
Abstract

Significance Statement
Adenoid cystic carcinoma is a relatively rare epithelial tumor that typically originates in the salivary glands, including the submandibular and minor salivary glands. However, it may occasionally arise in other locations, such as the breast, Bartholin glands, skin, and trachea. Tracheal adenoid cystic carcinoma is a rare, low-grade malignant tumor originating from the glands of the tracheal and bronchial walls. It rarely involves the thyroid, which can lead to misdiagnosis as thyroid cancer.
A 50-year-old female patient with no known comorbidities presented to the otolaryngology clinic with complaints of progressive neck swelling and shortness of breath. Neck ultrasonography revealed a hypoechoic, vascularized mass lesion located in the midline of the neck, occupying the right thyroid lobe. Contrast-enhanced magnetic resonance imaging (MRI) of the neck was performed for further evaluation. MRI revealed a space-occupying lesion originating from the right lateral wall of the trachea at the supraglottic level, extending into the right thyroid lobe and isthmus, and invading the right vocal cord (Figure 1). Positron emission tomography-computed tomography showed hypermetabolic involvement of the trachea’s right lateral wall, the right vocal cord, and the thyroid lobe (Figure 2). Additionally, multiple subcentimeter hypermetabolic nodular lesions were observed in both lungs (Figure 2). A tru-cut biopsy of the right thyroid lobe was performed, and the pathological examination revealed ductal and myoepithelial cells forming cribriform patterns in a hyalinized stroma. Immunohistochemical analysis showed that ductal epithelial cells were positive for pan-cytokeratin (CK), CK7, and CD117, while myoepithelial cells were positive for vimentin and S-100 (Figure 3). Based on imaging and histopathological findings, a diagnosis of primary adenoid cystic carcinoma (ACC) originating from the trachea was established. In adults, most primary tracheal tumors are malignant, with approximately two-thirds being squamous cell carcinomas. ACC accounts for about 10% to 15% of cases, making it the second most common type. 1 Tracheal adenoid cystic carcinoma (TACC) is most commonly located in the upper trachea, particularly in the posterior cartilage of the trachea. Primary TACC often metastasizes to the lungs and bones. 2 TACC is rare and often diagnosed late because its symptoms are nonspecific and insidious. These tumors are frequently misdiagnosed and may not present symptoms until they occlude 75% of the tracheal lumen. 3 As in our case, TACC involving the thyroid is even rarer. In patients with thyroid masses, the presence of tracheal lesions or a history of ACC should raise suspicion of TACC metastasis to the thyroid. Comprehensive investigations are essential to identify any metastatic involvement. Advanced imaging and pathological evaluation are crucial for establishing an accurate preoperative diagnosis and developing an effective treatment plan. Surgical resection remains the primary treatment for TACC and has been shown to improve survival. 4 In recent years, adjuvant therapies, such as radiotherapy and chemotherapy, have demonstrated some therapeutic benefits. Radiotherapy may be used to treat inoperable cases; however, its efficacy remains uncertain. This case highlights the importance of considering TACC as a differential diagnosis in patients with thyroid masses, particularly those with a history of tracheal lesions or ACC. Prompt and thorough diagnostic approaches are vital for early.
