
Abstract
Introduction
Facial nerve paralysis is a complex disease, which can lead to a partial or complete lack of facial movement. This not only leads to functional deficits such as poor eyelid closure, oral incompetency, difficulty with phonation of labial sounds, and external nasal valve stenosis but may also cause significant psychological trauma leading to isolation and worsening quality of life.1,2 Treatment is variable and may depend on the degree and timing of onset of facial paralysis. Facial reanimation options include observation, neuromuscular retraining, botulinum toxin injection, and surgical options including static slings, nerve and regional muscle transfers, myectomies, neurectomies, and microvascular free-muscle transfers. 2 Given the variety of options available and the possibility of worsening a patient’s paralysis and function, it is critical for patients to seek treatment from providers who are well trained in facial reanimation and can provide patients with a comprehensive and individualized treatment strategy.
Social medial use has become increasingly prevalent in medicine and within the field of facial plastic surgery.3-6 A survey showed that 80% of facial plastic surgeons used social media professionally with those in private practice more likely to utilize social media professionally. 6 Additionally, nearly half of all patients reference social media when seeking plastic surgery care and 40% of these patients were strongly influenced by its content. 7 While online and social media–based resources may have benefits for patient education, the reliability of these resources is not guaranteed due to lack of peer review. There are numerous studies from a variety of specialties, which describe the poor quality and reliability of medically-based social media posts.8-17 Within the last decade, there has been an increase in the number of social media posts regarding facial paralysis.4,18 However, there is a lack of literature regarding the quality of social media posts related to facial reanimation. Since YouTube and Facebook are the most used social media platforms by age groups seeking information on facial paralysis and facial reanimation, the authors sought to describe the landscape regarding facial paralysis on these platforms. 19 The objectives of this study were to assess the presence and quality of posts related to facial reanimation on YouTube and Facebook and to identify potential gaps in social media resources for patients with facial paralysis.
Methods
Ten key search terms (KSTs) related to facial reanimation were identified. The authors determined that these KSTs would be the most searched phrases that encompassed facial reanimation. These KSTs included “facial reanimation,” “gracilis free flap,” “gracilis muscle facial nerve,” “gracilis muscle facial paralysis,” “synkinesis,” “cross face nerve graft,” “cross nerve innervation,” “facial paralysis,” “facial paralysis treatment,” and “facial paralysis surgery.” The top 10 posts from each KST were obtained from YouTube and Facebook. Dummy accounts were created to prevent any search result bias due to previous YouTube and Facebook searches. Specifically, within Facebook, channels searched included Facebook Videos, Facebook Photos, Facebook Pages, and Facebook Places. For video posts, data were also collected on the number of views, length of video, source, and location of the video source. For Facebook Photos, data were collected on source, location, purpose of the post, and whether the post showed preoperative and postoperative images. For Facebook Photos, only 9 photographs were included due to lack of further data. For Facebook Pages and Facebook Places, data were also collected on location and whether the page or place was an academic or private practice entity. Exclusion criteria included social medial posts with no English translation or posts unrelated to facial paralysis or reanimation (Figure 1).
