
Abstract

Harold Schuknecht was born in 1917 in South Dakota (Figure 1). 1 An otologic surgeon, otopathologist, and research director, his extensive otologic research career spanned from the 1940s until the 1990s. He finished his undergraduate studies at the University of South Dakota, medical school at Rush Medical College in Chicago, an internship in Des Moines, Iowa, and finished his otolaryngology residency at the University of Chicago in 1949. 2 Schuknecht’s first otopathology exposure was with his mentors at the University of Chicago, where he worked under John Lindsay, Henry Perlman, Heinz Kobrak, and William Neck. 2 It was with John Lindsay that Schuknecht saw the “logical continuity” of otopathology with an innovative clinical practice. 2 Starting as fulltime faculty at the University of Chicago, he progressed to Henry Ford Hospital in Michigan in 1953. 2 In 1961, he was recruited to the Chair of the Department of Otology and Laryngology at Harvard Medical School and Chief of Otolaryngology at Massachusetts Eye and Ear Infirmary. 2 Eventually, it was at Massachusetts Eye and Ear Infirmary that he conducted much of his pioneering work in otopathology for which he is remembered. 1 His weekly “Sunday School” otopathology study sessions there are still fondly recalled. 2 Joseph Nadol summed it up perfectly: “. . . Schuknecht reestablished the histologic and scientific basis for modern medical and surgical otologic intervention, based on his lifelong studies of human temporal bones.” 2
Harold Schuknecht at Massachusetts Eye and Ear Infirmary in an undated photograph—detail by Miriam Redleaf, July 19, 2022.
Schuknecht’s experience in clinical otology enabled him to pair patient conditions with otopathologic analysis. One description from his Henry Ford Hospital days is typical of his eloquence and insight (Figure 2): Primary neural degeneration without haircell degeneration, or neural presbycusis. The horizontal sections show the 8th nerve present in the internal auditory meatus. Reissner’s membrane and the stria vascularis appear normal. The supporting cells of the organ of Corti are shrunken, but the hair cells are present and probably normal. There is a patchy ganglion cell loss of about 5% in both upper and lower basal turns. The maculae of the utricle and saccule and all of the cristae are normal.
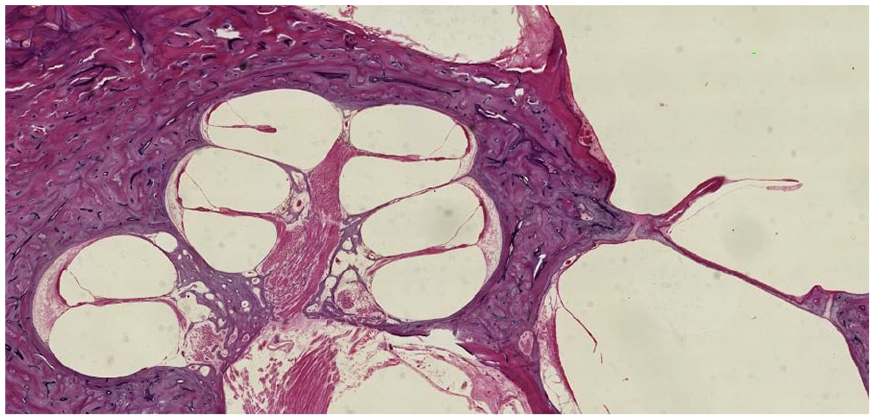
H & E of mid-modiolar section—a Henry Ford Hospital patient with neural presbycusis as described by Dr. Schuknecht—showing the cochlea, internal auditory canal with auditory nerve, cochleiform process, and stapes footplate—University of Chicago Lindsay Otopathology Laboratory and Archives, January 14, 2025.
This pairing of clinical experience with otopathology enabled him to create stapes prostheses, to devise the tympanomastoidectomy, and to revise labyrinthectomy in Meniere disease. 2 But Schuknecht is best known today for his correlations of otopathologic findings to the clinical presentations of diseases—such as Meniere disease, presbycusis, otosclerosis, and benign paroxysmal positional vertigo. 2 His textbook Pathology of the Ear is still widely referenced today. 3
Temporal bone histopathology was first developed in Europe in the late 19th century, creating complex sample extraction and fixation techniques which accommodated the delicate labyrinthine structures housed in the depths of rigid bone. 4 The first temporal bone laboratory in the United States was established at Johns Hopkins in 1924, driven by the work of Samuel Crowe and Stacy Guild. 5 The second temporal bone laboratory in the United States began at the University of Chicago under John Lindsay, which collected its first specimens in 1930. Schuknecht, who had trained under Guild, eventually founded his own otopathology laboratory at Massachusetts Eye and Ear in 1961. 4
Once a feature of every mid-20th century Otolaryngology department, today there are few temporal bone otopathology laboratories. Only 6 active otopathology laboratories remain in the United States: Johns Hopkins University, Massachusetts Eye and Ear Infirmary, Stanford University, the University of California Los Angeles, the University of Chicago Lindsay Otopathology Archives, and the University of Minnesota. The archival material housed in these collections remains an irreplaceable resource for demonstrating the anatomy and cellular structure of temporal bone contents. In few organs is the relationship between structure and function so legible as in the inner ear. While other organs may be indifferent to variations in microscopic details of geometry with only minimal physiologic consequences, the inner ear’s role as waveguide and mechanical sensor makes it uniquely amenable to analysis of angles and dimensions at the length scales best illustrated by histopathology. Therefore, otopathology remains a fundamental tool for understanding inner ear anatomy and physiology. Furthermore, existing samples have the potential to reveal new information when explored with recently developed techniques in optical microscopy, biochemistry, or molecular biology.
It is critical that the opportunities afforded by Schuknecht’s contributions, as well as those of countless other researchers and donors, be recognized as an irreplaceable resource and be scrupulously preserved. Schuknecht died in 1996 in Boston after a cerebrovascular event. 6 Schuknecht requested there be no memorial service in his memory. However, at his bequest, he donated his own temporal bones to the otopathologic process which he had championed for decades (Figure 3).
Dr. Schuknecht’s own processed temporal bones—Miriam Redleaf, July 19, 2022.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.