
Abstract
Introduction
Stroke, with its significant mortality and disability rates, represents a substantial threat to public health. In China, nearly 2 million new cases of stroke are reported each year. 1 Tracheostomy serves as an essential intervention for ensuring airway patency and sustaining life in patients with stroke who are critically ill. Research has shown that the tracheostomy rate among patients with ischemic stroke is approximately 1.3%. 2 In contrast, in patients with hemorrhagic stroke, particularly those with severe conditions and Glasgow Coma Scale (GCS, a method for assessing the degree of coma of a patient by evaluating eye opening response, language response, and limb movement) scores below 8, the tracheostomy rate is significantly higher, ranging from 50% to 70%. 3
Although tracheotomy saved the patient’s life, it laid the groundwork for related complications in the subsequent recovery process. Complications of tracheostomy, such as airway collapse or narrowing, granulation tissue formation, and pulmonary infections, can significantly affect the quality of life, swallowing function, and vocal mechanisms in patients with stroke, thereby impeding their recovery process.4,5 The first Stroke Recovery and Rehabilitation Roundtable (SRRR) experts panel emphasized that the early subacute phase (7 days to 3 months post-stroke), a critical period for neurorepair, should be the focus for the rehabilitation of various system functions. 6 Research indicates that early decannulation positively influences the recovery of consciousness and overall prognosis in patients who have undergone tracheostomy.7,8 One study revealed that decannulation was achieved in 59.4% of stroke patients surviving the first 12 months after tracheostomy and was associated with better functional outcomes compared to patients without decannulation. 9 According to a systematic review and meta-analysis involving 1405 studies, decannulation occurred in 79% (95% CI 51%-93%) of survivors of patients undergoing tracheostomy after severe acute brain injury. 9 Therefore, finding the key factors for early decannulation is the primary goal of medical staff.
Previous related studies have listed some important factors affecting decannulation. A review of the literature identified several factors contributing to the failure of tracheostomy decannulation, including advanced age, neurological damage, moderate to severe anemia, impaired cough reflex, and swallowing dysfunction.10,11 Conversely, successful decannulation is associated with well-managed pulmonary infection, a robust cough reflex, and a short intubation duration. 12 Despite its importance as a tool for assessing aspiration risk in patients who have undergone tracheostomy, the modified Evan’s blue dye test (MEBDT) is infrequently used in domestic research.13,14 To address this gap, a retrospective study was conducted involving patients with stroke who underwent a tracheostomy at a tertiary grade A hospital between January 2020 and December 2023. The study analyzed the general demographics, airway conditions, nutritional status, and infection indicators of the patients to identify key factors influencing successful early subacute phase decannulation. The objective of these findings is to guide the development of an early rehabilitation program for patients with stroke undergoing tracheostomy, to enhance recovery outcomes by addressing the factors that influence decannulation.
Data and Methods
General Information
A retrospective analysis was conducted on patients with stroke who underwent tracheostomy at a tertiary grade A hospital between January 2020 and December 2023. The inclusion criteria were as follows: (1) patients diagnosed with stroke confirmed through brain computed tomography or magnetic resonance image, in accordance with the diagnostic criteria outlined in the “Chinese Guidelines for Diagnosis and Treatment of Acute Ischemic Stroke 2018” 15 and the “Chinese Guidelines for Diagnosis and Treatment of Acute Intracerebral Hemorrhage (2019)” 16 ; (2) patients who underwent tracheostomy within 3 months of disease onset. Exclusion criteria were: (1) patients with incomplete medical records; (2) patients who were transferred to the ICU or died due to severe changes in their condition during hospitalization. A total of 219 patients met these criteria and were included in the study.
Investigation Methods
Clinically relevant data was collected through the review of medical records, rehabilitation assessments, and laboratory test results. Data included the following variables: gender, age, level of consciousness (as assessed during the first examination upon admission), GCS score (from the first assessment upon admission), tracheal polyp status (determined by the first fiberoptic bronchoscopy result after admission), use of a speaking valve, results of the MEBDT test 17 (conducted by a senior swallowing therapist during the first assessment after admission), coughing ability (as assessed upon admission), and nutritional risk (as determined by the first NRS2002 score upon admission). Laboratory data included the presence of multidrug-resistant bacteria in sputum cultures and white blood cell count, both derived from the first tests conducted after admission).
