
Abstract

Transoral robotic surgery (TORS) for the treatment of oropharyngeal cancer has become centered at tertiary referral centers. 1 To avoid treatment delays or multiple anesthetics, the need for repeat operative endoscopy may be questioned when the diagnosis has been made at an outside institution. However, inadequate visualization of relevant anatomy can preclude TORS candidacy and may lead to procedure abortion or conversion to an open technique.2,3 To evaluate this dilemma, we explored the ability to assess oropharyngeal exposure for TORS candidacy via operative endoscopic photo-documentation.
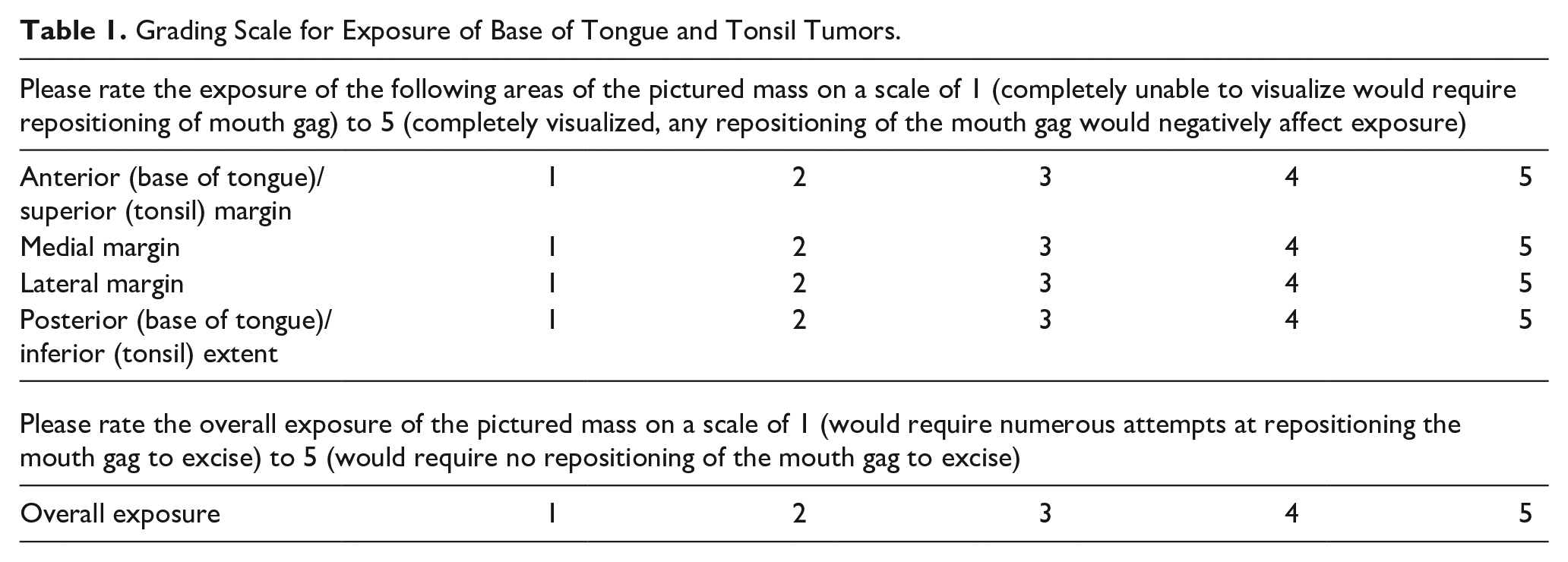
Prior to offering TORS as a primary treatment modality at our tertiary center, we frequently simulated oropharyngeal exposure during staging endoscopy. At this time, photo documentation of the exposure using multiple retractors in different positions is obtained. We retrospectively identified 19 patients between 7/1/18 and 7/1/20 who had their most ideal exposure photographed at 3 depths within the aerodigestive tract, and with the retractor in 2 discrete positions: tongue positioned midline, under the tongue blade (In), and pulled contralateral from the lesion of interest from under the tongue blade (Out). All exposures were obtained using the Medrobotics Flex Retractor System. The exposure obtained with each technique was then evaluated by 4 fellowship-trained head and neck surgeons, blinded to patient and technique. They used A novel grading scale on an electronic-based survey was used to assess the adequacy of exposure to a base of tongue and tonsil tumors (Table 1).
