
Abstract

Significance Statement
Extramedullary plasmacytoma (EMP) is a rare tumor of plasma cells that manifests outside the bone marrow. The gold standard for diagnosis is histopathologic examination. Radiotherapy represents an efficacious treatment option, given the tumor’s radiosensitivity. In a patient presenting with a laryngeal mass, EMP should be considered as a potential diagnosis in addition to the more common tumors observed in this area, although it is a rare occurrence.
A 69-year-old male patient was admitted to our center with a chief complaint of hoarseness, which had been increasing over the previous 6 months. The patient was a nonsmoker and abstained from alcohol, with no history of trauma. He had a history of coronary artery disease and was currently undergoing medical treatment for it. Physical examination revealed no palpable mass or lymphadenomegaly in the neck. A contrast-enhanced computed tomography (CT) scan of the neck revealed a 40 × 32 × 37 mm mass lesion at the supraglottic level, extending inferiorly to the vocal cord level. The lesion was relatively well-circumscribed and homogenously contrasted (Figure 1). There was no significant destruction of the cartilaginous structures. Subsequently, magnetic resonance imaging (MRI) was performed to facilitate a clear evaluation of the lesion borders. The results demonstrated the presence of a mass lesion within the vallecula at the supraglottic level, extending inferiorly along the left lateral and anterior wall of the larynx, and along the ariepiglottic fold on the left. This lesion was observed to focally narrow the supraglottic airway with marked diffusion restriction on diffusion-weighted images and dense heterogeneous contrast on postcontrast images (Figure 2). Laryngoscopic evaluation confirmed the lesion described on MRI and punch biopsy was taken from this area. Laryngeal biopsy revealed plasma cell infiltration with CD138, CD38, CD56 strongly positive, and CD19 negative. These