MEBDT involves administering a specific quantity of dyed food to the patient and subsequently observing the secretions coughed out or suctioned from the tracheostomy site to detect the presence of aspiration. 14 A positive result is indicated by the presence of dye in the secretions, whereas its absence indicates a negative result. In addition to its high sensitivity and specificity in determining whether there is aspiration in patients undergoing tracheotomy, this assessment method is simple, easy to implement, provides timely feedback, and poses no harm to the human body. Compared to the videofluoroscopic swallowing study, this method does not require patient transfer. Compared to fiberoptic endoscopic evaluation of swallowing, it reduces the risk of procedural injuries and minimizes patient discomfort. Given the current imbalance in medical resources, this method is more conducive to promotion.13,18,19
Cough ability is assessed using the Cough Strength Score, 20 which ranges from 0 to 5 and reflects the cough strength of the patient from weak to strong. This assessment tool is straightforward and is clinically recommended for its ease of use. 21
Decannulation criteria include: (1) Spontaneous breath, absence of the need for ventilator support; and (2) Stable vital signs. Normal body temperature; (3) Presence of a cough reflex, with the ability to autonomously expectorate sputum; (4) Tolerance for continuous tube occlusion for more than 48 hours without signs of respiratory distress, and monitored oxygen saturation at 95% or higher; (5) Chest imaging examination reveals no newly emerged or progressive infiltrative, consolidative, or ground-glass opacities; (6) Informed consent from family members.
Decannulation process: When the aforementioned conditions are met, the critical care team will initiate the extubation process. The critical care team consists of 3 specialist physicians, 4 rehabilitation therapists, and 3 senior neurology nurses. During each decannulation, at least 2 physicians, 1 rehabilitation therapist, and 1 specialist nurse are present. Throughout the entire extubation process, we provide vital sign monitoring for the patient. Prior to extubation, 2 physicians will conduct another auscultation of the patient’s lungs, with specialist nurses assisting in clearing the airway. Following decannulation, specialized nurses assist physicians in wound care. Ultimately, physicians, rehabilitation therapists, and specialized nurses will readjust the rehabilitation plan and advise on relevant precautions.
Successful decannulation is defined as the patient exhibiting no significant respiratory distress, being capable of independently coughing out sputum or having it removed via electric suction, and not requiring re-intubation for respiratory assistance, all within 7 days after the tracheostomy tube is removed. 12
Statistical Analysis
Statistical analysis was conducted using IBM SPSS 20.0 software. Quantitative data with a normal distribution were expressed as mean ± standard deviation, whereas data that did not follow a normal distribution were expressed as median and quartiles. Inter-group comparisons for continuous data were conducted using independent sample t-tests or non-parametric tests as appropriate. Categorical and ordinal data were presented as frequencies and percentages, with inter-group comparisons performed using chi-square tests or non-parametric tests. Factors showing statistically significant differences in inter-group comparisons were included in the logistic regression analysis to identify independent predictors of successful decannulation. The predictive ability of these factors was assessed by calculating the area under curve (AUC) in receiver operating characteristic (ROC) curve analysis. All statistical tests were conducted with a significance level set at P < .05.
