
Abstract
Retropharyngeal infiltrative intramuscular lipomas are rare, and only 2 cases have been reported. Surgical resection is technically challenging owing to anatomical constraints, with no established optimal approach. Furthermore, the risk of recurrence is high. Herein, we report a novel, minimally invasive, and effective surgical approach for retropharyngeal infiltrative intramuscular lipoma. A 75-year-old woman presented with snoring as the chief complaint. Magnetic resonance imaging revealed a 52 × 38 mm lipoma in the retropharyngeal space with infiltration into the longus capitis muscle. A combined transoral and transnasal approach using existing endoscopic instruments enabled complete tumor resection with enhanced visualization and minimal invasiveness. Postoperative histopathological examination confirmed the diagnosis of infiltrative intramuscular lipoma. One year postoperatively, no recurrence was observed, and the patient will continue long-term follow-up. Infiltrative intramuscular lipomas are associated with a high risk of recurrence, and wide excision of the infiltrated area is required to achieve clear margins. Therefore, a surgical approach that balances complete resection with minimal invasiveness is required. The combined transoral and transnasal approach offers a cost-effective, minimally invasive, and precise method for resecting retropharyngeal infiltrative intramuscular lipomas.
Keywords
Introduction
Retropharyngeal lipomas are rare, and their deep location often delays diagnosis until the tumor becomes large and symptomatic.1,2 Intramuscular lipomas account for <1% of all lipomas, 3 and infiltrative intramuscular lipomas are particularly significant because of their potential for recurrence 4 and the difficulty in differentiating them from atypical lipomatous tumors (ALT). 5 Surgical resection is technically challenging owing to anatomical constraints, with no established optimal approach. Furthermore, the risk of recurrence is high, and a wide excision including the surrounding infiltrated muscle tissue is recommended.6,7 This report presents the case of an older woman with an infiltrative intramuscular lipoma in the retropharyngeal space that was treated using a minimally invasive approach.
Case Presentation