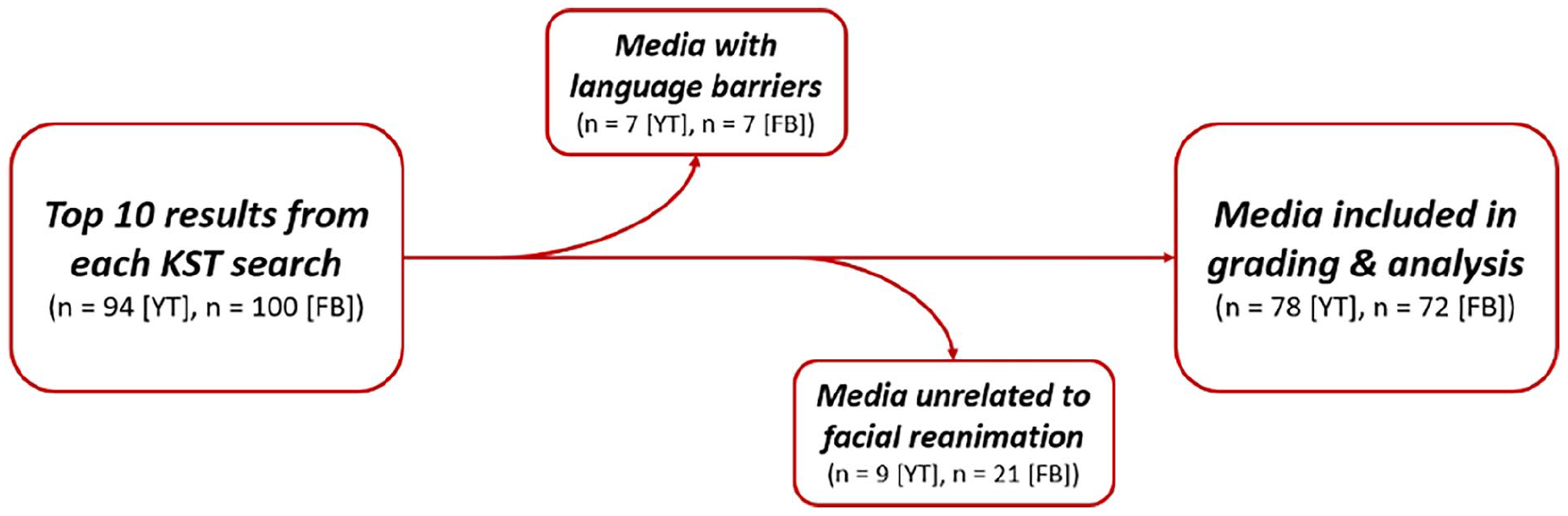
Figure describing inclusion and exclusion criteria.
Grading Tools
Grading tools utilized included Journal of the American Medical Association (JAMA) Criteria, Global Quality Score (GQS), and Modified DISCERN. For video grading, the authors also implemented their own grading scale, the Social Media Quality Score (SMQS). JAMA Criteria was used to evaluate the reliability of Facebook Pages and Facebook Places. One point was awarded for each of the following categories: authorship, attribution, disclosure, and currency (Supplemental Figure 1). GQS was used to rate YouTube and Facebook Videos on flow, quality, and usefulness on a 5-point Likert scale (Supplemental Figure 2). GQS of 1 or 2 indicate low-quality videos, 3 indicates medium-quality videos, and 4 or 5 indicate high-quality videos. Modified DISCERN was used to grade the quality of YouTube and Facebook Videos. One point was awarded to each “yes” answer for the following questions concerning a post (Supplemental Figure 3):
Is the video clear, concise, and understandable?
Were valid sources cited?
Is the provided information balanced and unbiased?
Are additional sources of information listed for patient reference?
Does the video address areas of controversy/uncertainty?
The SMQS was created by the authors to grade YouTube and Facebook Videos based on content and source. Higher quality videos represented video posts that would be more useful to a patient searching for information on facial reanimation (Supplemental Figure 4). The highest grade (score of 1) was a source, which provided patient education from a qualified expert. Qualified experts were determined by evaluating the credentials of the author to determine whether they had an advanced degree and/or credentials (such as fellowship training in facial plastic or plastic surgery) or whether the work was created through an institution of higher learning. If neither was present, the authors evaluated whether the source had an established presence in the topic. If not, they were considered an unqualified source.
Statistical Analysis
Qualitative analysis was performed for the data collected. For the video posts, the mean scores by KST were analyzed using the Kruskall-Wallis test. The video length was analyzed using an ANOVA test. The grading scores comparing YouTube and Facebook Videos were compared using a student’s t-test and a chi-squared test. SAS was used for statistical analysis. Statistical significance was set at P < .05.