Results
Comparison of Clinical Data and Univariate Analysis Between Two Groups
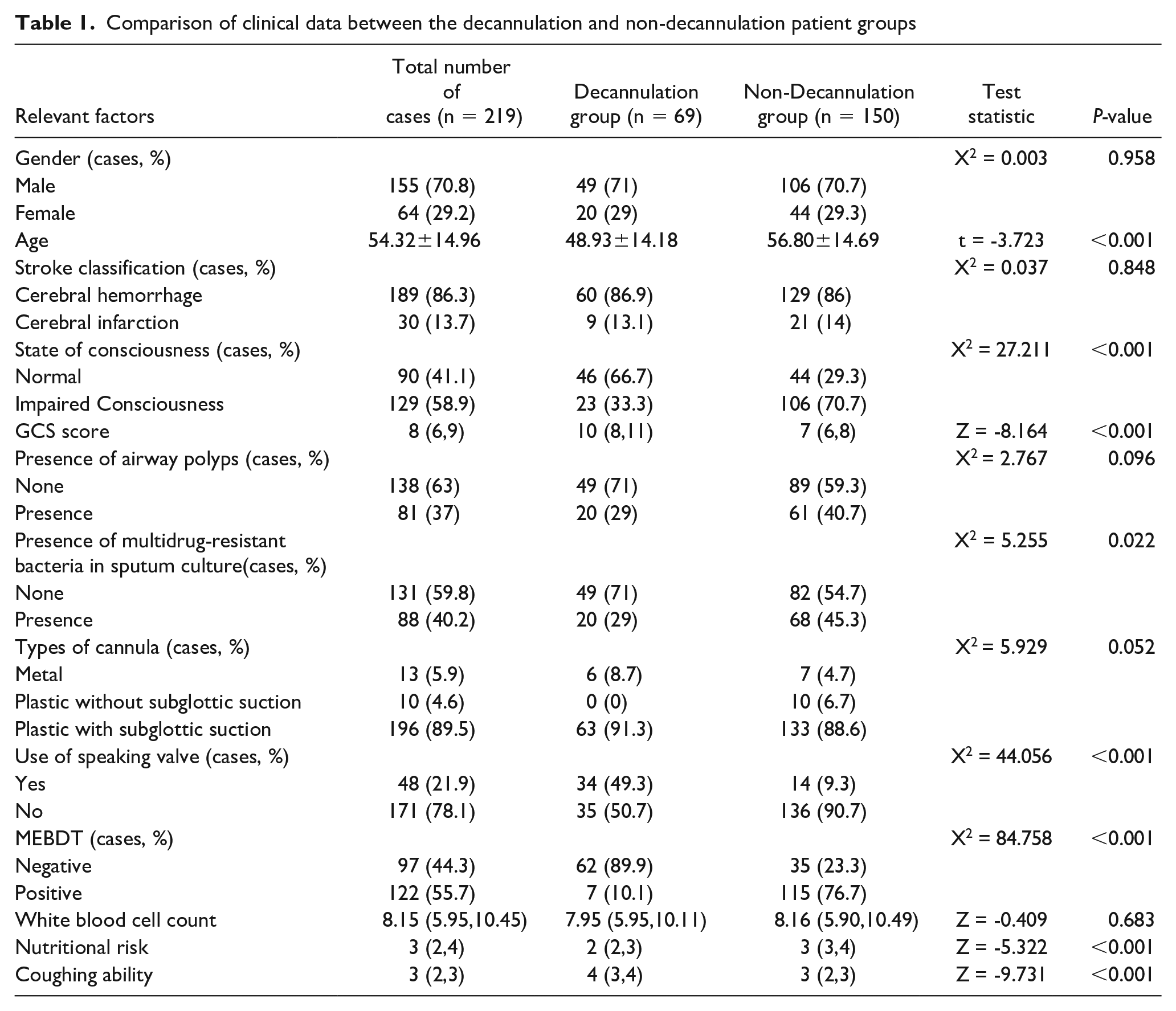
A total of 219 patients who underwent tracheostomy for stroke were included in this study. Of these, 69 patients had their tracheostomy tubes removed within 3 months, constituting the decannulation group. The remaining 150 patients, who did not have their tubes removed within 3 months, comprised the non-decannulation group. This group included 1 patient who required re-intubation within 48 hours after decannulation due to a change in condition. The analysis revealed no significant differences (P > .05) between the 2 groups in terms of gender, stroke subtype, presence of airway polyps, type of tracheostomy tube, or white blood cell count. Significant differences (P < .05) were observed in age, level of consciousness, GCS score, presence of multidrug-resistant bacteria in sputum, use of a speaking valve, and results of the MEBDT (see Table 1). Among 69 patients, 2 had a history of viral encephalitis, 1 had a history of Guillain-Barre syndrome, 19 were diagnosed with hypertension, and 5 were diagnosed with diabetes.
