
Abstract
Introduction
The parotid glands are the largest salivary glands in the body, and changes in their cellular structure can lead to the development of localized tumors. 1 The frequency of tumors in the salivary glands has been reported to be 15 in 100,000. Parotid tumors are the most common salivary gland tumors, with the majority benign.1,2
Parotidectomy is a surgical procedure performed for benign and malignant lesions located in the parotid gland. In 2014, 3530 parotidectomy procedures were reported in the United States. 3 The parotid tissue consists of superficial and deep lobes, with the facial nerve located between these 2 lobes. The modified Blair incision is commonly used for both superficial and deep lobe lesions located in the parotid gland.1,2,4 This incision, first described by Blair in 1918 and modified by Bailey in 1941, has been used for parotidectomy as the standard incision since then. This incision includes cuts in different planes including vertical, oblique, and horizontal cuts throughout the pre- and infraruriculer skin region. 5 This incision allows easy access to the parotid gland, and clear visualization of the parotid region. Also, by this incision, a wide exposure of facial nerve and its branches is obtained. It allows one to see and preserve the facial nerve and branches during the removal of tumor tissue. The incision also facilitates easy access to the upper jugular lymph nodes when necessary.
All types of surgical incision can lead to scar formation. Regardless of the extent of resection in parotidectomy, patients may face cosmetic problems in the preuricular, infra-auricular, and retromandibular regions postoperatively. Deformities in this area can negatively impact an individual, highlighting the importance of achieving cosmetically-pleasing results after surgery, especially considering that benign parotid masses are relatively more common in younger populations. 6
Surgical complications of parotidectomy are classified as major and minor. Scar formation, with an incidence rate of 12%, has been reported to be the most bothersome complication of surgery. In addition to aesthetic problems after surgery, some complications such as numbness and the development of Frey syndrome can also occur. 7 The primary objective of reconstruction procedures after resection during surgery is to prevent the complications mentioned above.
Epidermos cream is made up of boric acid, coconut oil, and sea buckthron, which helps repair damaged tissues in the upper and middle layers of the skin by stimulating new collagen production. It is commonly used to preserve the natural protective barrier of the skin that helps keep the skin supple and moisturized.
The purpose of this study was to evaluate the effect of epidermos barrier cream on postoperative parotidectomy incision scars.
Methods
The study received approval from the Mugla Sitki Kocman University Clinical Research Ethics Committee with number 9/X and the date of April 13, 2023. Subsequently, approval was obtained from the Ethics Committee of the Turkey Medicines and Medical Device Agency of the Turkish Ministry of Health with the number E-68869993-511.06.01.02-1189653 and the date of August 11, 2023.
Surgical Procedure
The study was carried out in the Department of Otorhinolaryngology of Mugla Sitki Kocman University Faculty of Medicine. Patients who underwent superficial parotidectomy due to benign parotid masses were included. In the study, patients aged 18 to 65 years were included without any diseases that can affect wound healing (such as type 2 diabetes). All patients underwent a preoperative evaluation with fine needle aspiration biopsy, and those with benign pathology (MILAN classification IVA) were included in the study. Patients who needed additional treatment that could affect wound healing, such as malignant parotid masses or those with systemic diseases, were not included in the study.
A total of 46 patients who underwent surgery for parotid masses were included in the study. All patients underwent a standard surgical procedure by the same surgeon. A modified Blair incision was made in all patients to access the parotid gland. Facial nerve monitoring was performed in all cases. Following the incision, a subsuperficial musculoaponeurotic system (SMAS) and subplatysmal skin flap were raised in all patients. The posterior branch of the great auricular nerve was preserved in all cases. Subsequently, the superficial parotid tissue was excised by identifying and following the facial nerve trunk in an anterograde manner. To prevent defects and potential complications, a sternocleidomastoid muscle (SCM) flap was rotated to the defect area in all patients. The flap was rotated superiorly on the upper part of the SCM, covering the area of the defect. A drain was placed in the cavity. Closure was achieved by suturing the platysma and SMAS tissues, followed by subcutaneous tissue with absorbable vicryl sutures. The skin was sutured with nonabsorbable prolene sutures individually spaced 10 mm apart. Finally, the operation was completed with a standard parotid dressing.
Follow-Up
During the postoperative period, patients were monitored in the hospital until drains were removed. Standard prophylactic antibiotics were administered during hospitalization. The patients were discharged after drain removal. The sutures were removed on the seventh postoperative day. Following the removal of the suture, patients were included in the study or the control group. To minimize the impact of possible external factors (such as season, nutrition, etc) on recovery and to avoid selection bias, patients were sequentially assigned to the study and control groups. In the study group, epidermos barrier cream was applied to the wound after suture removal. The control group, on the other hand, underwent the healing period without any treatment. The epidermos barrier cream was applied twice a day, in the morning and in the evening, covering the wound area.