A 75-year-old woman presented to our department with a 2-year history of snoring. Flexible laryngoscopy revealed a smooth, painless submucosal mass along the posterior wall, extending from the nasopharynx to the oropharynx (Figure 1a,b), with significant narrowing of the upper airway. Magnetic resonance imaging (MRI) revealed a 52 × 38 mm mass with high signal intensity on T1-weighted images (Figure 1c) and low signal intensity on contrast-enhanced fat-suppressed T1-weighted images (Figure 1d), suggesting a lipomatous lesion.
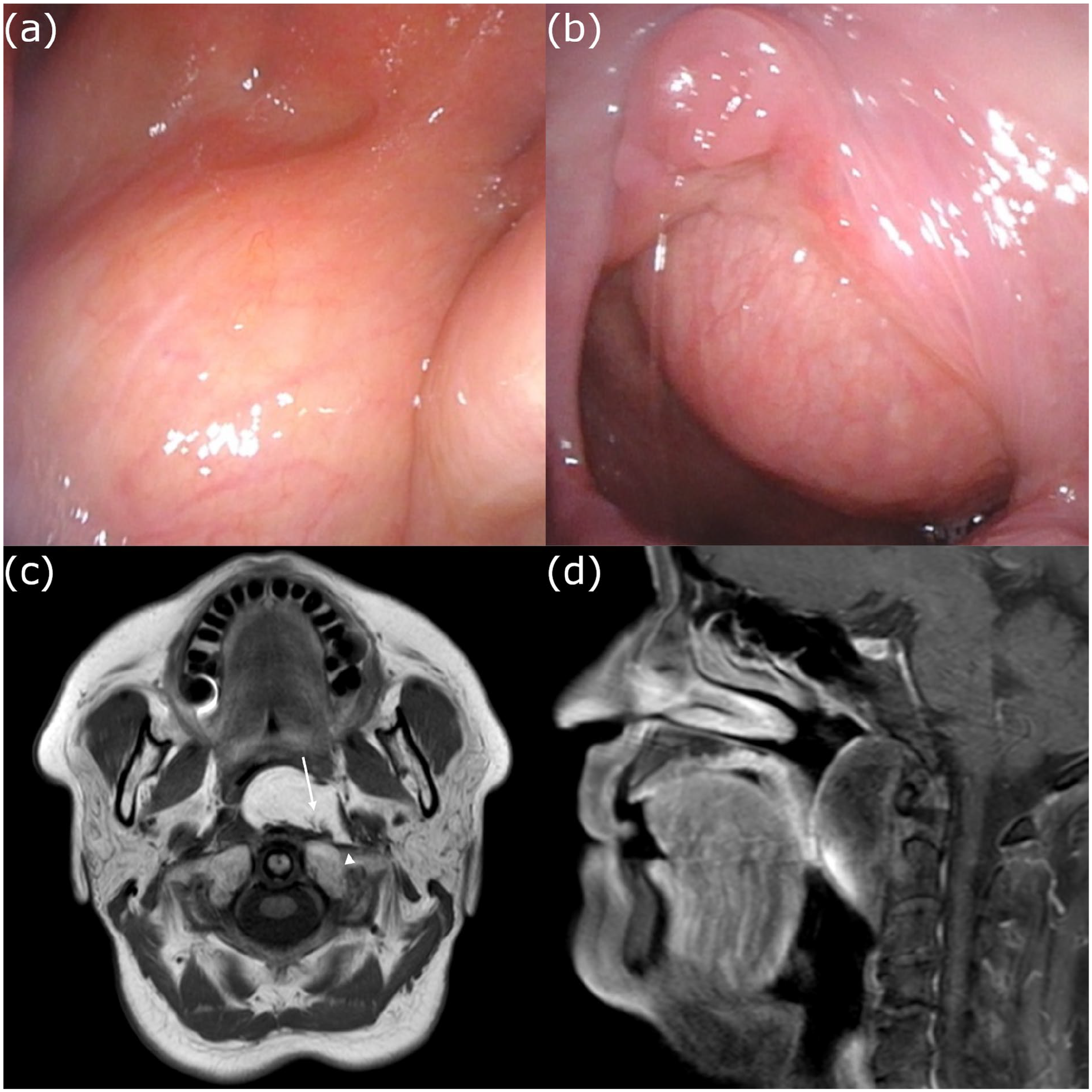
(a) A smooth submucosal mass is observed along the posterior wall of the nasopharynx. (b) Continuation of the mass into the oropharynx. (c) T1-weighted magnetic resonance image shows a 52 × 38 mm lipomatous mass in the retropharyngeal space with high signal intensity. The mass infiltrates the longus capitis muscle (arrowhead), with indistinct margins and muscle tissue within the tumor (arrow), suggesting muscle infiltration. (d) Contrast-enhanced fat-suppressed T1-weighted magnetic resonance image shows low signal intensity in the mass, which extends from the nasopharynx to the oropharynx.
The mass infiltrated the longus capitis muscle (arrowhead, Figure 1c) and had indistinct margins and a signal intensity consistent with that of the muscle tissue within the tumor (arrow, Figure 1c). Based on these findings, a preoperative diagnosis of infiltrative intramuscular lipoma was made. In addition, the patient (body mass index, 29.1 kg/m2) was diagnosed with obstructive sleep apnea (OSA) syndrome due to obesity, airway narrowing, and elevated respiratory event index (REI) values of 53.1 and 44.5 events per hour on 2 consecutive nights, respectively.
Surgical Planning
Surgical treatment was planned to establish a definitive diagnosis of the tumor and alleviate symptoms. Most of the mass was located along the midline in the retropharyngeal space, extending from the nasopharynx to the oropharynx. A minimally invasive combined transoral and transnasal approach was planned to optimize visualization and accessibility by using the standard endoscopic equipment routinely used for endoscopic sinus surgery and tonsillectomy.
Surgical Procedure
A transoral approach was initially used, and a mouth gag was used to secure the surgical field similar to that for tonsillectomy (Figure 2a). Incision of the pharyngeal mucosa revealed a soft, encapsulated lipomatous mass directly beneath it (Figure 2b), allowing easy dissection of the caudal two-thirds under direct visualization (Figure 2c).