Comparison of clinical data between the decannulation and non-decannulation patient groups
Multifactorial Logistic Regression Analysis
Variables with statistically significant differences identified in the univariate analysis were assigned values and incorporated into the multifactorial logistic regression model, with successful decannulation as the dependent variable. The analysis revealed that a positive dye test (P = .012, OR = 6.243, 95% CI = 1.500-25.989) was an independent risk factor for decannulation in patients with stroke undergoing tracheostomy. Conversely, high GCS scores (P = .001, OR = 0.380, 95% CI = 0.212-0.680) and strong cough ability (P < .001, OR = 0.053, 95% CI = 0.018-0.159) were identified as protective factors for successful decannulation. The detailed results are presented in Tables 2 and 3.
Overview of Independent Variables Assigned in the Study.
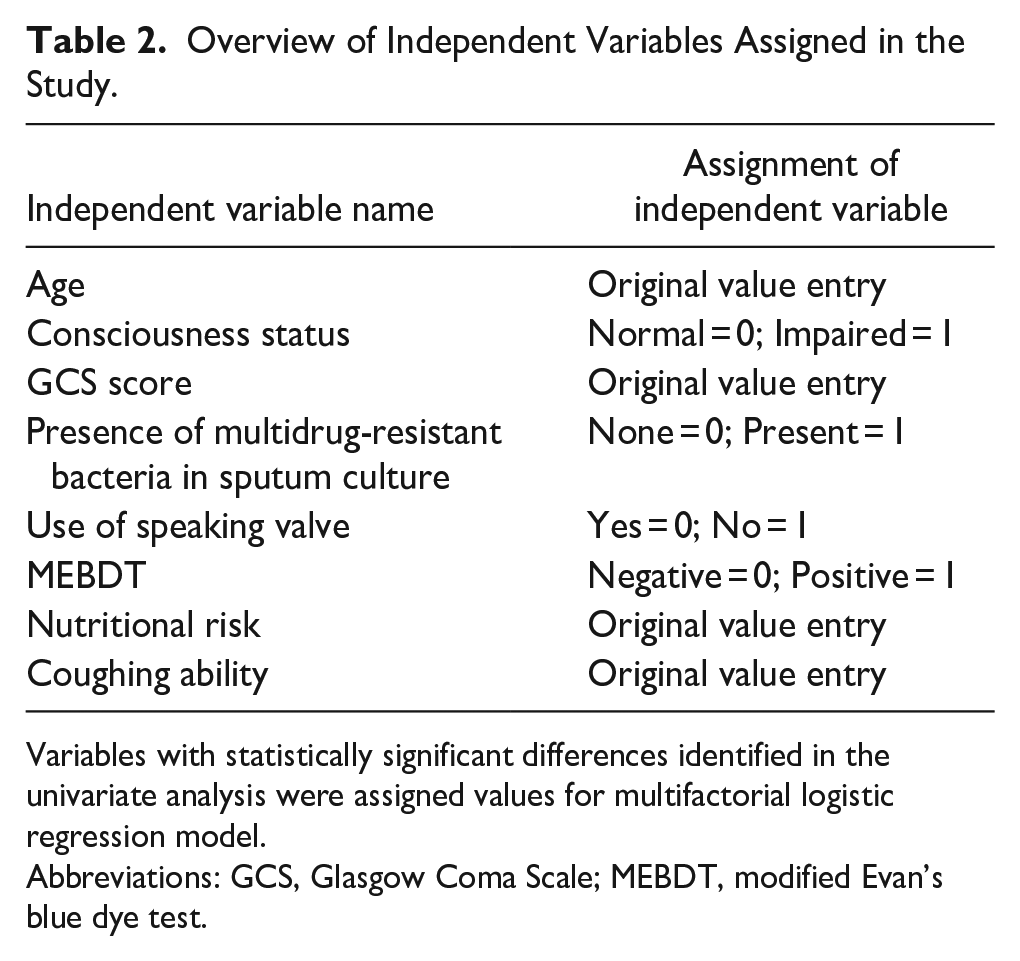
Variables with statistically significant differences identified in the univariate analysis were assigned values for multifactorial logistic regression model.
