
Abstract
Introduction
Idiopathic sudden sensorineural hearing loss (ISSNHL) refers to a rapid onset of hearing decrement exceeding 30 dB across 3 contiguous frequencies within a span of less than 3 days. 1 While the cause of ISSNHL can be idiopathic, it may also stem from viral infections, vascular issues, or immunologic disorders. The challenge in pinpointing the precise etiology of this hearing loss has resulted in a lack of consensus regarding the management of ISSNHL. A significant proportion of SSNHL cases are idiopathic, and if not promptly diagnosed and treated, can lead to chronic hearing impairment, tinnitus, and diminished quality of life. Regarding treatment strategies, some researchers have advocated for the use of dexamethasone, administered either intravenously or via tympanic membrane injection.2,3 While there is no standardized treatment protocol, the consensus is that glucocorticoids form the cornerstone of pharmacological management. 4 Multiple studies have highlighted the safety and efficacy of intratympanic injection as a therapeutic modality. 5 Findings indicate that brief courses of intratympanic steroid therapy demonstrate a pronounced therapeutic benefit for moderate ISSNHL, surpassing the natural progression of the condition and the effects of placebo. Additionally, this method allows for a higher concentration of steroids to reach the affected ear, minimizing systemic adverse effects. 6 It is recommended that intratympanic steroid therapy be initiated within 2 to 6 weeks of the onset of ISSNHL, with a strong emphasis on the timing of intervention. 7
In this study, patients with idiopathic sudden deafness who failed to respond to conventional medical therapy within 1 week were selected. These individuals underwent treatment with dexamethasone via intratympanic injection, utilizing either portable video otoscopy or conventional video otoscopy as guidance. The portable ear endoscope is a new type of wireless, portable, handheld video ear endoscope equipped with a high-definition display screen. By comparing the outcomes of these 2 different approaches, the study aimed to evaluate the efficacy and discern the advantages and disadvantages of portable video otoscopic tympanic injection.
Materials and Methods
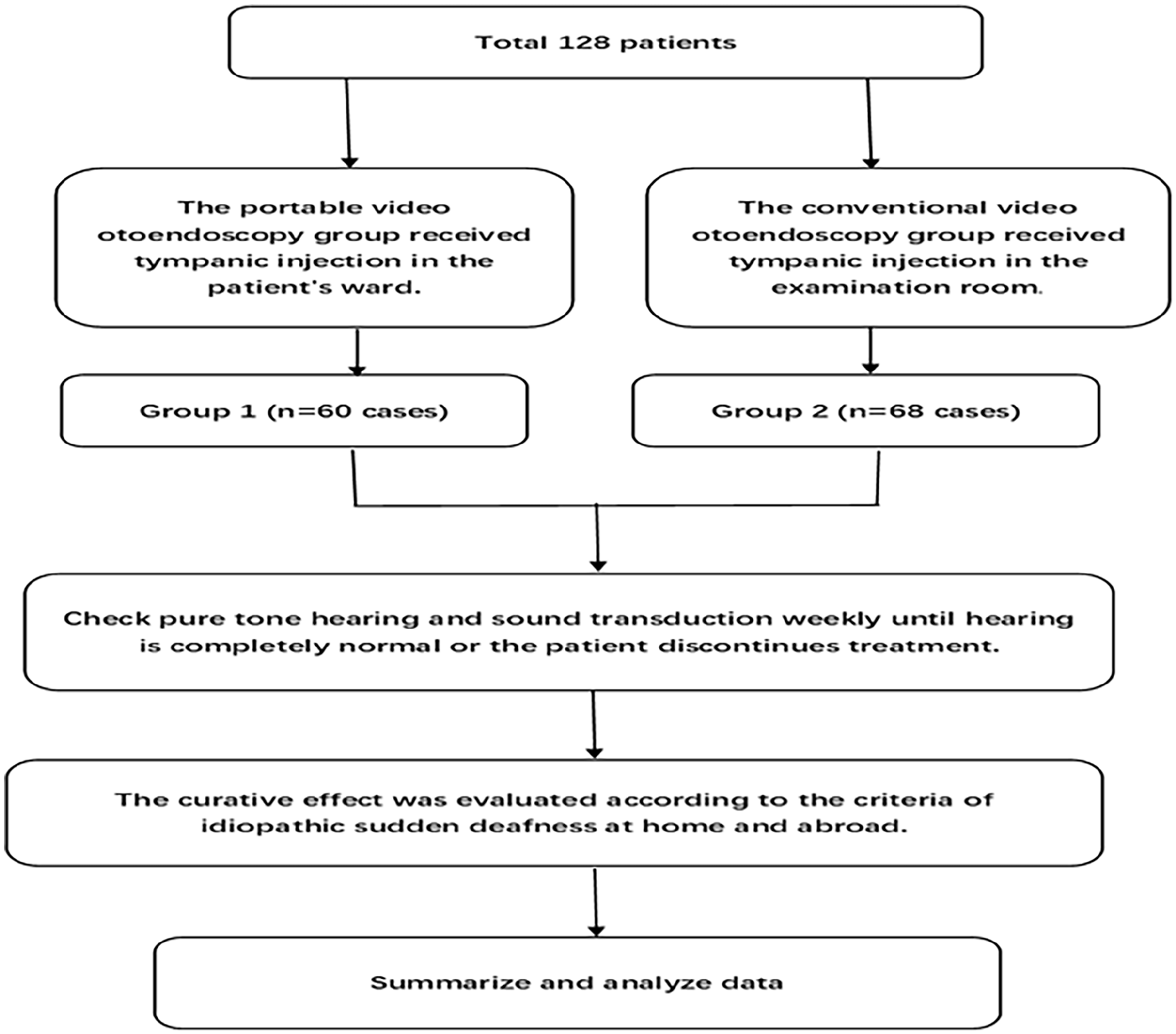
The research protocols were reviewed and approved by the institutional review board of our hospital, ensuring adherence to ethical guidelines and regulatory standards (Figure 1). This study was granted ethical clearance by the Ethics Committee of Hangzhou Normal University Affiliated Hospital.
Experiment methods.