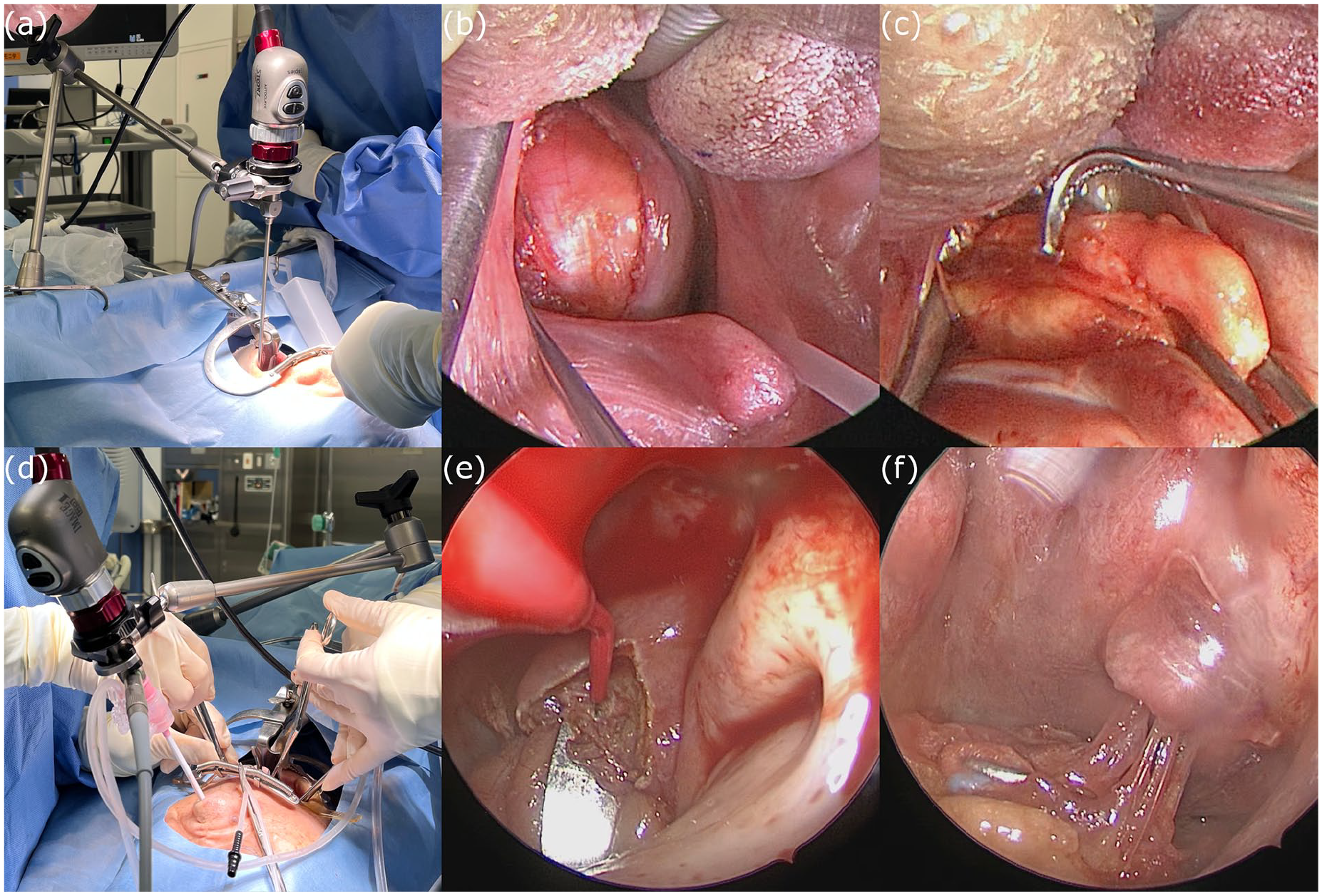
(a) Transoral approach with a mouth gag providing a surgical field similar to that for tonsillectomy. (b) A soft, lipomatous mass covered by a thin capsule is observed beneath the pharyngeal mucosa. (c) The caudal two-thirds of the encapsulated tumor are dissected under direct visualization. (d) The transnasal approach, with the endoscope inserted transnasally and the mouth gag maintained for countertraction. (e) The superior margin of the tumor is confirmed by incising the superior pharyngeal constrictor muscle. (f) Tumor infiltration into the muscle tissue is clearly visualized endoscopically, and the infiltrated muscle is excised along with the tumor.
Owing to inadequate visualization of the nasopharynx via the transoral route, we transitioned to a transnasal approach for better accessibility. During this procedure, the surgeon was positioned on the patient’s right side, and the endoscope was inserted transnasally for direct visualization of the nasopharynx (Figure 2d). The continued use of the mouth gag allowed the assistant to retract the tumor through the oral cavity and provided effective countertraction during the procedure. A microdissection needle was used to incise the superior pharyngeal constrictor muscle and to confirm the superior margin of the tumor (Figure 2e). The capsule became progressively indistinct at the sites of muscle infiltration, which was consistent with the indistinct margins observed on MRI. Clear endoscopic visualization confirmed tumor infiltration into the muscle tissue, and the infiltrated muscle was excised along with the tumor (Figure 2f). The tumor was completely excised, and the pharyngeal mucosa was sutured to conclude the procedure. No intraoperative complications were observed.