Results
YouTube Videos
The results of the YouTube video analysis are shown in Table 1. There was a significant difference between KSTs in views (P < .01) and SMQS (P < .01). Highest views were returned by the KSTs “facial paralysis treatment” and “facial paralysis,” while “gracilis muscle facial nerve” yielded the lowest views. Thirty-six (46.2%) out of 78 videos evaluated came from academic sources. Twenty-nine (37.2%) came from nonacademic but qualified sources, while 10 (12.8%) came from patient or parent reports. Three (3.8%) of the 78 videos came from other sources. There was a significant difference between KSTs by location (P < .001) with the majority of the videos being from the United States.
Means by KST for YouTube Videos.

Abbreviations: GQS, Global Quality Score; KST, key search term; SMQS, Social Media Quality Score.
Kruskall-Wallis test.
ANOVA.
Facebook Videos
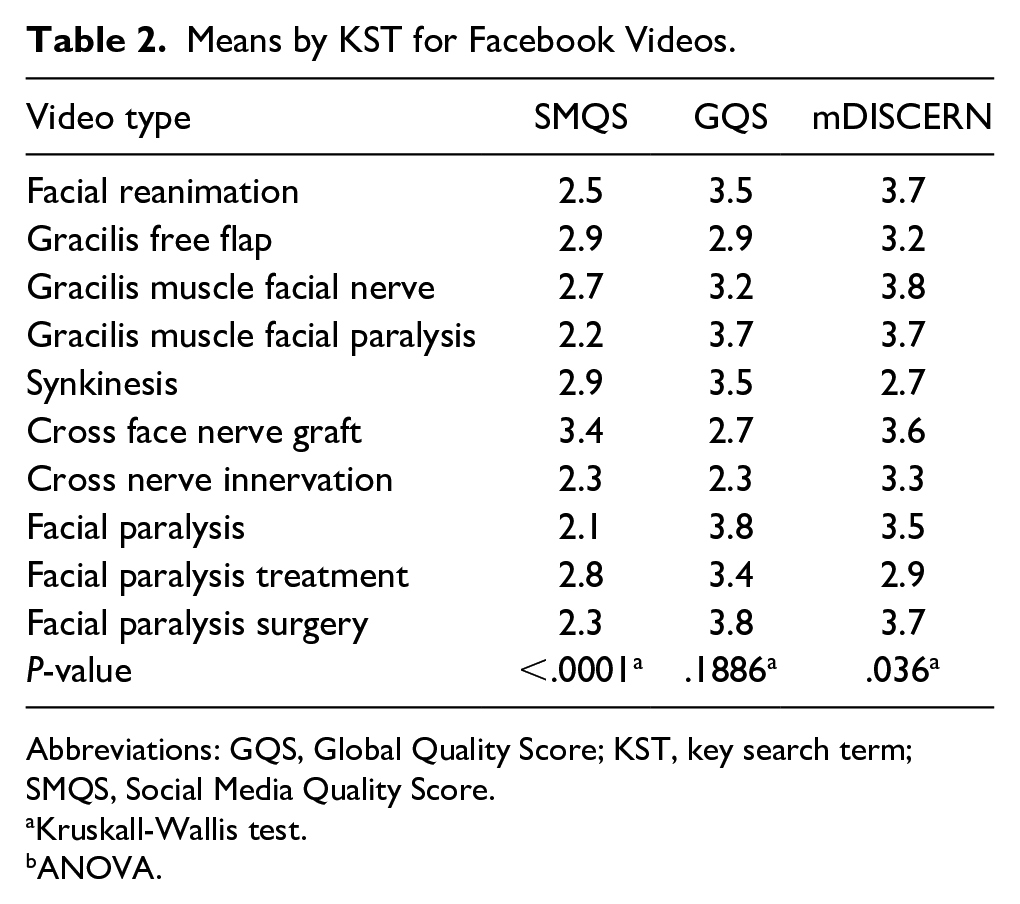
The results of the Facebook video analysis are shown in Table 2. There was a significant difference between KSTs in SMQS (P < .01) and Modified DISCERN (P = .036). Forty-six (63.9%) out of 72 videos evaluated came from academic sources, 13 (18.1%) came from nonacademic but qualified sources, while 13 (18.1%) came from patient or parent reports. There was no significant difference between KSTs in location (P = .089) with the majority of the videos being from the United States.