Abbreviations: GCS, Glasgow Coma Scale; MEBDT, modified Evan’s blue dye test.
Results of Multivariate Logistic Regression Analysis.
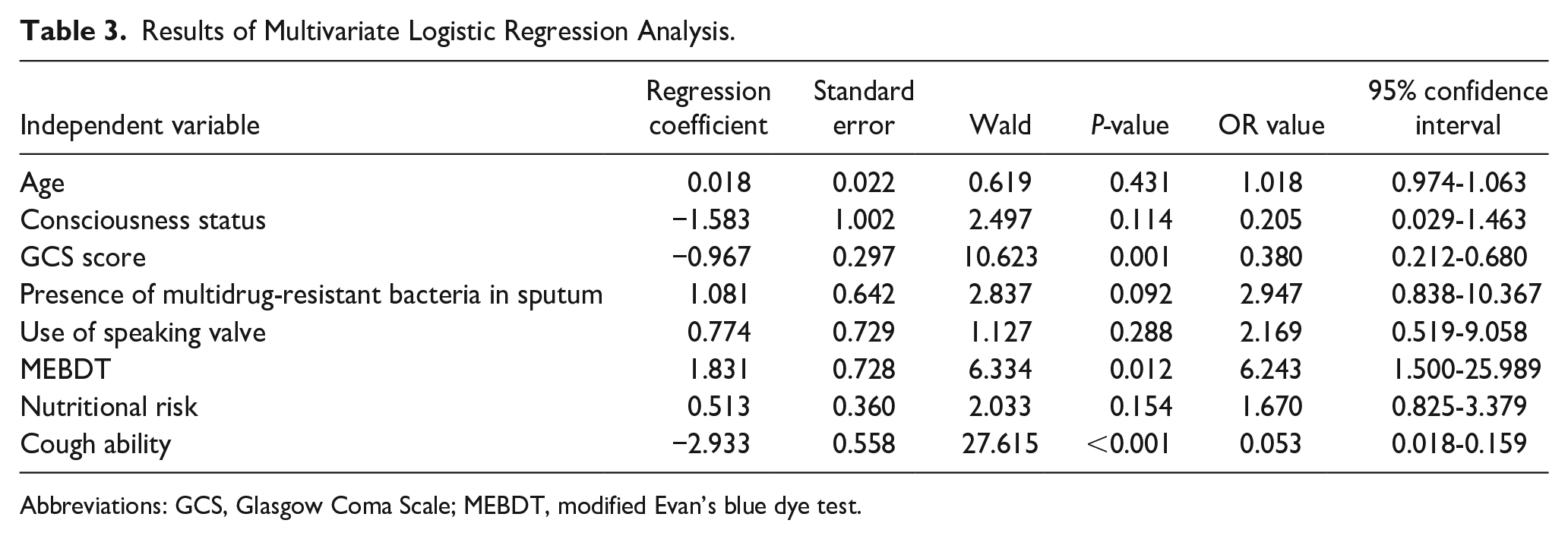
Abbreviations: GCS, Glasgow Coma Scale; MEBDT, modified Evan’s blue dye test.
Prediction of GCS Score, Dye Test Results, and Cough Ability for Successful Decannulation at Tracheotomy
The ROC curve analysis demonstrated that the AUC for predicting successful decannulation after tracheostomy was 0.848 for the GCS score, 0.843 for the MEBDT results, and 0.885 for cough ability, indicating good predictive performance for each individual factor. When combined, the AUC for these 3 factors was 0.975, reflecting an excellent predictive capability. The maximum Youden’s index for the combined model was 0.829, with a cut-off value of 0.19, sensitivity of 95.6%, and specificity of 87.3%. The individual AUCs were lower than the combined AUC, underscoring the superior predictive performance of the combined model (see Table 4 and Figure 1).
Multifactorial Receiver Operating Characteristic Curve Results for Predicting Successful Decannulation.