Postoperative Course and Histopathological Findings
The patient reported minimal pain and achieved full oral intake on postoperative day 2. Postoperative monitoring revealed a reduction in the REI to 20.8 and 9.3 events per hour on 2 consecutive nights, respectively, indicating improvement from baseline.
At the 6-month follow-up, the absence of residual tumor was confirmed on MRI (Figure 3a and b), and endoscopy at 10 months demonstrated complete healing without scarring or inflammation (Figure 3c and d). No recurrence was observed after 1 year.
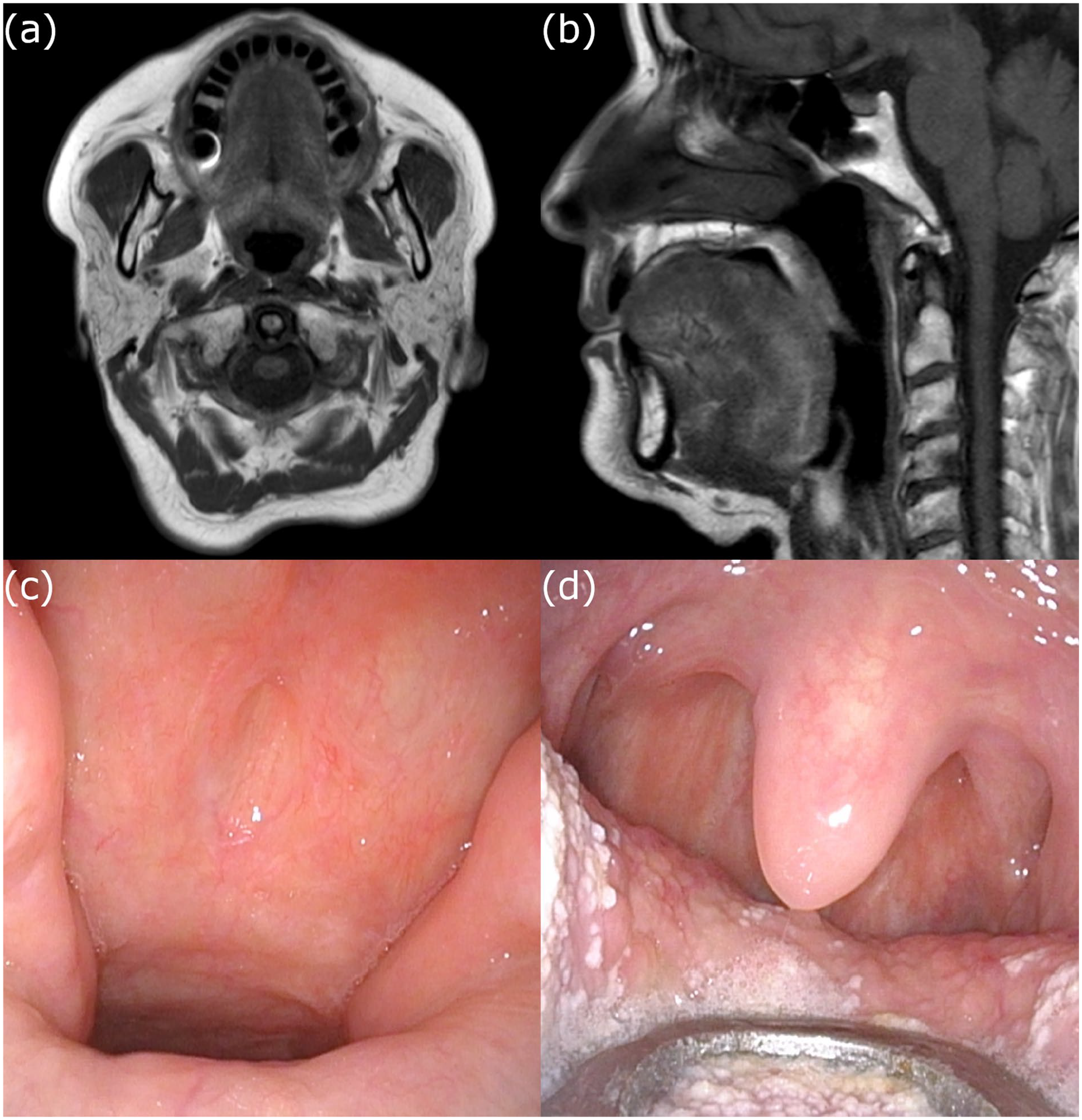
(a, b) T1-weighted axial and sagittal magnetic resonance images at postoperative 6 months show no evidence of residual tumor. (c, d) Endoscopic views of the nasopharynx and oropharynx at postoperative 10 months show complete mucosal healing without scarring or inflammation.