The wound sites of the patients were evaluated during the routine follow-up period as in the first, second, and fourth weeks. The evaluation was made by a senior head and neck surgeon who did not know in which group the patient included. The first check-up was performed in the first week, where the sutures were removed, and the patients were assigned to the study or control group. The second check-up was carried out in the second week along with the assessment of pathological results. The pathological results were pleomorphic adenoma in all cases. The final check-up was performed during the first month of the wound site examination. These 3 follow-ups were part of the routine postsurgical follow-up, and patients were not called for additional evaluation unless there were other issues requiring additional treatment (Figures 1–4).

Patient follow-up in the study group.

Patient follow-up in the control group.

Long-term results in the study group.

Long-term results in the control group.
All study patients were asked to subjectively evaluate their wound sites in the first, second and fourth weeks using a patient assessment form during these periods. All participants were explained the routine postoperative surgical follow-up period. The possible positive effects of cream were detailed, as well as the possible negative effects. To prevent a possible bias effect, possible negative effects such as possible maceration and possible skin reaction were also explained. This way, we tried to prevent the bias of believing their scars were better.
The patients were evaluated with a six-item questionnaire in each evaluation. This questionnaire includes scoring the scar in 6 values (from 0 to 5) to evaluate how the patient perceives the scar at the surgical site, checking for any dehiscence at the scar site, redness and color changes at the edges of the scar, the presence of sensory loss at the scar area, and signs of infection at the edges of the scar. Additionally, the scar sites were scored in a standardized environment at each follow-up (the scar site was viewed from the side at a distance of 30 cm in daylight for a clear view). In this evaluation again, we used a 6° grading system (from 1 to 6), the scar structure was aesthetically assessed as follows: good scar healing level (1-2 points), moderate scar healing level (3-4 points), and poor scar healing level (5-6 points). This classification system starts from 1 to 6 to prevent 0 degree as a non-scar that may affect the study results.
Statistical Analysis
Statistical analyses of the study were performed using the SPSS software (IBM Corp Released 2020; IBM SPSS Statistics for Windows, Version 27.0., IBM Corp). Chi-squared and Fisher-Freeman-Halton analyses were applied to compare categorical variables between independent groups. The descriptive statistics of the qualitative variables were presented as frequency (n) and percentage (%). Values of P < .05 were considered statistically significant.
Results
There were no statistically-significant differences in terms of age distribution between the groups (P > .05). There were also no statistically-significant differences between the groups in terms of gender (P = .788). All patients had pleomorphic adenoma as a result of tumor resection pathology. In the control group, the mean tumor size was 26.36 mm (SD: 10.68 mm), and in the study group, the mean tumor size was 25.63 mm (SD: 10.62). There were statistically-significant differences between the groups in terms of tumor size (P = .836).
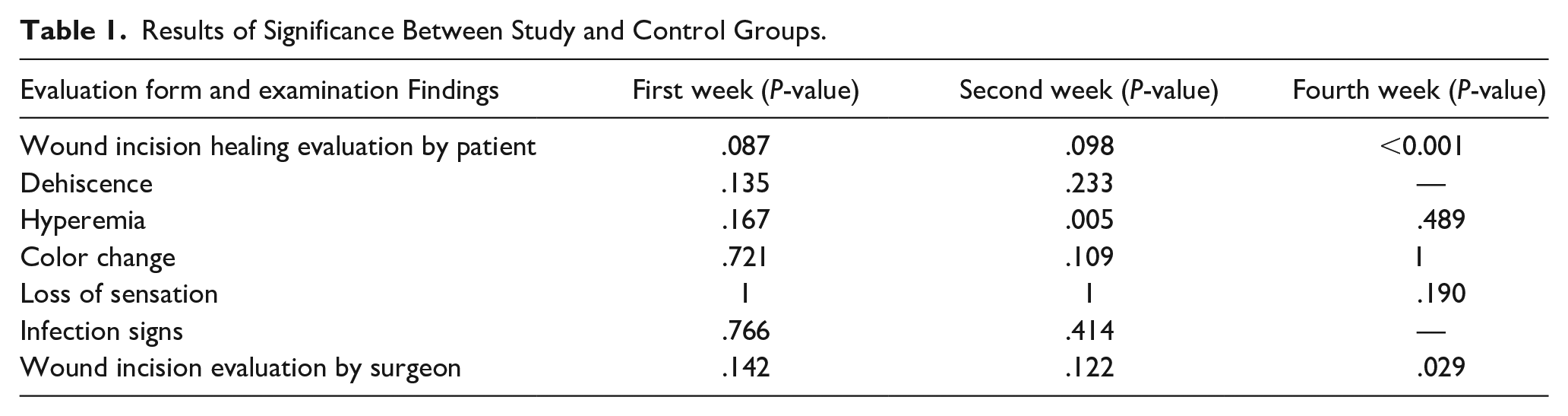
According to the results of the evaluation of the questionnaire that inquired about wound sites in the first week, statistically-significant differences were not observed between the groups in terms of scar formation at the wound site (P = .087), presence of skin dehissance (P = .135), presence of hyperemia (P = .167), change in color at the edges of the wound (P = .721), loss of sensation in the wound area (P = 1), and the presence of signs of infection in the wound area (P = .766). Similarly, no statistically-significant differences were observed in the evaluation of scar formation at the wound site in the first week (P = .142).