cells were strongly positive with kappa and lambda negative. Protein electrophoresis showed no M spike and serum and urine immunofixation electrophoresis showed no monoclonality. Positron emission tomography- computed tomography (PET-CT) did not show any lesion in any location or bony structures. In the bone marrow biopsy, CD38 was 2% to 3%, CD138 was 3% to 4% positive, CD19, CD20, and CD56 were negative. With these findings, multiple myeloma was excluded and the patient was diagnosed as extramedullary plasmacytoma (EMP). After radiotherapy in the involved area, due to lesion persistence, combination treatment with bortezomib, cyclophosphamide, and dexamethasone was initiated. The patient has been monitored for approximately 20 months, during which time he has remained in remission and no new lesions have developed.
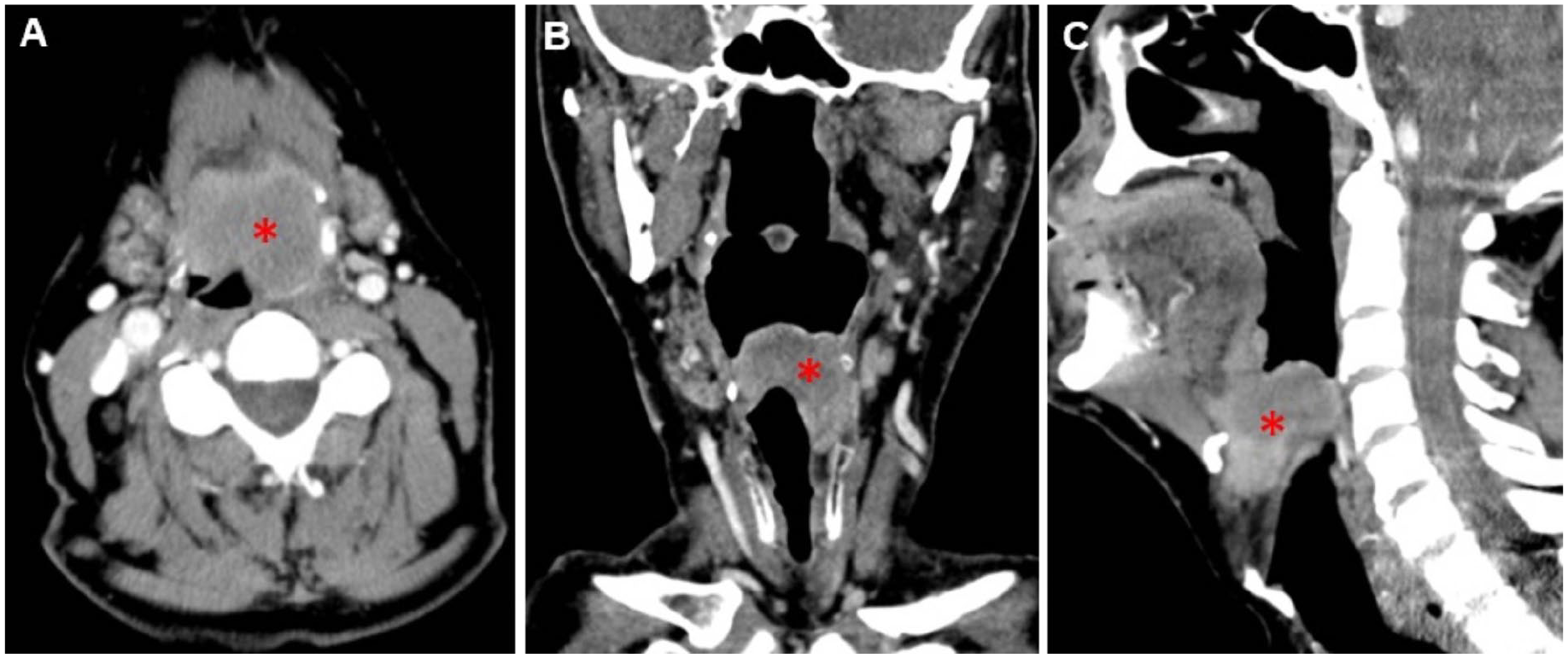
Axial (A), coronal (B), and sagittal (C) contrast-enhanced neck CT images showed a relatively well-circumscribed homogeneously enhancing hyperdense lesion (asterix) in the left supraglottic area. CT, computed tomography.
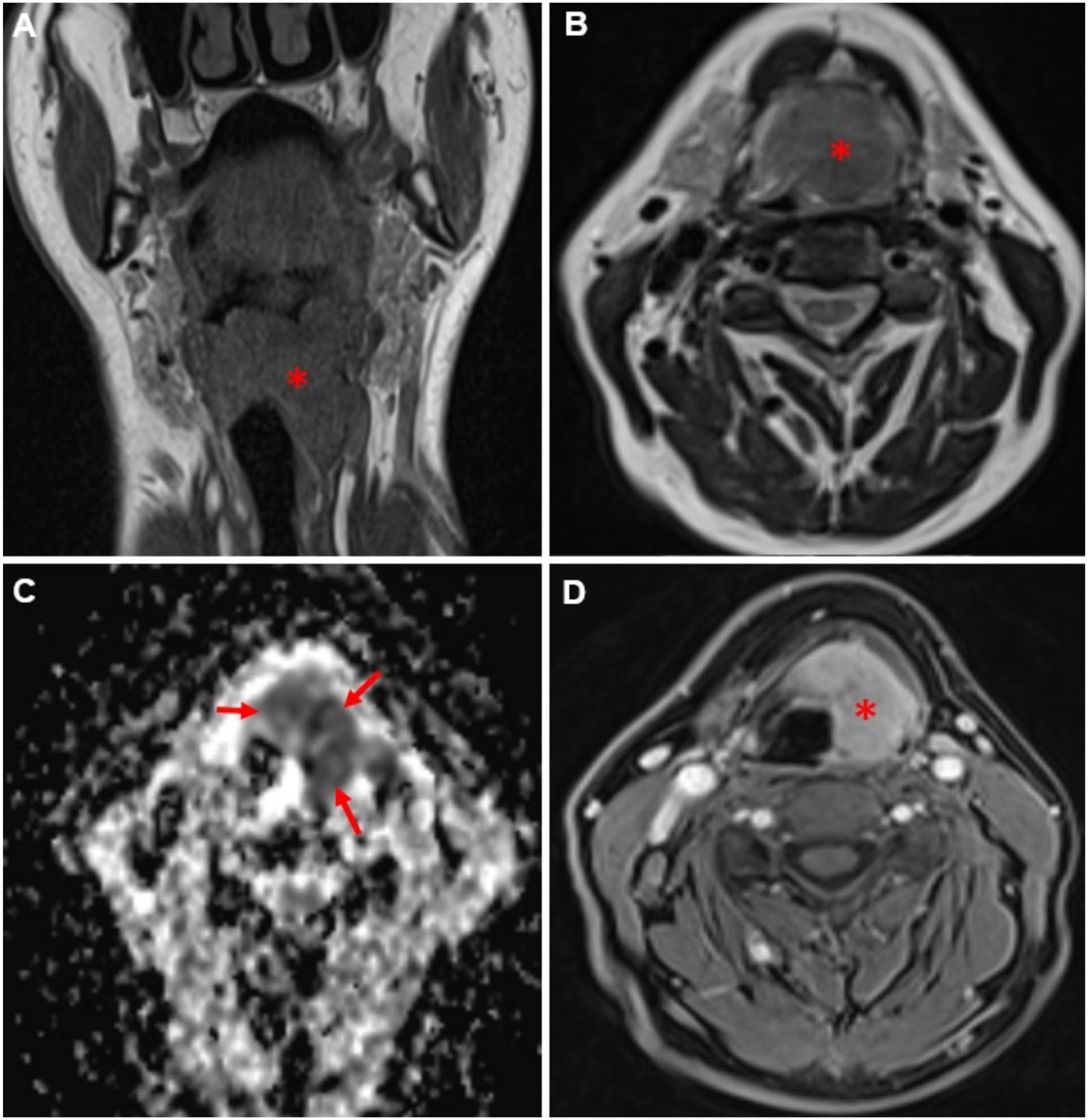
The laryngeal mass (asterix) is hypointenseon T1-weighted coronal section (A) and T2-weighted axial section (B). The mass restricts diffusion on apparent diffusion coefficient map (C) as shown by hypointensity (arrows). Postcontast T1-weighted axial section (D) shows intense homogeneous contrast enhancement.
EMP is a rare malignant type of plasma cell neoplasm. Although 80% of EMPs are observed in the head and neck area, predominantly within sinonasal lymphoid tissue, these lesions represent less than 1% of head and neck neoplasms. The occurrence of localization in the larynx is exceedingly uncommon, comprising a mere 0.04% to 0.45% of malignant laryngeal tumors and originating from the submucosal space. The epiglottis, vocal cords, false vocal folds, aryepiglottic folds, and thyroid cartilage are primarily impacted. Most patients are between 