
Abstract

Significance Statement
Salivary gland tumors may arise anywhere in the oral cavity and oropharynx, but tonsillar location is extremely rare. We present an unusual case of mucoepidermoid cancer of the right palatine tonsil in a female patient who presented with atypical symptoms of globus sensation without a clinically obvious lesion resulting in delayed diagnosis. The patient was treated with tonsillectomy and postoperative radiotherapy with satisfactory outcomes over a 2-year follow-up period.
Case Presentation
A 49-year-old female presented to the ENT outpatient clinic with a three-month history of globus sensation. The patient reported no other symptoms including pain, dysphagia, otalgia, or hoarseness. There was no relevant medical, social, or family history. The patient had previously visited other ENT specialists over a period of three months, but no diagnosis was made.
Clinical examination including flexible fiberoptic laryngoscopy was normal (Figure 1). There were no abnormal cervical lymph nodes on palpation. Considering the presence of persistent symptoms, a magnetic resonance imaging with contrast was arranged revealing swelling in the area of the right palatine tonsil with a maximum diameter of approximately 1.4 cm (Figure 1). The lesion appeared to have not well-defined margins and vascularity similar to that of the surrounding healthy tissue. The patient underwent bilateral diagnostic tonsillectomy. Histopathological report described findings compatible with intermediate-grade mucoepidermoid carcinoma (MEC) arising from the surface of the right palatine tonsil, probably derived from minor salivary glands (Figure 2). No perineural or vascular invasion was observed, while both p16 and p63 markers were positive (Figure 3).
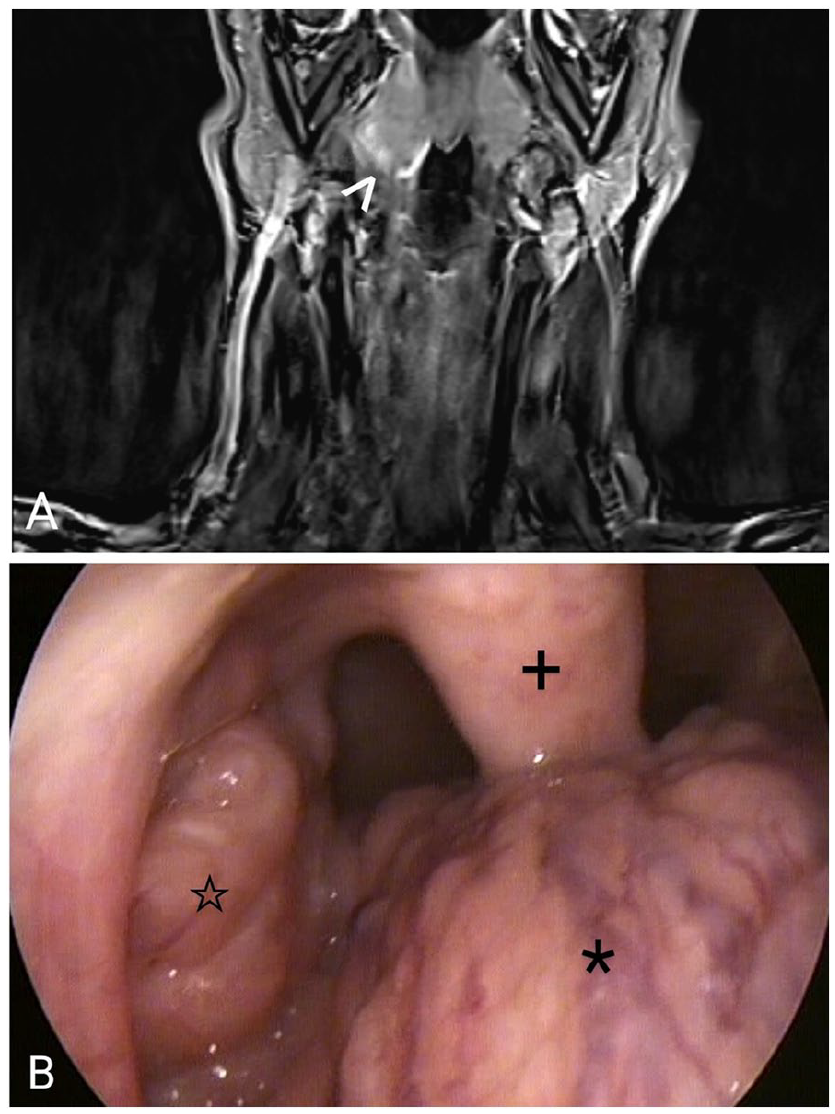
(Α) Coronal view of T1-weighted magnetic resonance imaging showing a tonsilar lesion (>). (B) Preoperative imaging of the oropharynx showing a normal-looking right tonsil (large asterisk); +: uvula, *: lingual tonsil.

