
Abstract

Significance statement
When reviewing a sleep study, examine the graphic summary to identify patterns, particularly changes in the apnea-hypopnea index across postures. If positional obstructive sleep apnea (OSA) is identified, laterality between the right and left lateral positions should be evaluated. If lateral positional OSA is detected, unilateral nasal obstruction should be suspected, as it can exacerbate OSA severity when lying contralateral to the obstructed side but alleviate it on the ipsilateral side.
A 66-year-old man was referred to the sleep clinic for unrefreshed sleep and years of snoring. His Epworth Sleepiness Scale was 11, with a Mallampati score of IV. His polysomnography showed severe obstructive sleep apnea (OSA) with an apnea-hypopnea index (AHI) of 34/hour. Notably, AHI was of 3 while sleeping on his right side (Figure 1, arrow and asterisk), compared with 24 on his left side and 30 on supine. The patient was referred to an otolaryngologist. A computed tomography scan of the sinuses for the patient revealed a deviated nasal septum to the right with mucus in the maxillary sinuses (Figure 2, arrow). He underwent septoplasty and then received continuous positive airway pressure (CPAP) treatment at a fixed pressure of 10 cm H2O after titration. The treatment resolved his daytime sleepiness, and he remains compliant with CPAP therapy.
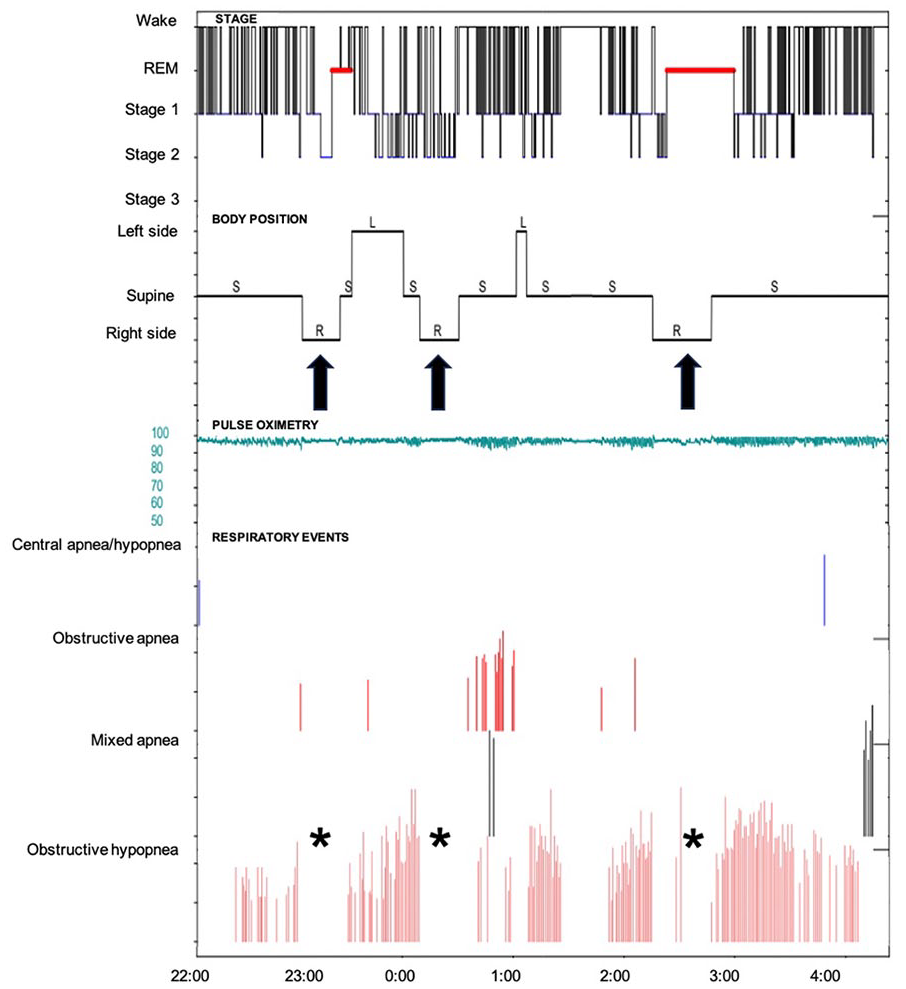
Graphical summary of polysomnography indicates that respiratory events primarily occurred in the left and supine positions but were scarce in the right lateral position (arrow and asterisk).