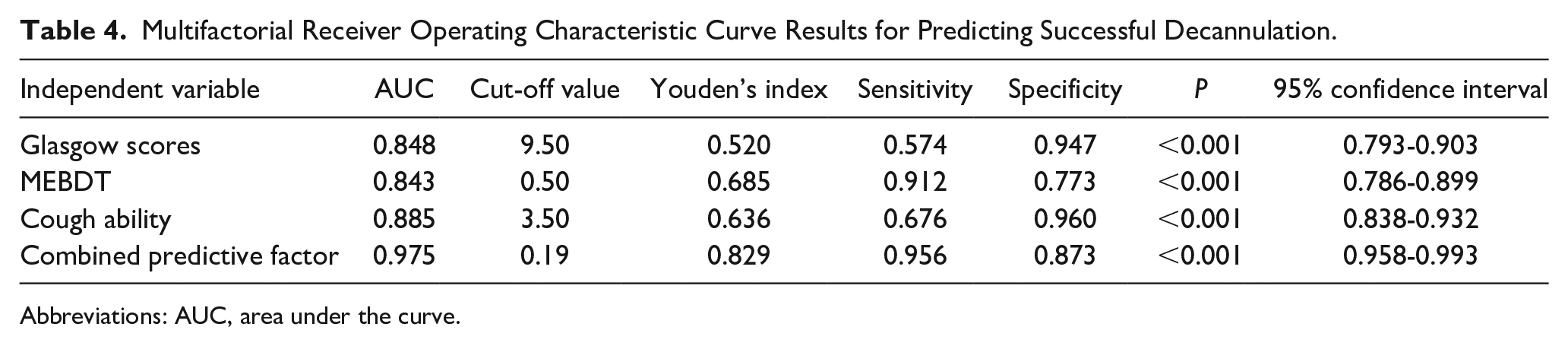
Abbreviations: AUC, area under the curve.
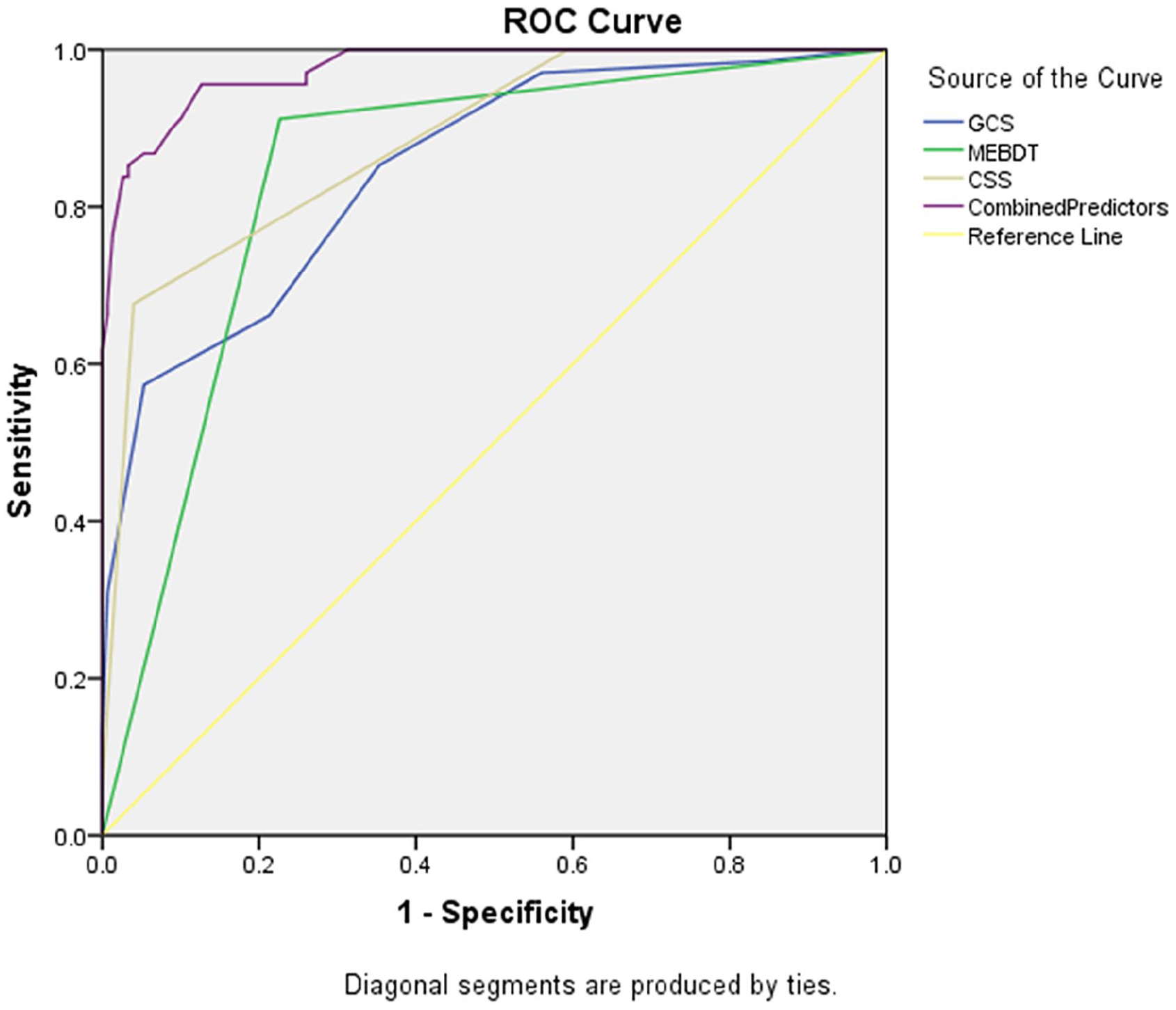
ROC curves. The ROC curve analysis demonstrated that the AUC for predicting successful decannulation after tracheostomy was 0.848 for the GCS score, 0.843 for the MEBDT results, 0.885 for cough ability, and 0.975 for the combination. ROC, receiver operating characteristic; AUC, area under the curve; GCS, Glasgow Coma Scale; MEBDT, modified Evan’s blue dye test.
Discussion
Tracheostomy Decannulation Status in Early Subacute Phase for Patients with Stroke
In this study, among the 219 patients diagnosed with stroke, 69 cases achieved successful decannulation within 3 months post-tracheostomy, resulting in a decannulation rate of 31.5%. This rate is notably lower compared to that reported by Lu et al, 12 but slightly higher than the decannulation rates observed by Du et al. 11 In one study reported by Zhang, 22 patients diagnosed with ischemic stroke within 1 month received a tracheostomy, the decannulation rates were lower. The variations in decannulation rates may be attributed to differences in the timing of stroke onset and the types of strokes across these studies. The lack of standardized rating scales or authoritative guidelines for pre-decannulation assessment and procedures in China indicates that the timing and success rates of decannulation are influenced by clinical experience and departmental proficiency. It is recommended that medical professionals address regional limitations by enhancing communication and knowledge sharing through participation in high-level specialty forums and advanced training at leading hospitals. Such efforts may help identify opportunities for earlier and safer decannulation for patients who have undergone tracheostomy and advanced neurorehabilitation practices.
The GCS Score, MEBDT, and Cough Ability are Independent Factors Influencing Tracheostomy Decannulation in the Early Subacute Phase of Stroke
The study results demonstrated that the GCS scores were significantly higher in the decannulation group compared to the non-decannulation group (P < .001). Multivariate regression analysis further indicated that a high GCS score (OR = 0.380, 95% CI = 0.212-0.680) served as a protective factor for tracheostomy decannulation in patients with stroke. Among the 69 patients who were successfully decannulated, all had GCS scores of ≥6, with approximately 84% having scores of ≥8. Previous studies have reported inconsistent results regarding the impact of GCS scores on decannulation outcomes in patients undergoing tracheostomy. These variations may be due to differences in sample sizes, disease types, and onset times across studies.23-26 To enhance the accuracy of findings, future research should consider expanding the sample size or conducting multicenter studies across diverse disease conditions.