High-power hematoxylin and eosin (H&E) stain demonstrates: (A) Epidermoid cell nests and cystic spaces (>) lined by epidermoid and rarely mucous cells (*) lying adjacent to bundles of skeletal muscle fibers (¤). (B) The cystic component of the carcinoma (+) invading (arrow) skeletal muscle fibers (¤). [100× magnification].

(A) Normal surface squamous epithelium of the palatine tonsil (arrow) and neoplastic cystic spaces (>) lined by epidermoid cells are positive for p63 immunostain [50× magnification]. (B) Epidermoid cell nests and cystic spaces lined by epidermoid cells show strong positivity for p16 immunostain (»), demonstrating the epidermoid component of the neoplasm [200× magnification]. (C) Cystic spaces (*) lined by mucous cells show positivity for cytokeratin 7 immunostain, demonstrating the mucous component of the neoplasm [100× magnification].
Following discussion at the multidisciplinary head and neck oncology team meeting, a positron emission tomography/computed tomography scan was performed. The scan detected hypermetabolic lesions at the anatomic site of the right tonsillar bed, extending from the lateral oropharynx to the level of the right epiglottic vallecula, suggestive of either residual cancerous tissue or postoperative inflammation. No distant metastases were identified. Based on the above results, the patient underwent a revision operation and multiple biopsies from the surrounding tissue were taken to ensure clear margins, all of which were normal. The patient received adjuvant radiotherapy in the palatine tonsils and bilateral cervical lymph nodes. There were no signs of tumor recurrence at 24-month follow-up.
MEC is one of the most common malignancies in both major and minor salivary glands and arises from the reserve cells of salivary excretory ducts. Parotid gland MEC represents approximately 56.8% of all cases, with females affected more than males. 1 On the other hand, the palate, buccal mucosa, tongue, and gingiva are the most common sites for MEC of the minor salivary glands. 1 Various malignant tumors may arise from the palatine tonsil, with squamous cell carcinoma and diffuse large B-cell lymphoma the most commonly seen. 2 In contrast, despite the presence of minor salivary glands in the palatine tonsils, only a few cases of tonsillar MEC have been reported in the literature. 3
Histologically, MEC is characterized by mucous, intermediate, and epidermoid cells. According to histopathological features such as necrosis, mitosis, and anaplasia, and the relationship among its cellular components, MEC is classified as low-, intermediate-, and high-grade. Clinical presentation usually includes pain, dysphagia, or referred otalgia, but atypical symptoms can also be present. Furthermore, the lesion may often be small and barely visible on clinical examination, and, therefore, early detection without imaging can be difficult. This happened in our case, where globus sensation was the only symptom, and there were no abnormal clinical findings, thus, early suspicion of underlying pathology was challenging. The role of imaging as part of further investigation for patients with persistent atypical symptoms is crucial.
Minor salivary gland carcinomas are often difficult to manage. The gold standard in the treatment approach for MEC consists of total tumor excision. Prophylactic neck dissection is also suggested by some authors in high-grade and clinical T3 or T4 tumors. 4 In the case of perineural invasion, positive lymph nodes, advanced high-grade tumors, or unclear surgical margins, adjuvant radiotherapy is also recommended. On the other hand, chemotherapy is generally adopted in palliative management of inoperable tumors. 5
Low- and intermediate-grade tumors demonstrate favorable outcomes, whereas high-grade carcinomas are highly aggressive with worse prognosis and mortality rates. Despite its rare occurrence in the palatine tonsil, MEC should be considered in differential diagnosis, as early recognition and appropriate management are the determining factors in the prognosis of these malignancies.
Footnotes
Acknowledgements
None.
Author Contributions
Conceptualization, K.C..; methodology, K.C., M.K., S.P.; investigation, K.C., M.S., S.P.; resources, K.C., M.K.; data curation, K.C., M.K., M.S., M.K., S.P.; writing-original draft preparation, K.C., M.K.; writing-review and editing, M.S., M.K., S.P.; supervision, S.P. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for Publication
Written informed consent was obtained from the patient for anonymized patient information and images to be published in this article.