Means by KST for Facebook Videos.
Abbreviations: GQS, Global Quality Score; KST, key search term; SMQS, Social Media Quality Score.
Kruskall-Wallis test.
ANOVA.
YouTube Videos Versus Facebook Videos
Comparison between YouTube and Facebook videos are shown in Table 3. YouTube videos were significantly longer than Facebook videos (median 694.9 seconds vs 255.9 seconds, P < .01). There were significant differences between YouTube and Facebook videos when comparing GQS (P = .01) and SMQS (P = .035), with no difference in Modified DISCERN (P = .595). YouTube tended to have a higher number of patient education videos from a qualified expert and surgical technique videos, while Facebook had a higher number of academically-based patient anecdotes.
Video Characteristics by Social Media Category.

Abbreviations: GQS, Global Quality Score; SMQS, Social Media Quality Score.
Student’s t-test.
Chi-square.
Facebook Photos
For Facebook photographs, 55.1% had both preoperative and postoperative photographs compared to 44.9% which had no preoperative and postoperative photographs. Of the photographs reviewed, 79.5% came from nonacademic or qualified sources, followed by 3.8% from patients and 3.8% from academic sources, 12.8% of photographs came from “other” sources. Of the photographs collected, 77.4% were obtained from the United States, 6.0% from India, and 3.6% from Egypt. The photographs were also categorized based on the primary purpose of the post: 52.9% were medical, 23.0% were educational, 9.2% were career/marketing, 5.8% were personal, 4.6% were surgical, and 4.6% were news (Figure 2).
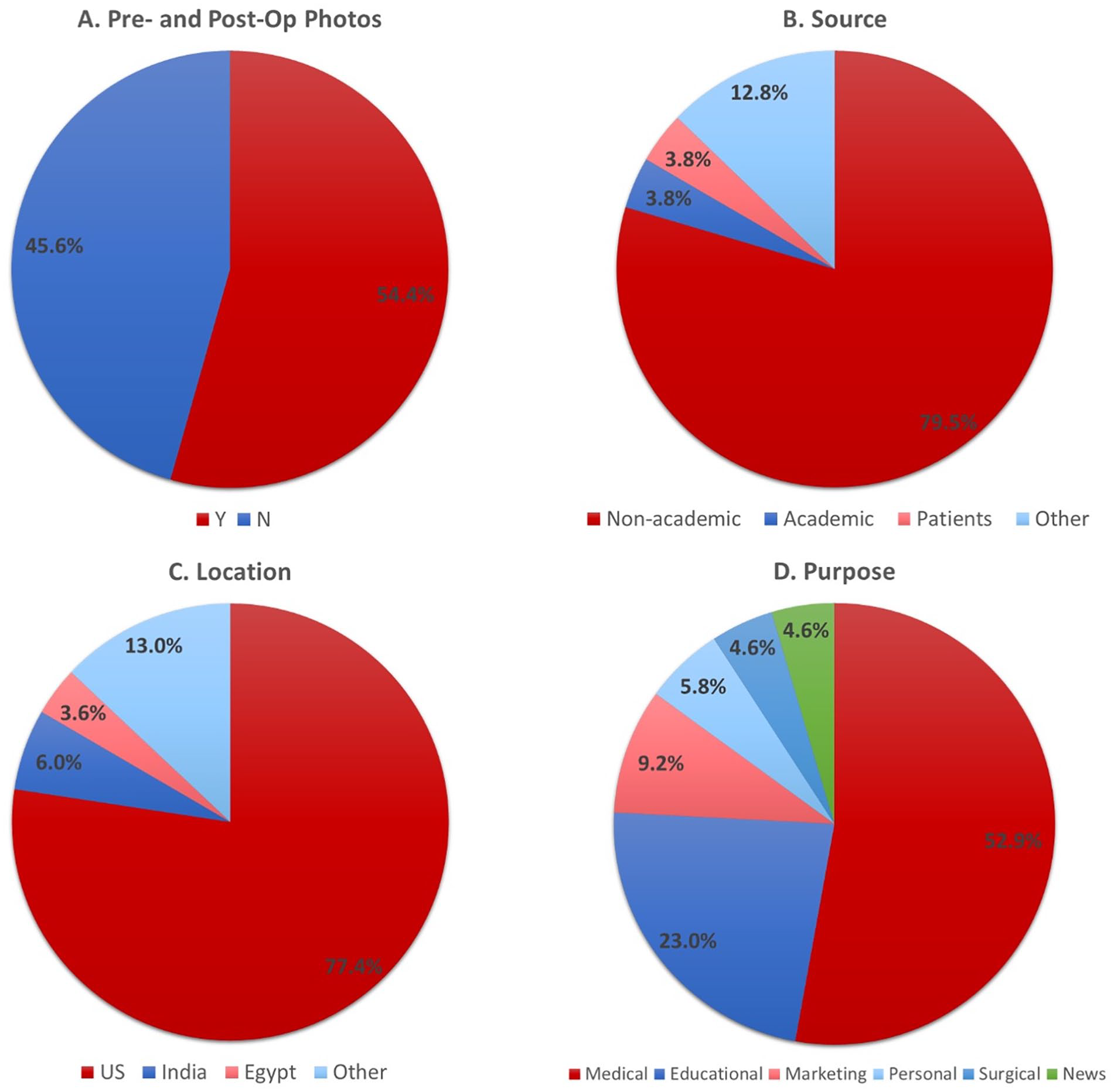
Distribution of Facebook photographs search results by (A) the presence of pre- and post-op photographs; (B) source type; (C) location by country; and (D) primary purpose of post.
Facebook Pages and Places
For Facebook pages, 30.4% were considered academic compared with 69.6%, which were considered private practice. For JAMA classification, the mean was noted to be 3.48 with a standard deviation of 0.64. The median was 4.0. Regarding location, 51.8% of pages were from the United States, followed by 8.4%, which were from India, and 7.2% from Canada. For Facebook places, 45.5% were considered academic compared with 54.6%, which were considered private practice. For JAMA classification, the mean was noted to be 3.68 with a standard deviation of 1.03. The median was 4.0. Regarding location, 63.2% of pages were from the United States, followed by 4.6% from Thailand and 4.6% from Germany (Figure 2).
