body, or a tingling sensation in the tonsil, 8 to being completely asymptomatic. Our patient had no symptoms, and the lesion was incidentally discovered during a routine examination by a general practitioner. On physical examination, a tonsillar hemangioma appears as a firm, light pink mass, non-pulsatile, non-indurated, and non-bleeding on contact, which may be sessile or pedunculated.7,8 It can vary in size, ranging from just a few millimeters to several centimeters. These clinical features pose a differential diagnostic challenge with other benign tonsillar tumors (papilloma, benign tumors of the accessory salivary glands, lymphangioma, lipoma, fibroma, and neuroma). A hemorrhage can occur either spontaneously or following minor trauma. 5
Imaging studies can be essential for confirming the diagnosis and assessing the extent of the lesions, allowing evaluation of both the non-visible components and the involvement of surrounding structures. Angiographic studies are not strictly necessary for diagnosis and are primarily used to determine the lesion’s size and extent. 12 These procedures are more complex than histopathological evaluations, come with higher morbidity, and can lead to unwanted side effects. For these reasons, angiography was not considered in this case. Recently, CT and magnetic resonance imaging (MRI) have been successfully used for diagnosing hemangiomas, similar to other soft tissue lesions. On CT scans, they may appear slightly hypodense without contrast but can also be isodense, making them sometimes difficult to detect. On MRI, these lesions typically show a strong and homogeneous T2 hyperintensity and a contrast pattern similar to that seen on CT, with uniform and rapid contrast enhancement. In the 3 reported cases of tonsillar hemangiomas in the literature, no preoperative imaging was requested. For our patient, we performed a CT scan of the facial region with and without contrast injection to better characterize the tumor preoperatively. The definitive diagnosis of tonsillar hemangiomas is histopathological, and their histological appearance varies depending on the different phases of their evolution.
The treatment of hemangiomas is not yet well codified. The management of oral mucosal hemangiomas varies according to the patient’s age, the size and location of the lesion, as well as the clinical characteristics of the hemangioma. 7 Several therapeutic methods have been reported in the literature: propranolol, topical application of glucocorticoids, topical application of interferon-alpha, laser ablation, cryotherapy, serotherapy, radiotherapy, and surgery. 5 Surgical removal of these lesions can result in serious complications, such as significant bleeding. In addition, there is a risk of postoperative recurrence. 12 All reported cases of tonsillar hemangiomas in the literature have been treated surgically (tonsillectomy), with good outcomes.7,8 In our patient, the hemangioma was pedunculated, arising from the superior pole of the left palatine tonsil but independent of the tonsillar parenchyma. We performed a tumor excision after double ligation and sectioning of the pedicle, without incident.
Cavernous hemangioma is associated with a higher risk of postoperative recurrence, making extended follow-up of the affected site necessary. 4 The ENT surgeon should be aware of this entity, especially in children, due to the high frequency of hemangiomas in this age group and the common practice of tonsillectomy.
Conclusion
Tonsillar hemangiomas are a rare clinical entity that all ENT surgeons should be familiar with to make informed therapeutic decisions and avoid hemorrhagic complications and recurrence. It often presents a diagnostic challenge for clinicians, requiring a biopsy of the lesion to establish a definitive diagnosis. Accurate clinical diagnosis and thorough preoperative evaluation are crucial for the effective management of these vascular tumors.
Footnotes
Author Contributions
Amani Hachicha was a doctor in charge of a patient, initiated the study, and wrote the manuscript.
Rania Lajilia wrote and edited the manuscript.
Sarra Ben Rjeb was the doctor specialized in histopathology who performed the microscopic examination
Senda Turki wrote and edited the manuscript.
All authors read and approved the final manuscript.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and its Supplemental Figures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The ethics approval is not required for case reports deemed not to constitute research at my institution “Hospital of FSI Tunis, Tunisia.”
Consent for Publication
Written informed consent for publication of the patient’s clinical details and clinical images was obtained from the patient.