Grading Scale for Exposure of Base of Tongue and Tonsil Tumors.
Our primary outcome measure was surgeon agreement on the overall adequacy of oropharyngeal exposure. Secondary outcome measures included agreement on exposure of tumor margins and comparison of exposure technique on overall exposure and tumor margins. The kappa test for agreement was used to assess agreement in grading between reviewers when considering the exposure grades in the ordinal scale. This test grades agreement as perfect (0.80 < kappa 1.00), substantial (0.60 < kappa 0.80), moderate (0.40 < kappa 0.60), fair (0.20 < kappa < 0.40), and poor or no agreement (kappa 0.20).
Surgeons were surveyed on the adequacy of oropharyngeal exposure of 19 malignancies using the original scale. The majority (n = 13; 72%) of patients with oropharyngeal cancer presented with early-stage tumors (clinical T-stage 1 or 2). Fair agreement was seen for an overall exposure score of 5 (kappa = 0.254; P < .001). A similar agreement was seen at the anterior/superior margin (kappa = 0.264; P < .001) and inferior/posterior margin (kappa = 0.2786; P < .001) when exposure could be considered ideal. Poor or slight agreement was seen for exposure grades of 5 of lateral margins (kappa = 0.137; P < .001) and grades of 1 of the inferior/posterior margin (kappa = 0.0932; P = .0157) and overall exposure (kappa = 0.0952; P = .0140). We did not find any moderate, substantial, or perfect agreement (Table 2).
Observer Agreement Results.
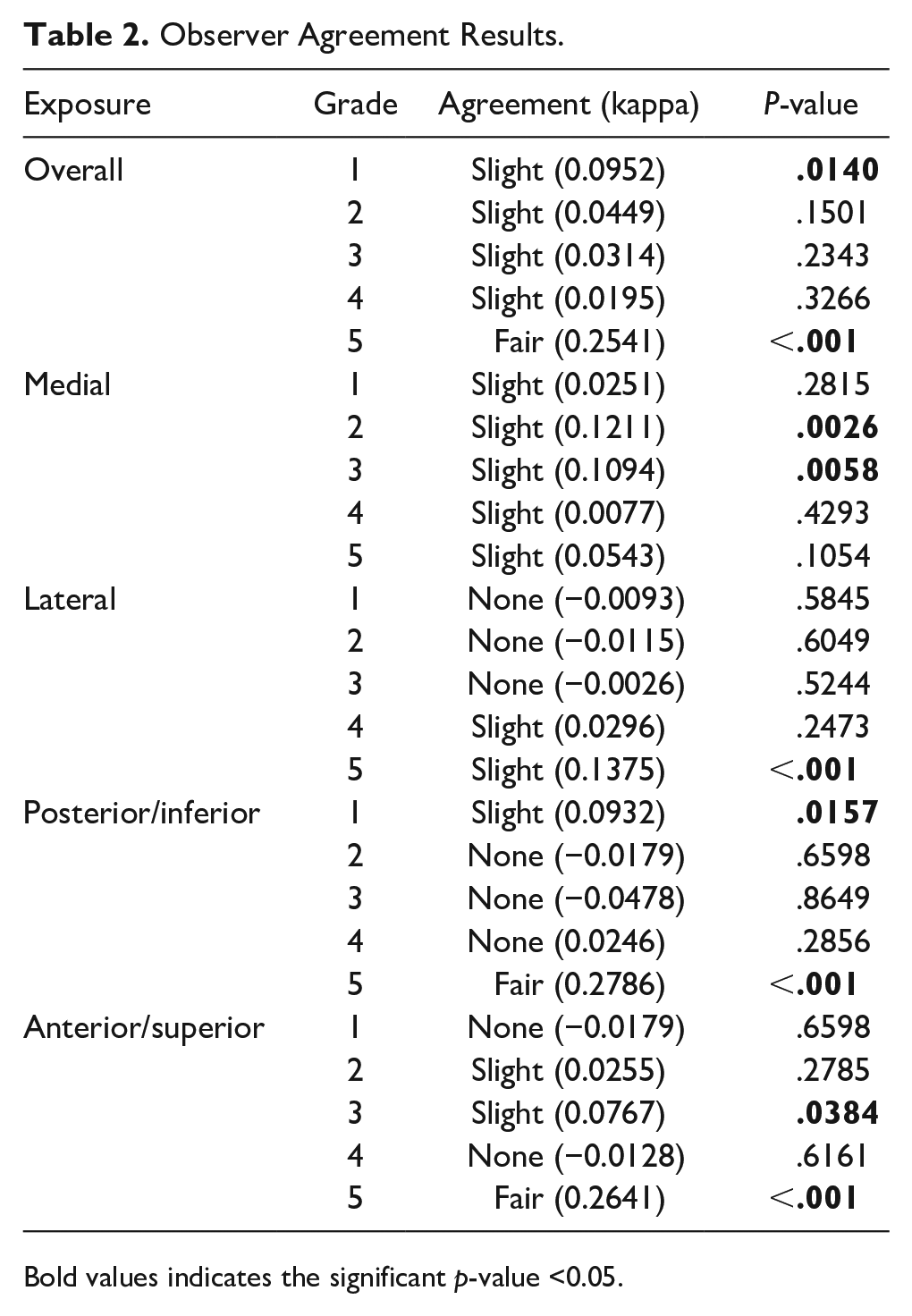
Bold values indicates the significant p-value <0.05.
Half of the patients with a cancer diagnosis (n = 9) were offered TORS, of whom 4 underwent surgery as a primary treatment. Candidacy was determined based on the surgeon’s assessment of oropharyngeal exposure at the time of staging endoscopy as well as discussion at a multidisciplinary tumor board. There were no significant differences in the median age (64.4 