Subjects
This investigation retrospectively analyzed the clinical data of patients admitted to our hospital for ISSNHL between January 2019 and June 2023. Eligible patients exhibited minimal hearing improvement following 1 week of standard treatment, with symptom onset ranging from 1 day to 20 days. The study population consisted of 54 males and 74 females, aged 20 to 77 years. Inclusion criteria for the study were (1) acute, unexplained hearing loss; (2) a decline of at least 20 dB in at least 2 contiguous audiometric frequencies within 72 hours; (3) uniform administration of a basic treatment regimen during hospitalization, which included Ginkgo Leaf Extract Injection (to enhance circulation), Mecobalamine injection (for neural nutrition), and Methylprednisolone sodium succinate intravenous infusion (80 mg daily for 3 days, followed by 40 mg daily for 3 days), with no significant hearing improvement observed after 1 week. Exclusion criteria encompassed: (1) Benign or malignant tumors affecting the external ear, middle ear, inner ear, or auditory nerve, or other clearly etiologized conditions causing hearing loss; (2) Comorbid neurological disorders or pregnancy; and (3) Conductive hearing loss exceeding 10 dB HL. Ultimately, 128 patients were enrolled, with 60 assigned to the portable video otoendoscopy group (Group 1) and 68 to the conventional video otoendoscopy group (Group 2).
Therapeutic Method
Upon the lack of significant auditory improvement following 1 week of conventional therapy, the therapeutic approach was modified to incorporate intratympanic dexamethasone injections, while concurrently continuing the previously administered therapeutic measures. Prior to the initiation of the intratympanic injections, patients underwent informed consent procedures, during which the potential benefits and risks of the procedure were thoroughly explained, and their written consent was obtained. The otoendoscopic equipment underwent standard disinfection protocols prior to each procedure. Intratympanic injections were administered at alternating intervals. Patients in Group 1 received the injections within the confines of their hospital ward utilizing Wireless Portable Handheld High-Definition Video Ear Endoscope (see Figure 2), while patients in Group 2 received the injections in a designated examination room utilizing an image monitoring system and otoendoscope (see Figure 3). Audiometric assessments, including pure tone audiometry and acoustic impedance testing, were conducted on a weekly basis until either the patient achieved normal hearing or elected to discontinue treatment.