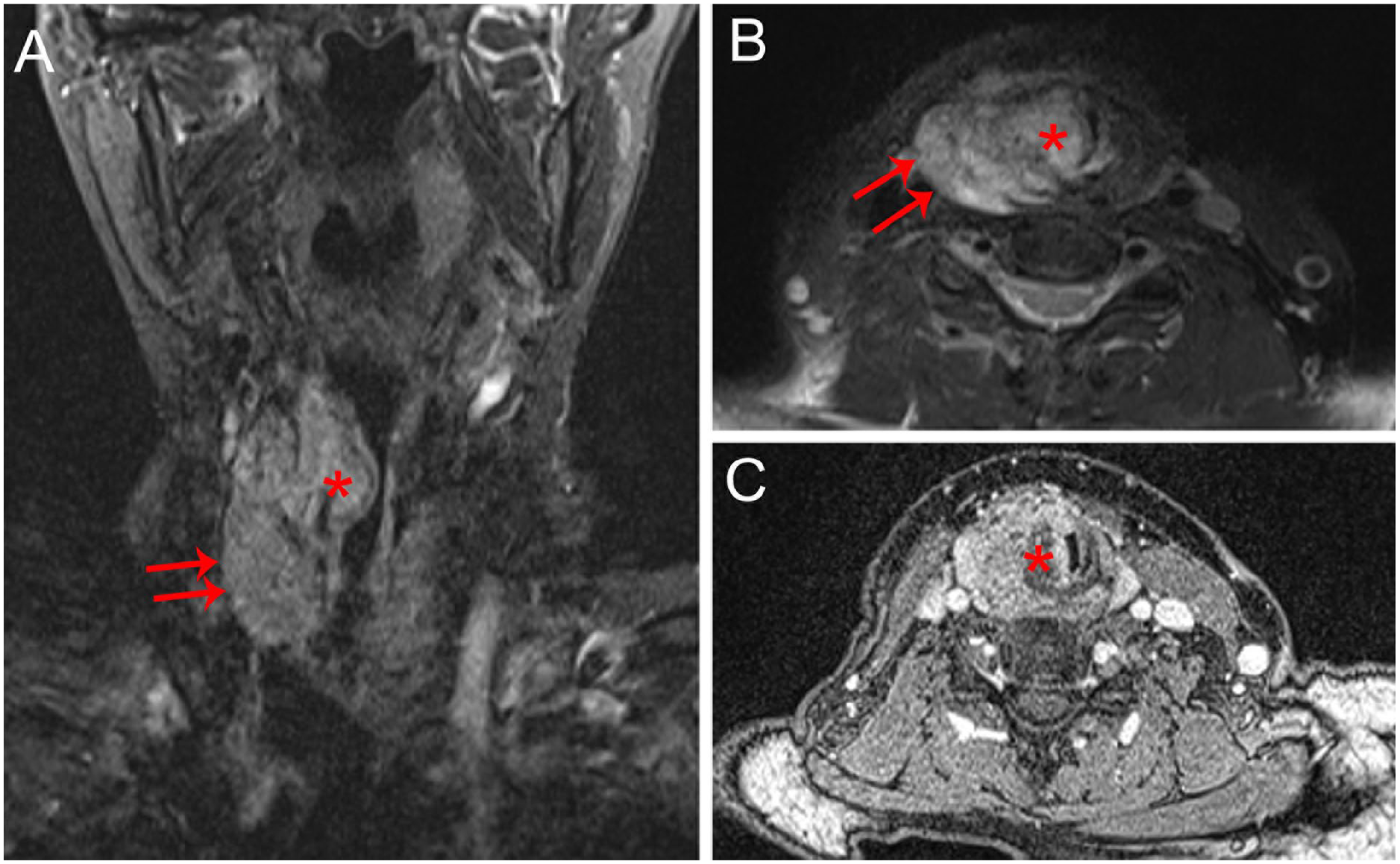
T2-weighted images of coronal (A) and axial (B) sections show a heterogeneous hyperintense mass (asteriks). The lesion extends into the right thyroid lobe (arrows). Postcontrast axial (C) section shows significant contrast enhancement (asteriks).