years vs 62.8 years; P = .757) or BMI (27.4 kg/m2 vs 27.5 kg/m2; P = .970) between the patients who were offered TORS as a treatment modality and those deemed not surgical candidates. Patients offered TORS had a lower average Mallampati score (2.00 vs 2.63); however, statistical significance is weak (P = .058). All TORS candidates (n = 9) were early tumor stage (T1 or T2) compared to 4 out 9 of non-candidates (P = .0294). All patients undergoing TORS were resected with clear margins.
Subgroup analysis was performed for each tumor subsite. There were no statistically significant differences between exposure techniques for tonsil tumors. For the base of tongue tumors reviewers favored the “In” technique to expose the lateral tumor margin [median (IQR) score “In”: 4 (3.75-4.25) vs “Out”: 3.25 (2.75-4); P = .050] though no differences were found for the anterior, medial, and posterior margins or overall exposure.
Our experience suggests that oropharyngeal exposure and TORS respectability are largely surgeon-dependent. When surveyed, only fair agreement could be seen among surgeons when exposure could be considered ideal. This interobserver variability on the adequacy of exposure suggests that TORS candidacy is surgeon dependent and should be determined via operative endoscopy by the resecting surgeon. When obtaining exposure to the base of tongue tumors, midline positioning of the tongue is one way surgeons may improve visualization of the lateral aspect of the malignancy in certain patients.
Footnotes
Authors’ Note
This work was presented as a poster at the American Head and Neck Society Annual Meeting, Virtual, July 22-25, 2021.
Data Availability Statement
Patient data will not be shared with third parties.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
This study received ethical approval from the EVMS IRB (approval #20-10-XX-0229) on June 07, 2021. This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required.