Wireless portable handheld high-definition video ear endoscope.

Conventional video otoendoscopy.
Intratympanic steroid injection methods: (1) 70% alcohol was used to disinfect the external auditory canal of the affected ear, and the head was tilted to the opposite ear in the supine position. (2) Puncture the anterior superior tympanic membrane with a 1 mL syringe (0.5 × 38 mm needle) and inject dexamethasone solution to fill the posterior tympanic area (0.4-0.5 mL). (3) The patient was kept in an elevated head position for 20 to 30 minutes and instructed not to speak, swallow, or move. An alcohol cotton ball was inserted into the external auditory canal and removed the next day. At the time of discharge, all patients had intact tympanic membranes and no obvious earache, dizziness, and other posttympanic injection complications.
Description of Therapeutic Effect Evaluation Methods
Based on the World Health Organization (WHO) guidelines, 1 the pretreatment hearing levels of participants were categorized into the following groups:
(i) Mild Hearing Loss (Mild HL): Pure-tone average (PTA) ranging from 26 to 40 decibels hearing level (dB HL) 26 to 40 dB HL
(ii) Moderate Hearing Loss (Moderate HL): PTA ranging from 41 to 55 dB HL
(iii) Moderate to Severe Hearing Loss (Moderate to Severe HL): PTA ranging from 56 to 70 dB HL
(iv) Severe Hearing Loss (Severe HL): PTA ranging from 71 to 90 dB HL
(v) Profound Hearing Loss (Profound HL): PTA of 91 dB HL or higher
Additionally, the participants were also grouped according to the severity of their hearing loss:
(i) Mild to Moderate Hearing Loss: PTA ranging from 26 to 55 dB HL
(ii) Moderate to Severe Hearing Loss: PTA ranging from 56 to 90 dB HL
(iii) Extremely Severe Hearing Loss: PTA of 91 dB HL or higher
The therapeutic efficacy for ISSNHL was assessed using the following criteria 1 :
(1) Recovery: Normalization of hearing in the affected ear or restoration to the level of the healthy ear/level prior to the onset of the disease
(2) Marked Improvement: Average hearing improvement of greater than 30 dB HL in the affected ear
(3) Improvement: Average hearing improvement of 15 to 30 dB HL in the affected ear
(4) No Improvement: Average hearing improvement of less than 15 dB HL in the affected ear
Statistical Analysis
Data processing and statistical analysis were performed using SPSS 19.0 statistical software. Continuous variables were expressed as mean ± standard deviation (x ± s) and compared between groups using the independent-samples t-test. Categorical variables were compared using the chi-square test. A P-value of less than .05 was considered statistically significant.
Result
Comparison of Baseline Clinical Characteristics
A comparative analysis of the general clinical data between the 2 groups revealed no statistically significant differences. Specifically, the independent-samples t-test demonstrated no significant variations in age, disease duration, treatment duration, pretreatment hearing grade, and tympanic injection frequency between the portable video otoendoscopy group and the conventional video otoendoscopy group (Table 1). Similarly, the chi-square test indicated no significant differences in gender distribution, ear disease characteristics, hearing loss severity, and the presence of comorbidities such as hypertension, hyperlipidemia, diabetes, and coronary heart disease between the 2 groups (Table 1).
Comparison of the Demographics and Hearing Characteristics Between the 2 Groups.