Discussion
In this study, we found that there was a significant difference in SMQS and GQS between YouTube and Facebook Videos with YouTube having an increased likelihood of having higher quality videos. Specifically, Facebook tended to have a higher number of academically-based patient anecdotes, while YouTube tended to have a higher number of patient education videos from a qualified expert and surgical technique videos. Although there are high-quality videos on both platforms, there were a considerable number of moderate or low-quality videos—58% of videos had a GQS of moderate or poor quality with 28% having a GQS of poor quality. Of note, when searching certain KSTs on YouTube, there is a separate category of videos denoted “From Health Sources.” While there were not many videos in this category, they were relatively high quality based on GQS, Modified DISCERN, and SMQS. This new category may represent content, which may be more reliable in its quality compared with videos not under this heading. In summary, while there was some high-quality material on both YouTube and Facebook Videos, there was a large proportion of low-quality content, which may be viewed by patients who are not able to determine the quality of the post. Thus, it is imperative that when surgeons post on social media, they post high-quality content that is appropriately labeled and can be found by patients. The most common pitfalls of low-quality posts were either posts from an unqualified source or material that was not relevant or useful to patients (such as advertising/marketing campaigns). A recently-published article suggested that the most common searches regarding facial paralysis are in regard to etiology and treatment. 20 Ideally, surgeons and other qualified experts should focus on creating material that explains the disease process, etiology, and symptoms, highlights the variety of potential treatment options, discusses the potential risks and benefits of these options, and directs patients to potential resources such a support groups and qualified providers who may provide treatment.