Macroscopic examination revealed a yellow soft-tissue tumor measuring 50 × 40 mm (Figure 4a). Histopathological evaluation revealed mature adipocytes (arrow, Figure 4b) interspersed with skeletal muscle fibers (arrowhead, Figure 4b), with no evidence of atypia, confirming the diagnosis of intramuscular lipoma.
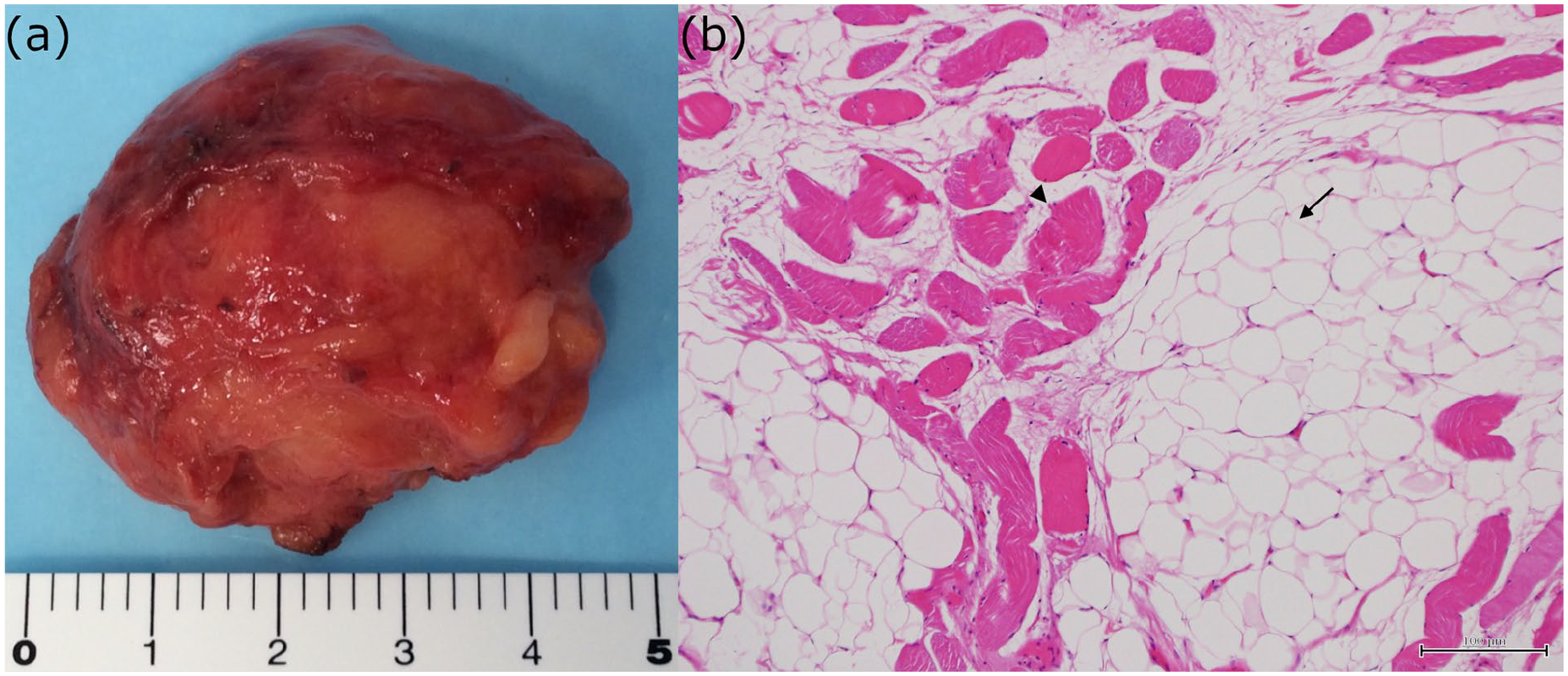
(a) Yellow soft tumor (50 × 40 mm) on macroscopic examination. (b) Photomicrograph of a hematoxylin and eosin stained section (×100 magnification) shows mature adipocytes (arrow) interspersed with skeletal muscle fibers (arrowhead).