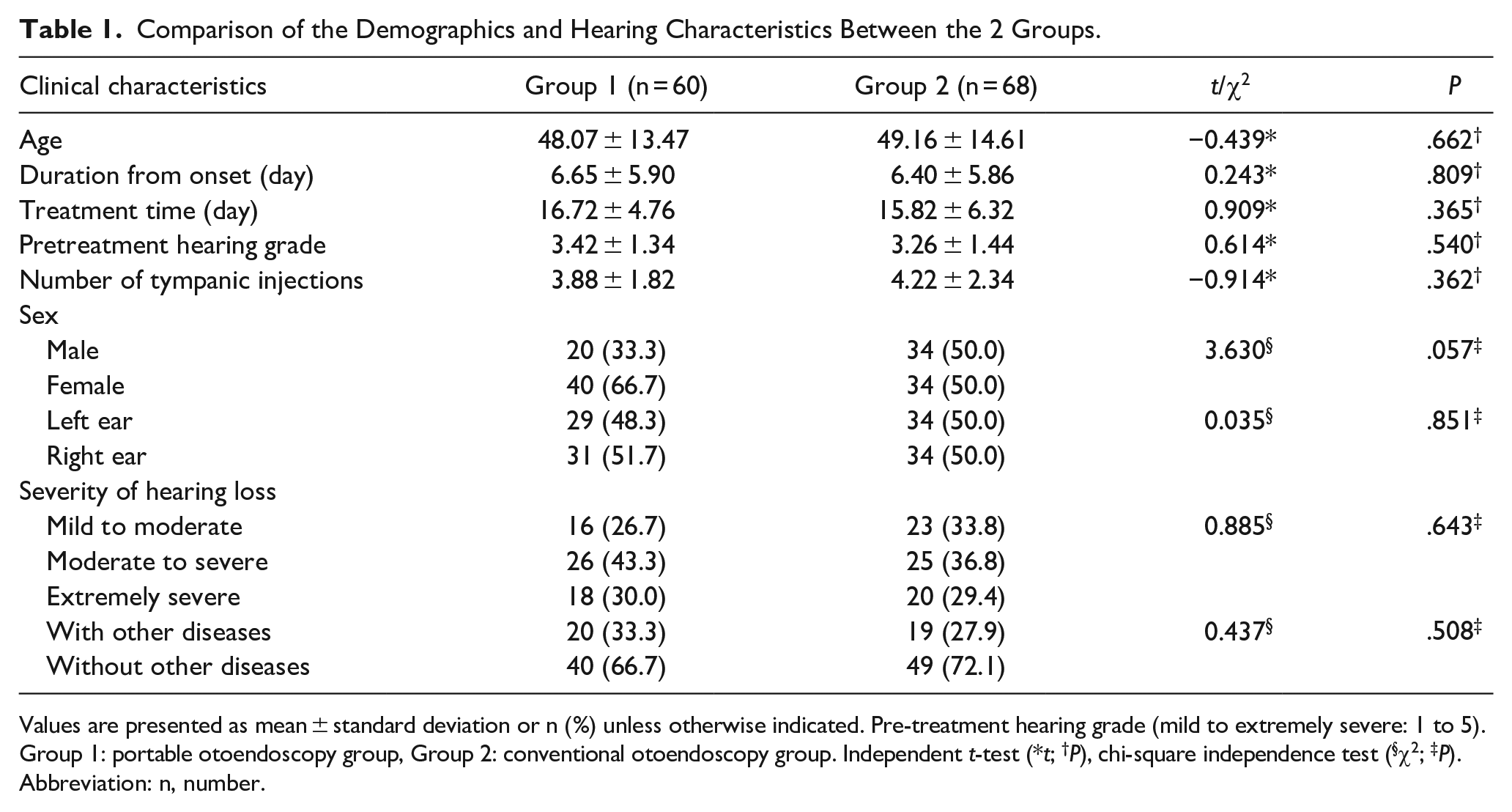
Values are presented as mean ± standard deviation or n (%) unless otherwise indicated. Pre-treatment hearing grade (mild to extremely severe: 1 to 5).
Group 1: portable otoendoscopy group, Group 2: conventional otoendoscopy group. Independent t-test (*t; †P), chi-square independence test (§χ2; ‡P).
Abbreviation: n, number.
Comparison of Overall Efficacy
A comparison of the total effective rate between the 2 groups revealed significant differences. Both portable video otoendoscopy and conventional video otoendoscopy demonstrated statistically significant improvements in hearing (t1 = 8.956, t2 = 6.299, P < .001) (see Figure 4). However, the portable video otoendoscopy group achieved a higher total effective rate (71.67%) compared to the conventional video otoendoscopy group (50.00%), with a significant difference observed (χ2 = 6.243, P = .012). This suggests that the portable video otoendoscopy technique may be associated with enhanced therapeutic efficacy for ISSNHL.