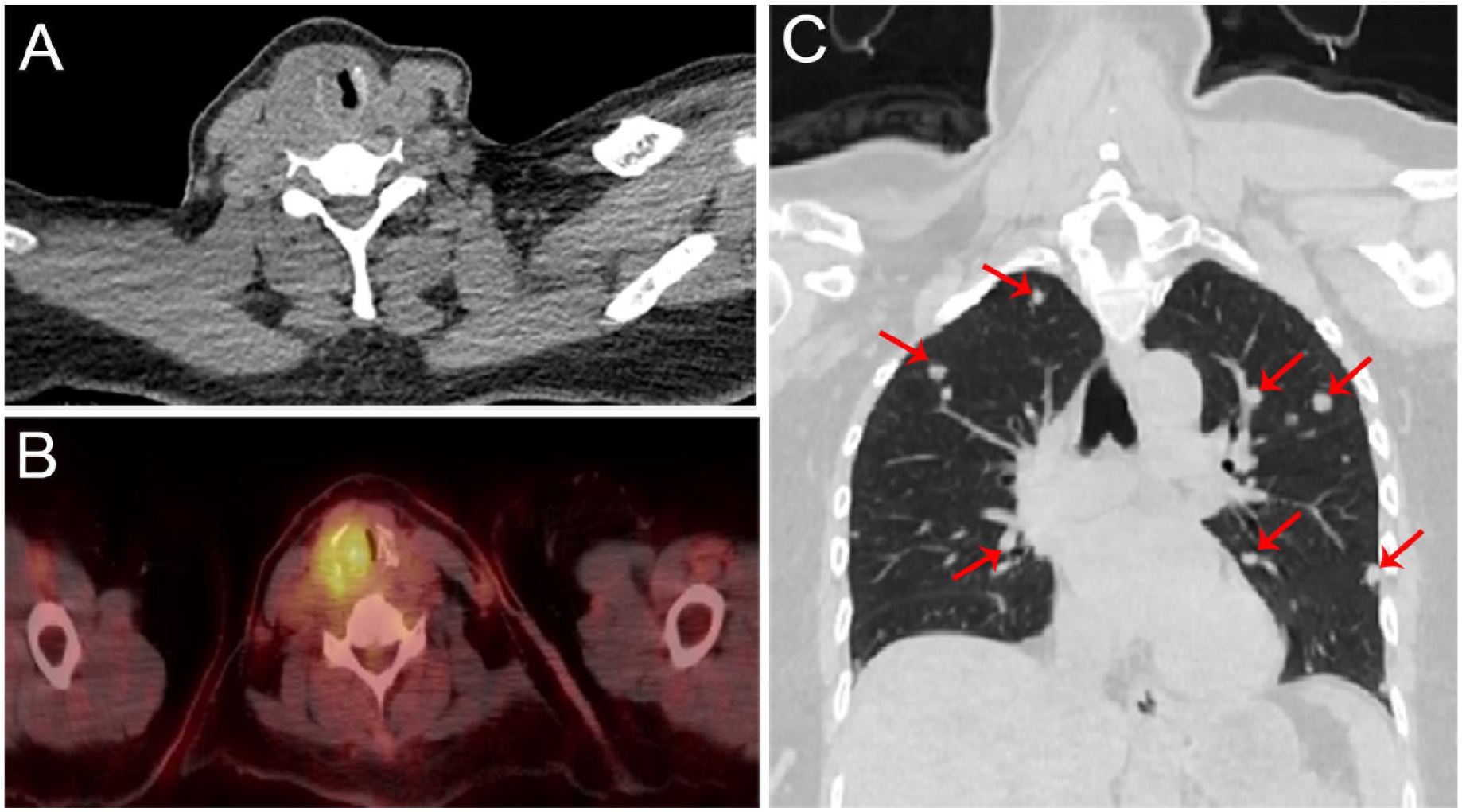
Axial CT (A) and axial fused fluorodeoxyglucose PET/CT (B) images show diffuse fluorodeoxyglucose uptake by the thickened trachea with a maximum standardized uptake value of 12. Axial thorax CT (C) shows multiple pulmonary nodules consistent with metastasis (arrows). PET, positron emission tomography; CT, computed tomography
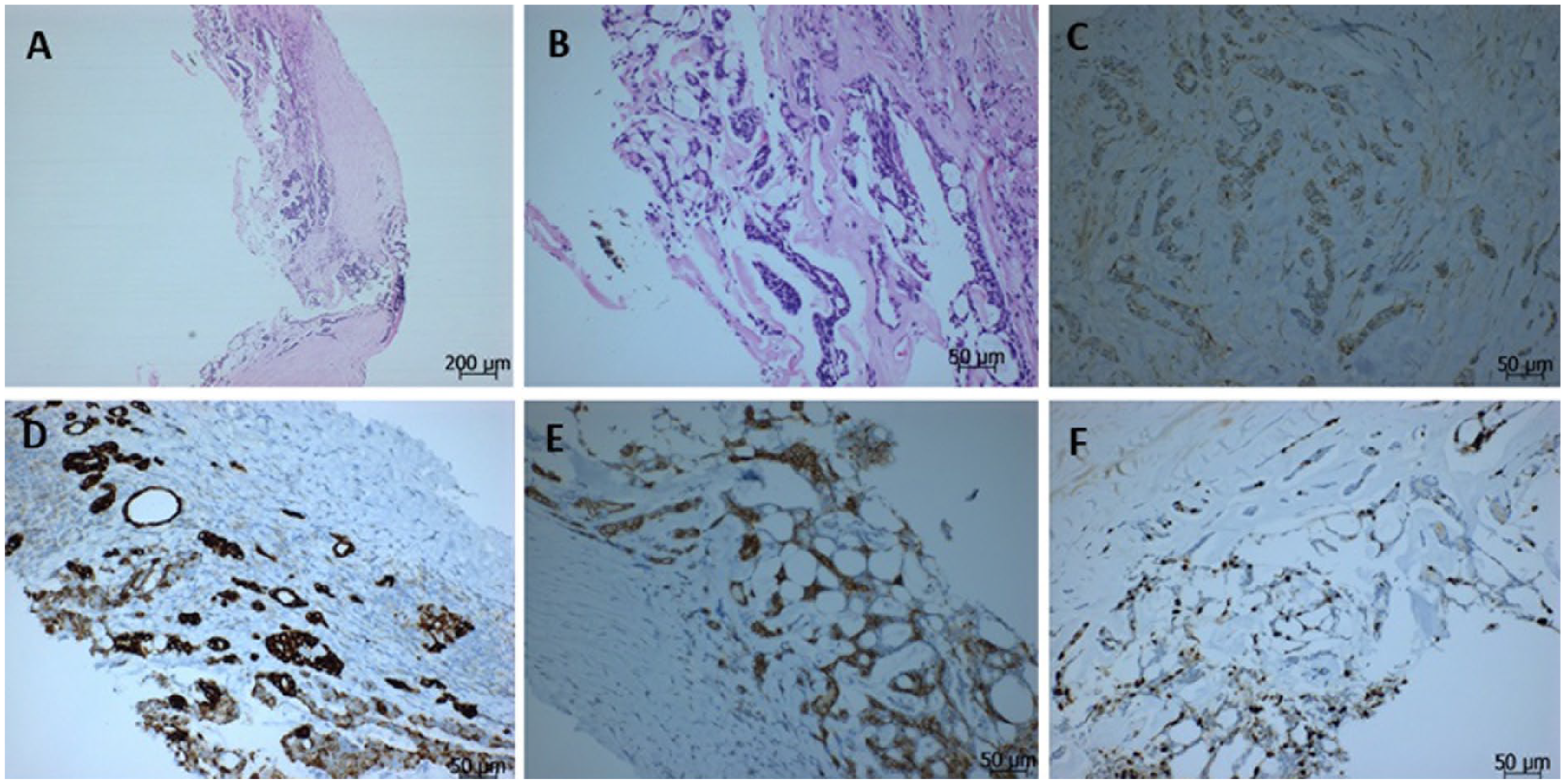
Adenoid cystic carcinoma consisting of ductal and myoepithelial cells distributed in fibrous stroma, occasionally containing cribriform pattern (hematoxylin-eosin) (A, B). Myoepithelial cells showing positive reactivity with S-100 (C). CK-7 positivity in ductal component (D). CD-117 positivity (C-E). Nuclear positivity with Ki-67 (D-F).
Footnotes
Author Contributions
M.Y. and C.A. contributed to the design of the case. M.Y. and S.Ö. contributed to the creation of images. M.Y. wrote the paper.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases.
Informed Consent
The authors declare that informed written consent was obtained from the patient for this case.