Discussion
Anatomical Challenges Associated With Retropharyngeal Lipomas
Retropharyngeal lipomas are often diagnosed late because of their deep location and typically present with symptoms such as dysphagia, snoring, dyspnea, and OSA after significant enlargement.1,2 In our patient, a >50 mm tumor caused severe airway obstruction and OSA, consistent with previous reports in which surgical resection alleviated symptoms.7,8 These findings highlight the importance of early detection and surgical intervention in such patients.
Surgical Approaches to Retropharyngeal Lipomas
The transoral approach offers direct access to the tumor but provides limited visualization of the superior nasopharynx. In our patient, the addition of a transnasal endoscopic technique enhanced visualization and enabled complete resection without the need for a transcervical incision.
Transcervical excision is the most commonly used approach for the treatment of retropharyngeal lipomas. 2 Regarding retropharyngeal infiltrative intramuscular lipomas, only 2 cases have been reported, and both were treated with transcervical excision.7,9 However, a minimally invasive approach is preferred when feasible, as it generally reduces surgical morbidity and provides aesthetic advantages. Nonetheless, for tumors with extensive lateral extension, particularly those near the carotid sheath, or for large tumors that cannot be removed through a small transoral incision, a transcervical approach may be necessary to achieve complete resection. 2
Advances in endoscopic sinus surgery and standardized otolaryngology equipment have increased the feasibility of the transoral approach for treating larger tumors. In our patient, the wide-angle view provided by the 0° endoscope ensured sufficient visualization despite the lateral extension. This finding suggests the potential utility of angled endoscopes in addressing laterally extended tumors.
Histological Features of Infiltrating Intramuscular Lipomas
Intramuscular lipomas are exceptionally rare and account for <1% of all lipomas. A previous study reported only 3 cases among the 707 examined lipomas. 3
The infiltrative nature of intramuscular lipomas necessitates careful management to prevent recurrence. The recurrence rates of these tumors range from 4% to 19%,4,5 with recurrences reported between 3 and 6 years after surgery.4,9 To minimize the risk of recurrence, wide excision of the infiltrative components and marginal resection of the encapsulated areas are crucial.6,7 Moreover, long-term follow-up incorporating both endoscopic examination and MRI is essential to monitor recurrence.
Differentiating infiltrative intramuscular lipomas from ALT remains challenging. ALT and well-differentiated liposarcomas are histologically identical tumors that are classified differently based on their anatomical location and resectability. 10 Fat-suppressed T1-weighted MRI with septal contrast enhancement can provide valuable clues; however, definitive diagnosis requires a histopathological evaluation. 11
The diagnostic challenges and risk of recurrence highlight the need for precise surgical techniques for effective management of intramuscular lipomas. Although transoral robotic surgery is an effective method for treating retropharyngeal intramuscular lipomas, its high cost and associated limitations, including the need for specialized equipment and training, 12 raise questions about its cost-effectiveness. 2 In contrast, in our patient, the use of standard endoscopic equipment allowed for complete tumor excision and demonstrated its practicality, especially in resource-limited settings where cost constraints are significant.
Limitations
Although the combined transoral and transnasal approach was effective in our patient, it has certain limitations. Tumors with extensive lateral extension beyond the reach of standard endoscopic tools may require a transcervical approach for complete resection. Additionally, because this is a single-case report, the findings may not be generalizable. Further studies with a larger number of cases are needed to assess the effectiveness of this approach, better understand the risk of recurrence, and refine surgical protocols. Factors such as tumor size, location, and surgeon’s experience are important considerations for future evaluation.
Conclusion
Retropharyngeal infiltrative intramuscular lipomas are exceedingly rare, and this case demonstrates the efficacy of a minimally invasive combined transoral and transnasal approach, which allows safe and complete tumor excision while avoiding transcervical incision and reducing postoperative morbidity. This approach is a cost-effective alternative to conventional methods that combines minimal invasiveness with effective outcomes. Future studies should use this approach in larger cohorts and compare its outcomes with those of conventional methods.
Footnotes
Data Availability Statement
The data supporting this case report are not publicly available due to patient confidentiality and privacy concerns. Further information is available from the corresponding author upon reasonable request, subject to institutional and ethical approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval for this case report was obtained from the Juntendo University Ethics Committee.
Consent to Participate
Not applicable.
Consent for Publication
Written informed consent was obtained from the patient for the publication of anonymized information in this article.