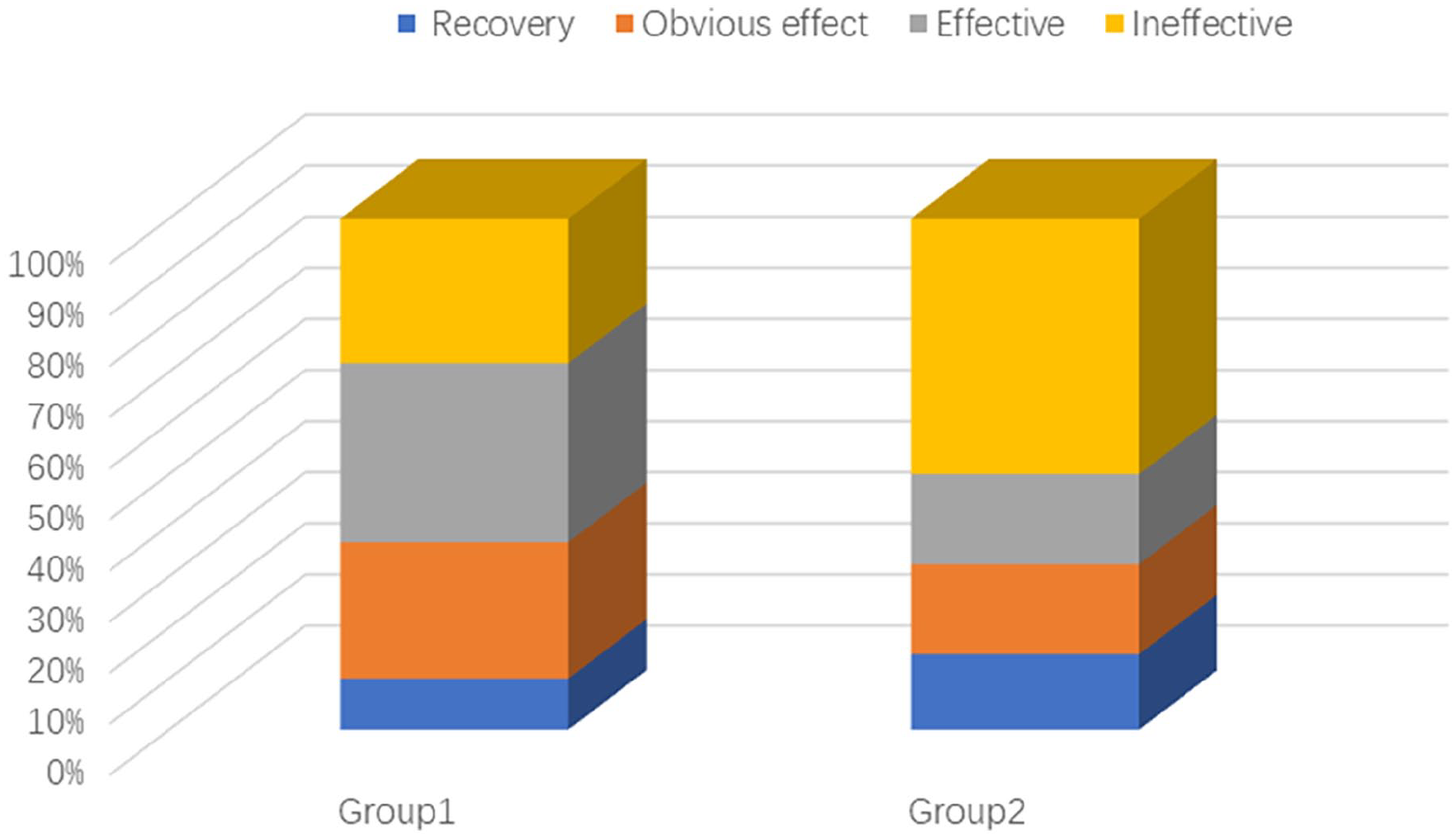
Comparison of efficacy between the 2 groups.