In the results of the evaluation of the questionnaire inquiring about the wound sites in the second week, statistically-significant differences were not observed between the groups in terms of scar formation at the wound site (P = .098), presence of skin dehiscence (P = .233), change of color at the edges of the wound (P = .109), loss of sensation in the wound area (P = 1), and the presence of signs of infection in the wound area (P = .414). However, a statistically-significant difference was observed between the groups in terms of the presence of hyperemia around the wound site (P = .005). In the study group, hyperemia was observed to be more frequent than in the control group. Furthermore, no statistically-significant differences were found in the evaluation of scar formation at the wound site in the second week (P = .122).
According to the results of the evaluation of the questionnaire inquiring about wound sites in the fourth week, there were no statistically-significant differences between the groups in terms of hyperemia at the wound edges (P = .489), color change at the wound edges (P: 1), and loss of sensation in the wound area (P = .190). Since no patients had skin opening or infection around the edges of the wound during this period, evaluations of these aspects between groups were not conducted in the fourth week. Based on the questionnaire completed by the patients, a statistically-significant difference between the groups was observed in terms of scar formation in the evaluation of the wound in the fourth week (P < .001). A statistically-significant difference was found in the evaluation of scar formation at the wound site in the fourth week, which was performed by the patient's surgeon (P = .029).
When evaluation was performed within each group in terms of scar, a continuous improvement was observed from the first week to the fourth week in both groups. The scar healing process within each group was statistically significant (P < .001; Table 1).
Results of Significance Between Study and Control Groups.
Discussion
Scar formation in the facial region significantly affects the quality of life of the patient. Scar formation has been reported as the most disturbing complication of parotidectomy in one of the studies. 7 Therefore, various modifications of classic incisions have been reported to reduce this scar formation. 8
Scar formation can be classified into 4 different types: tense (flat), contracted, atrophic (depressed), and raised. 9 Sometimes, multiple phenotypes can be observed in a single wound. Flat scars are the least symptomatic and are generally considered the normal scar phenotype. This type of scar tissue usually takes on the color of the body later on and progresses without any symptoms. Flat scar tissue usually forms when the edges of the wound are under tension. Contracted scar tissue is typically observed in cases where the wound tissue is tense and damaged. This type of scar tissue often causes pain and can sometimes cause loss of function. 10 Atrophic scars are below the surface level. Raised scars are usually called hypertrophic scars or keloids and are the most troublesome type of scar for the patient in terms of cosmetics, symptomatic, and psychological impact. 11
To prevent scar formation, silicone-based topical creams are commonly used. 12 Silicone-based creams are inert with no active components, but improve general skin healing conditions by providing occlusion and hydration. 13 Furthermore, natural substances such as aloe vera, green tea, and onion extract, with antioxidant and anti-inflammatory properties, have been reported to reduce inflammation and prevent excessive collagen production. 11
Frequently-postoperative dressing changes have been reported to affect superficial healing tissue by causing inflammation and edema. 14 Therefore, barrier creams are now commonly used, especially during the pandemic, for postoperative wound care. Epidermos wound care cream contains Hippophae rhamnoides (sea buckthorn) oil, Cocos nucifera (coconut) oil, and boric acid as its main active ingredients. Sea buckthorn oil, with its saturated and unsaturated fatty acids, improves skin hydration. The omega fatty acids and oleic acid derivatives of their content reduce skin fluid loss. 15 Furthermore, the fatty acids in their content exhibit strong antioxidant properties. 16 In 2012, Hwang et al. demonstrated that sea buckthorn extract regulates moisture content, matrix metalloproteinase activity, and superoxide dismutase activity, causing the aging of the skin. 17 The antioxidant effect of sea buckthorn is observed not only in keratinocytes but also in fibroblasts, thus affecting the most important cells for wound healing. 18
Coconut oil in its composition has been shown to have anti-inflammatory and antimicrobial effects along with its moisturizing effect. 19 Furthermore, coconut oil has been reported to increase the number and lifespan of dermal fibroblast cells in cell culture studies. 20 Another ingredient in the content is boric acid, which lowers the pH of the environment and thus exhibits antiseptic, antifungal, and antibacterial properties. Furthermore, the positive effects of boric acid on wound healing have been reported on angiogenesis, collagen synthesis, and reepithelialization. 21
After parotidectomy, the quality of life of patients is typically assessed using the Parotidectomy Outcome Inventory-8 (POI-8) scale. 22 This evaluation method involves questions about pain in the surgical area, sensory problems, incision scar, weakness in facial muscles due to facial paralysis or paresis, formation of a deformity in the parotidectomy region due to loss of parotid volume, presence of Frey syndrome symptoms, appearance of dry mouth, and concerns about the possibility of revision surgery. However, in our study, because malignant patients were not included, standard surgical methods were used to prevent the development of Frey syndrome and the prevention of dry mouth by surgically removing the superficial lobe and preserving the deep lobe, the modified version of the POI-8 scale was used to evaluate isolated skin outcomes of the parotidectomy procedure.