50 and 70 years of age at the time of diagnosis and the prevalence is higher in men at a ratio of 3:1.1,2 The symptoms are typically nonspecific and vary according to the location of the tumor, such as hoarseness or airway obstruction. The definitive diagnosis of the disease is based on histopathologic examinations and immunohistochemical tests showing monoclonality and the presence of plasma cells indicating neoplastic nature. Radiologic examinations are helpful in determining the location and extent of the lesion and in excluding other bone and soft tissue lesions and lymphadenopathy. CT usually shows a homogeneous laryngeal mass with smooth margins and mild to moderate contrast enhancement. Calcification and infiltrative growth pattern may be observed within the lesion. EMP may result from the infiltration of multiple myeloma or may represent the primary lesion, as observed in our case. Concurrently, the progression to multiple myeloma can be observed in approximately one-third of cases with EMP, which is associated with a poor prognosis. Consequently, diagnostic procedures such as bone marrow biopsy, positron emission tomography and MRI for lytic lesions and dissemination, serum protein electrophoresis, and immunoelectrophoresis are conducted.1,3,4 In patients with EMP, surgery was the primary treatment option before 1999, but in recent years, radiotherapy has become the preferred treatment due to the tumor’s radiosensitivity. In some cases, chemotherapy combinations are also applied. 5
Footnotes
Author Contributions
E.G.: idea, design, literature review, writing the article, references, and fundings. S.G.: design, control/supervision, critical review, materials. G.S.: control/supervision, critical review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases.
Informed Consent
We declare that written informed consent for patient information and images to be published was provided by the patient.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.