In this study, a positive MEBDT result (OR = 6.243, 95% CI = 1.500-25.989) was identified as an independent risk factor for decannulation during the early subacute phase of stroke in patients undergoing tracheostomy. Due to its simplicity and suitability for bedside application, MEBDT is commonly used in clinical practice as a screening tool for aspiration in patients undergoing tracheostomy. Previous research has indicated that the efficacy of MEBDT in detecting aspiration is comparable to that of swallowing fluoroscopy, 13 and MEBDT results are recommended as one of the most reliable predictors of successful decannulation in patients undergoing tracheostomy.8,27 Therefore, it is advisable to perform standardized MEBDT as early as possible for patients undergoing tracheostomy to assess aspiration risk, thereby providing a basis for safe early decannulation.
The cough reflex, recognized as a fundamental indicator for decannulation, has been widely acknowledged and applied in clinical practice.11,12 This study identified good coughing ability (OR = 0.053, 95% CI = 0.018-0.159) as a protective factor for early decannulation in patients with stroke undergoing tracheostomy, which is consistent with the findings reported by Li et al. 28 The criteria for cough scoring are straightforward and easily applicable in clinical settings. Moreover, assessing cough ability has demonstrated significant predictive value for the risk of re-intubation. 29 Therefore, it is advisable for medical professionals to establish specialized pulmonary rehabilitation teams to assess the cough ability of patients who have undergone tracheostomy promptly. For patients with impaired cough reflexes, an appropriate pulmonary rehabilitation program should be developed and implemented to support early decannulation in patients with stroke.
Age and Nutritional Risk were Excluded from the Regression Analysis
In this study, age was a related factor for early extubation of stroke patients with tracheotomy, but it was not an independent factor. This result was similar to that of Yang et al, 30 but other studies have also shown that old age is an independent risk factor for inability to extubation.11,31,32 This may be related to the fact that age was not segmented in detail in this study or the sample size was small.
Studies have shown that nutritional status is an important factor affecting the success or failure of extubation in patients with tracheotomy.31,33 Previous studies used specific laboratory indicators to represent the nutritional status of patients, such as hemoglobin and serum albumin. Although the nutrition assessment scale used in this study can represent the overall nutritional risk of patients. Therefore, there might be a difference.
Limitation
The retrospective study design employed in this research encompassed a substantial time span for case collection, yet solely relied on data from a single hospital, thus presenting certain shortcomings and limitations. Additionally, due to the prolonged illness, repeated hospitalizations, and turnover issues encountered by these patients, they pose significant challenges for follow-up. In the future, considerations could be given to expanding the sample size, pursuing multicenter collaboration, conducting prospective cohort studies, and delving deeper into relevant issues.
Conclusion
The results of this study indicate that the combined prediction of early decannulation using the GCS score, MEBDT, and cough ability offers a superior AUC compared to each factor individually. Although the specificity of the combined prediction (87.3%) is slightly lower than that of the GCS score (94.7%) and cough ability (96%), the Youden index for the combined model (0.829) exceeds that of each individual factor. Therefore, we recommend the combined application of these 3 measures in clinical practice. For stroke patients undergoing tracheotomy, GCS assessment, cough ability assessment, and MEBDT should be performed in the early stages of the disease, provided that there are no serious changes in the condition or related complications. Early detection of adverse factors for decannulation and intervention should be carried out to lay the foundation for early decannulation.
Footnotes
Acknowledgements
We would like to acknowledge the hard and dedicated work of all the staff who implemented the intervention and evaluation components of the study.
Author Contributions
Conception and design of the research: H.-M.Q., D.-Z.T. Acquisition of data: H.-M.Q., R.-Y.X. Analysis and interpretation of the data: X.-Y.H., Q.-Y.X. Statistical analysis: X.-Y.H., H.-M.Q. Writing of the manuscript: H.-M.Q., R.-Y.X. Critical revision of the manuscript for intellectual content: D.-Z.T., Q.-Y.X.
All authors read and approved the final draft.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Zhujiang Hospital of Southern Medical University (2024-KY-185-01). This study was conducted in accordance with the declaration of Helsinki. Due to the retrospective nature of the study, the requirement of patient consent for inclusion was waived by the Ethics Committee of Zhujiang Hospital of Southern Medical University. Patient personal privacy and data confidentiality have been upheld.
Consent for Publication
Not applicable.