The primary assessment method in this study is to evaluate the effects of epidermos barrier cream on postoperative incision scars. For this purpose, the patient was asked to score the scar from 1 to 6 to assess how the patient perceived the scar on the surgical site. Similar methods have been observed in the literature for scar evaluation. Gao and colleagues evaluated the incision scar in 3 stages: satisfactory, mild satisfactory, and unsatisfactory. 23 In our evaluation, we considered 1 to 2 points as good scar healing, 3 to 4 points as moderate scar healing, and 5 to 6 points as poor scar healing.
In the study, the evaluation form also includes asking about loss of sensation. The Magnus auricularis nerve runs just below the skin during the incision used for parotidectomy and can be easily injured during the incision. Preservation of the posterior branch of this nerve is crucial to maintaining sensation in the auricular region, which significantly affects quality of life. 24 Another symptom evaluated postoperatively in the study was pain in the operation area. Postoperative pain after parotidectomy has been reported in the range of 8% to 25%. 25 Another finding evaluated postoperatively in the study is the inflammatory reactions observed at the edges of the wound. Local inflammation, often reported along with hypoesthesia, is a common minor complication. 26 In our study, while no differences were observed between the groups in terms of hyperemia in the first week of the study, a statistically-significant difference in hyperemia between the groups was observed in the second week. This suggests the potential effect of an epidermos barrier cream on the early-inflammatory response. Closure of the wound and reduction in the inflammatory response likely constitute crucial steps in reducing scar formation in the long term.
In the literature, especially good or very good surgical results have been reported cosmetically after parotidectomy performed for benign tumors. 27 In this study, patients with benign parotid masses were included. Patients requiring intervention in the deep lobe or additional postoperative treatment that could affect wound healing were not included in the study. The rate of patient discomfort due to the incision scar after parotidectomy has been reported as 32.4% in previous studies. 28 In our study, we also determined this rate as 30.4% similar to the literature. Most of these patients are in the control group, and the normal healing process of this surgery may form a level of healing tissue that disturbs the patients.
The basic mechanisms of epidermos barrier cream in wound healing are believed to involve reducing mechanical stress at the edges of the wound and decreasing pro-inflammatory and profibrotic mechanisms during wound healing. Therefore, epidermos is considered an optimal wound care product, both for covering and protecting the wound and for its anti-inflammatory and antifibrotic properties. These hypotheses must be supported by further histopathological studies.
Strong points of the study: All surgeries were performed by the same surgeons using the same method. All patients were followed in a similar way as its normal way. The parotidectomy scar was evaluated by both the patient and the surgeon. The findings of both were concordant.
Weakness: The results and hypotheses obtained in the study should be supported by histopathological findings.
Conclusion
In this study, the modified Blair incision used for superficial parotidectomy and its healing period were evaluated. The use of postoperative epidermos barrier cream led to improved scar healing at the surgical site. More studies can be planned in larger populations and must be supported by histopathological findings. With these findings, epidermos barrier cream can be used to heal normal wounds, as well as in cases where the wound site is complex and the healing process can create significant scarring.
Footnotes
Acknowledgements
This study is own work of authors.
Author Contributions
Ozan Gokdogan, Ömer faruk Güzel, Mahmut Demirtaş, Sabri Koseoglu, and Harun Üçüncü have played role in data collection, analysis, and in the writing of the paper. Fulden Cantaş Turkiş has played role in data evaluation, analysis, and in the writing of paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study received approval from the Mugla Sitki Kocman University Clinical Research Ethics Committee with number 9/X and the date of April 13, 2023. Subsequently, approval was obtained from the Turkey Medicines and Medical Device Agency Ethics Committee of the Turkish Ministry of Health with the number E-68869993-511.06.01.02-1189653 and the date of August 11, 2023.