Efficacy Across Different Degrees of Hearing Loss
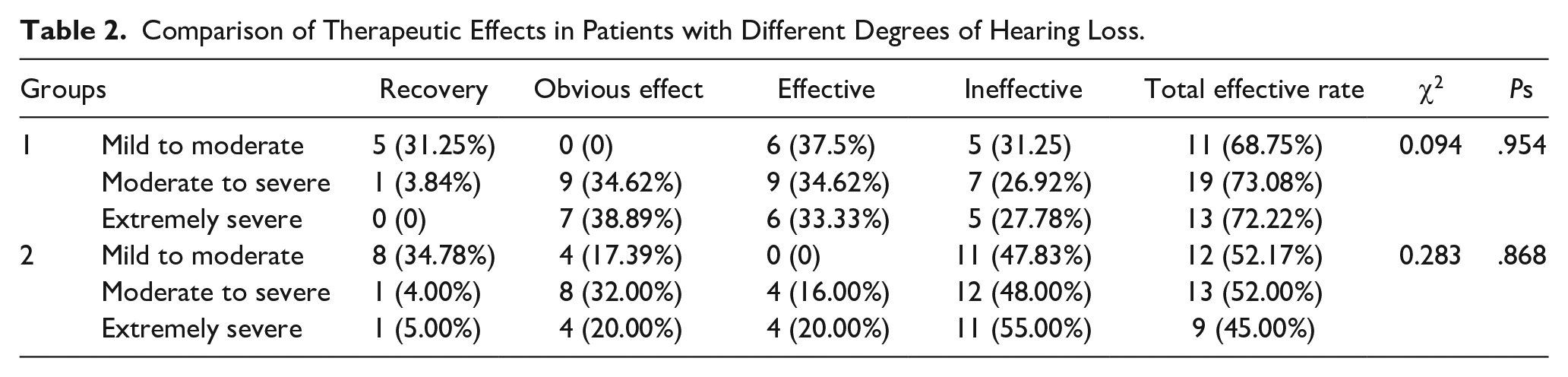
The study investigated the efficacy of intratympanic dexamethasone injection across various degrees of hearing loss within the 2 groups (Table 2). While both portable video otoendoscopy and conventional video otoendoscopy groups exhibited effectiveness for patients with mild to moderate, moderate to severe, and extremely severe hearing loss, there were no statistically significant differences in the total effective rates between the 2 groups within each hearing loss category. Specifically, the chi-square test results for mild to moderate deafness (χ2 = 1.072, P = .301), moderate to severe deafness (χ2 = 2.422, P = .120), and extremely severe deafness (χ2 = 2.880, P = .090) indicated no significant differences. This suggests that the choice of otoendoscopy technique does not impact the efficacy of intratympanic dexamethasone injection across different degrees of ISSNHL severity.
Comparison of Therapeutic Effects in Patients with Different Degrees of Hearing Loss.
Discussion
The timing is crucial for the treatment of ISSNHL. Initial therapy should be initiated within 2 weeks of symptom onset, while salvage therapy should be considered within 1 month of onset. 4 Optimal recovery is typically observed at least 2 weeks after the damage to inner ear hair cells. 8 Therefore, patients with ISSNHL should receive active treatment and the efficacy should be evaluated after at least 2 weeks of therapy.
In this context, we selected local tympanic injection of dexamethasone for patients with ISSNHL who failed to show significant improvement with conventional systemic therapy within the first week. Following transtympanic dexamethasone administration, hearing improvement was observed in both groups. When comparing patients with varying degrees of hearing loss within and between the groups, no significant difference in treatment response rate was observed. This suggests that the initial severity of hearing loss is not predictive of treatment response. Thus, intra-tympanic dexamethasone therapy is effective for patients with different degrees of hearing loss. The mechanisms of action of corticosteroids in the treatment of ISSNHL are well-established and include (1) Anti-inflammatory effects: Reduction of inflammation within the inner ear. (2) Ischemic protection: Protection against ischemic damage. (3) Increased cochlear blood flow: Improvement in blood flow to the cochlea. (4) Regulation of endocochlear potentials and protein synthesis: Modulation of these physiological processes within the inner ear. Corticosteroids not only directly affect the function of outer hair cells but also help to reduce the size of the degenerated area of the stria vascularis. Moreover, intra-tympanic injection is an effective method for delivering prednisolone to the inner ear. 9 Compared to systemic corticosteroids, local injection through the tympanic cavity allows for higher intra-tympanic drug concentrations. 10 Therefore, intra-tympanic injection of dexamethasone not only increases the concentration of drugs in the inner ear and improves the effective rate but also significantly reduces systemic side effects.