For YouTube videos, we noted a significant difference in SMQS between various KSTs, and for Facebook videos, we noted a significant difference in both SMQS and Modified DISCERN between KSTs. This suggests that the search terms patients utilize to find content may significantly affect the quality of the content they view. However, no single KST consistently had improved scores. Interestingly, the KST with the highest views, “facial paralysis treatment,” had relatively-low scores in all 3 grading systems than its counterparts, suggesting that the most viewed search term was providing worse quality information. This gives rise to 2 areas of improvement for surgeons who perform facial reanimation. As providers, we need to give patients better quality search terms, which they can use to find high-quality information. As educators, when producing this content, we need to be deliberate with assigning the “key words,” which allow our content to be located and utilized.
Many of the posts in Facebook Photos, Places, and Pages did not meet the authors’ inclusion criteria, and only a qualitative analysis was performed. The majority of these posts were from nonacademic sources, which is consistent with previous studies. This may potentially be related to institutional barriers at academic institutions, which may not allow a social media presence. 6 Facebook Photos yielded diverse content ranging from medical and surgical posts, educational posts, marketing, or personal posts. Facebook Places and Pages were evaluated by the JAMA criteria with scores of 3.68 and 3.48, respectively. Although these scores are relatively high, given the low sample size, definitive conclusions cannot be made about the quality of this content. Although the posts on Facebook Photos, Places, and Pages do have some quality content, there are still gaps in these channels, and there is plenty of opportunity for health professionals to further capitalize on these outlets.
Since its advent, social media has significantly changed daily life within society and its use continues to increase significantly.4,18,19 It is not surprising that many people are utilizing social media to direct their health care. This may include learning about disease processes, treatment options, and even deciding to undergo surgery or select specific providers based on those provider’s social media posts.7,21,22 This ease of access provides a great benefit for patients who wish to understand their medical problems and treatment options and, in the best case scenario, allows patients with lower health literacy to make educated decisions about their health care. However, this is dependent on accurate information in social media posts, which have virtually no form of peer review. There have been numerous studies which have demonstrated that some of the medical information on social media is of lower quality and may not greatly benefit patients.8-17 While the subpar quality of this content may be obvious to health care providers who are experts in their respective fields, this may not be easily distinguished by patients. Thus, high-quality social media posts are required in order to successfully educate and benefit patients.
Additionally, with the development of large language models such as ChatGPT, there is an even greater need to ensure that the quality of medical information online and on social media is accurate. This is especially pertinent if artificial intelligence models use social media posts to create their content—they may inadvertently use low-quality posts as their source material leading to the distribution of poor-quality information. However, artificial intelligence also has the potential to significantly improve the quality of social media posts if used judiciously. A recent study compared the performance of ChatGPT versus an expert rhinoplasty surgeon in answering preoperative and postoperative questions about septorhinoplasty. They found that ChatGPT had significantly-higher ratings in accuracy, completeness, and overall quality of responses and was preferred over the expert rhinoplasty surgeon. 23 Additionally, artificial intelligence can effectively provide indications and management of complications regarding tympanostomy tube insertion, can provide accurate patient educational material regarding obstructive sleep apnea, and can successfully lower the reading level of online patient materials to allow for improved reading accessibility.24-26 While the benefits of artificial intelligence are impressive, other studies have warned against potential inaccuracies of these large language models and caution against their immediate implementation for providing patient education materials.27,28 As health care providers who are on the forefront of our respective fields, we must find a way to bridge these 2 dichotomies. Ideally, we will find ways to utilize programs such as ChatGPT and search engine machine learning algorithms to help surgeons emphasize specific patient education topics in their preoperative and postoperative appointments in order to allow for optimum care. 29 Given that social media has become increasingly prevalent in health care within the last decade, it is not unreasonable to predict that artificial intelligence will follow a similar trend. As health care providers, we must understand the previous shortcomings in our use of social media and try to anticipate the integration of artificial intelligence into medicine so that we can leverage this new technology judiciously for our patient’s benefit.