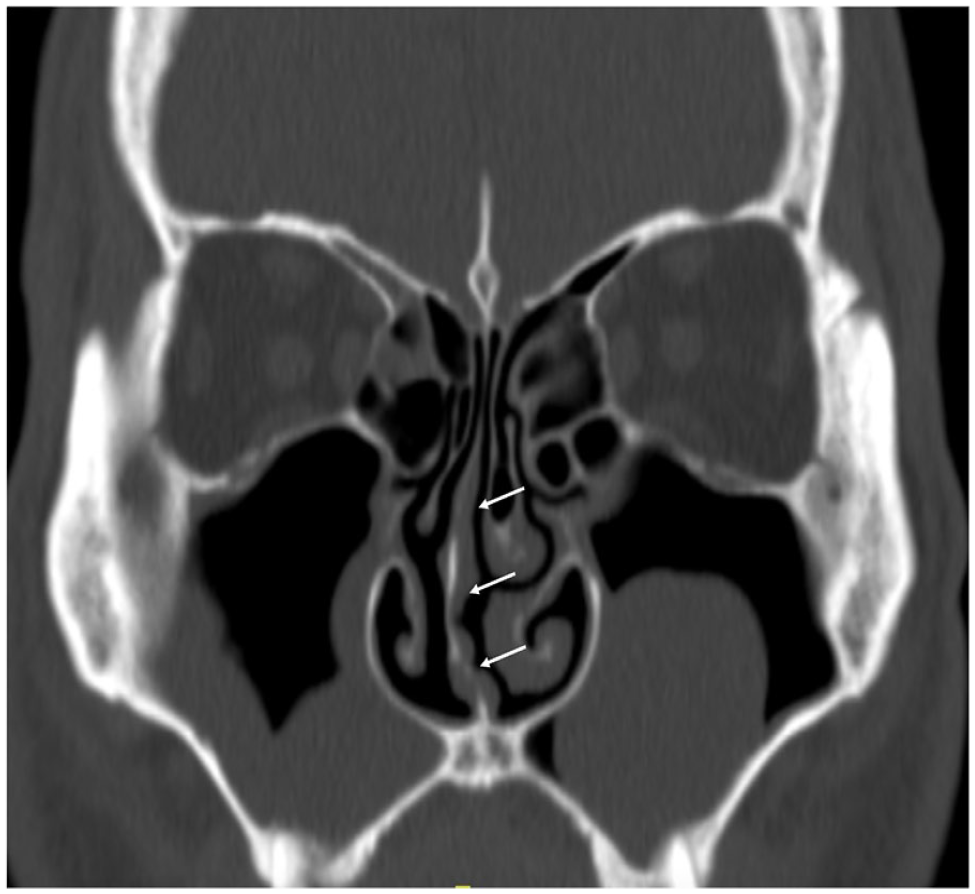
Computed tomography of the sinuses reveals the right-sided nasal septum deviation (arrow) and mucus in both maxillary sinuses.
Positional OSA, characterized by a more severe AHI in the supine position than in the non-supine position, is a prominent feature in about half of the patients with OSA. 1 Higher collapsibility in the supine position than in the non-supine position is a primary pathological mechanism in positional OSA. This increased collapsibility is attributed to a reduced functional residual capacity in lung volume and a more elliptically-shaped upper airway in the supine position. 2 It is also possible that increased nasal resistance due to nasal venous stasis in recumbency, 3 leading to upper airway collapse, could contribute to positional OSA. Consequently, one might expect greater nasal resistance in the supine position than in the non-supine position, which could explain positional OSA. However, studies have shown that total nasal resistance in patients with OSA either slightly increased or remained unchanged when moving from the supine to the non-supine position.4,5 This stability in total nasal resistance during sleep across different postures is attributed to the “nasal cycle”—the periodic swelling and decongestion of the nasal mucosa. This cycle results in alternating airflow between the left and right nostrils every 2 to 3 hours, maintaining stable total nasal resistance with constant bilateral airflow. 6 During sleep, the difference in nasal resistance between the right and left nasal cavities is more pronounced than in the upright position. 7 However, the alternating airflow of the nasal cycle persists, compensating to maintain stable total nasal resistance throughout the night. 7
Another mechanism that helps maintain the stability of bilateral nasal airflow between the supine and non-supine positions is the corporal-nasal reflex. Lateral recumbency, with pressure on the axilla and hips via proprioceptive stimulation, can enforce congestion and decongestion of the ipsilateral and the contralateral side of the nasal cavities, respectively.3,8 Therefore, pressure applied on one side of the body causes ipsilateral nasal venous congestion with increased nasal resistance (decreased airflow) and contralateral decongestion with decreased nasal resistance (increased airflow).
These mechanisms work together to maintain constant nasal resistance in individuals with normal nasal structures during sleep. If unusual increases in nasal resistance are detected, which could aggravate the severity of OSA, this may indicate unilateral nasal obstruction.5,9
Since the patient’s respiratory events predominantly occurred while he slept on his left side—a position that typically decreases resistance and increases airflow through the right nostril while the left nasal cavity in dependent position becomes congested with decreased airflow—it can be inferred that his right nasal passage was obstructed. This obstruction would increase upstream airflow resistance, elevate the negative collapsing pressure, and make the pharynx more prone to collapse, thereby contributing to OSA.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for the publication of this manuscript