Conventional tympanic injections are typically performed in a clinical setting using an image monitoring system and a rigid otoscope, which is currently the most widely used video otoscope connected by an optical fiber. However, this method is restricted by the limited space and requires patients to lie flat for 20 to 30 minutes postinjection, during which time other patients awaiting the same treatment can only wait. If a patient before them experiences ear pain or dizziness, it may also induce anxiety and fear in the subsequent patient undergoing treatment. The portable otoscope features a flip-screen design, utilizing a pivot mechanism to allow the display to be flipped, enabling the physician to observe images at the optimal angle with the convenience of camera and recording functions. After use, the lens and the main display screen can be detached for easy storage and portability. It facilitates bedside tympanic injection procedures, free from spatial limitations, and saves other patients 20 to 30 minutes of waiting time. Similarly, it also allows busy medical professionals to save time in treating all patients.
This study investigated the efficacy of tympanic dexamethasone injection for ISSNHL by comparing 2 different ear endoscopic-guided techniques. The results revealed a significant advantage for portable video ear endoscopy over conventional video ear endoscopy, warranting further exploration of the underlying reasons. Potential Factors Contributing to the Superiority of Portable Video Ear Endoscopy: (1) Psychological Factors: Minimizing Environmental Adaptation: Patients treated using portable video ear endoscopy can receive therapy from the comfort of their beds, eliminating the need to adjust to a new treatment environment. This reduces anxiety and fear, potentially improving treatment adherence. Previous research has highlighted the negative impact of poor adherence on treatment outcomes. 11 Reducing Mood Fluctuations: The familiarity and comfort of the in-room setting mitigate mood swings, decreasing the body’s stress response and its subsequent negative influence on neurohumoral regulation. This helps maintain optimal microcirculation in the inner ear, essential for proper blood supply and metabolic function. 12 Promoting Relaxation and Improved Microcirculation: The calming environment fosters relaxation, enhancing inner ear microcirculation and immune function. This, in turn, facilitates hearing recovery. 13 (2) Time Factor: Extended Drug Exposure: Intratympanic dexamethasone bypasses the blood-brain and labyrinth barriers, maximizing drug concentration within the perilymphatic fluid and cochlear blood flow. 10 Fu’s research suggests that the duration of drug exposure after tympanic injection directly correlates with treatment efficacy. 13 Optimized Dexamethasone Penetration: Patients in the portable video ear endoscopy group maintain a lying position for an extended period following treatment. This prolonged recumbency allows more time for dexamethasone to permeate the round window membrane and reach the inner ear, potentially enhancing treatment efficacy.
Conclusions
The study demonstrates that the use of portable video ear endoscopic tympanic injection for treating ISSNHL offers several advantages: (1) It is not constrained by location, timing, or frequency, making it convenient for operation, transportation, and facilitating ward rounds, teaching, and consultation. (2) The rotating display provides a clear and easily observable view without the need for expensive equipment such as fiber optics and dedicated displays. (3) The ability to capture photos and videos facilitates data storage and review, and the ease of replacing the tube makes it particularly suitable for medical units with a high volume of patients and frequent endoscope usage. In this study, no significant complications were observed before or after treatment, except for pain and mild dizziness in some patients who underwent the injection. However, the study has limitations. Previous research has suggested a potential association between ISSNHL and labyrinthorrhagia in patients unresponsive to tympanic injection of Dexamethasone. 14 Although the incidence of this condition is low, the retrospective nature of the study precluded further investigation. Additionally, as a single-center retrospective study, further research is needed to establish the treatment’s efficacy, identify optimal therapeutic tools, and determine the ideal patient population that could benefit from this approach.
Footnotes
Author Contributions
The parts that the authors have played in the article are as following: Conceptualization: R.T., J.D., and J.J. Data curation: R.T. and J.D. Formal analysis: R.T. Investigation: R.T. and J.D. Methodology: J.D. and J.J. Project administration: J.D. and J.J. Supervision: J.D. and J.J. Writing – original draft: R.T. Writing – review & editing: J.D. and J.J.
Availability of Data and Materials
The original data can be obtained from the corresponding author by email upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Health Science and Technology Project of Hangzhou city (A20220403).
Ethics Approval
This study was approved by the Ethics Committee of Hangzhou Normal University Affiliated Hospital.