Limitations
A limitation of this study was that the social media searches were confined to YouTube and Facebook. Although they are the 2 most used platforms, Instagram, Snapchat, and TikTok are more commonly used by Americans under the age of 30, and studying these platforms may be a future avenue of investigation. 19 Additionally, given the subjective and nonvalidated nature of some of the grading scales utilized in this study, there may be some level of bias, which was unintentionally introduced. Also, the ten KSTs used in this study may not fully encompass all facial reanimation procedures. Finally, the search results may be biased due to the proprietary algorithms on YouTube and Facebook, potentially biasing the results.
Conclusions
Social media will continue to be used by patients to direct their health care choices. Regarding facial reanimation, our study found YouTube may have higher quality videos than Facebook videos. However, both platforms have a considerable number of moderate or poor quality videos. Additionally, there was a significant difference in the quality of videos encountered depending on the search terms utilized. Our findings suggest that higher quality posts regarding facial reanimation are needed on social media. As health care providers, we must provide patients with appropriate resources and search terms, so they may find high-quality posts, and when posting content, we must carefully curate the “key words” so that this content is readily accessible by patients.
Supplemental Material
sj-tiff-1-ear-10.1177_01455613241307886 – Supplemental material for Assessing the Quality of Social Media Content Regarding Facial Paralysis and Reanimation
Supplemental material, sj-tiff-1-ear-10.1177_01455613241307886 for Assessing the Quality of Social Media Content Regarding Facial Paralysis and Reanimation by Kevin Ngo, Lacy S. Brame, Aniruddha C. Parikh and Mark M. Mims in Ear, Nose & Throat Journal
Supplemental Material
sj-tiff-2-ear-10.1177_01455613241307886 – Supplemental material for Assessing the Quality of Social Media Content Regarding Facial Paralysis and Reanimation
Supplemental material, sj-tiff-2-ear-10.1177_01455613241307886 for Assessing the Quality of Social Media Content Regarding Facial Paralysis and Reanimation by Kevin Ngo, Lacy S. Brame, Aniruddha C. Parikh and Mark M. Mims in Ear, Nose & Throat Journal
Supplemental Material
sj-tiff-3-ear-10.1177_01455613241307886 – Supplemental material for Assessing the Quality of Social Media Content Regarding Facial Paralysis and Reanimation
Supplemental material, sj-tiff-3-ear-10.1177_01455613241307886 for Assessing the Quality of Social Media Content Regarding Facial Paralysis and Reanimation by Kevin Ngo, Lacy S. Brame, Aniruddha C. Parikh and Mark M. Mims in Ear, Nose & Throat Journal
Supplemental Material
sj-tiff-4-ear-10.1177_01455613241307886 – Supplemental material for Assessing the Quality of Social Media Content Regarding Facial Paralysis and Reanimation
Supplemental material, sj-tiff-4-ear-10.1177_01455613241307886 for Assessing the Quality of Social Media Content Regarding Facial Paralysis and Reanimation by Kevin Ngo, Lacy S. Brame, Aniruddha C. Parikh and Mark M. Mims in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
This study was presented at the 2023 Combined Otolaryngology Spring Meeting, May 3 to 7, 2023.
Author Contributions
K.N.: investigation, data curation, and writing—original draft, review, and editing. L.B.: conceptualization, formal analysis, and writing—original draft, review, and editing. A.P.: conceptualization, formal analysis, and writing—original draft, review, and editing. M.M.: conceptualization, methodology, writing—review and editing, and supervision.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study is IRB exempt as no patient data were used during this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.