
Abstract
Introduction
Childhood obesity has become an increasing health care concern in the United States with approximately 20% of children affected. 1 Obesity has been linked to several diseases in the pediatric population including sleep disordered breathing, obstructive sleep apnea (OSA), hypertension, diabetes mellitus type II, and reactive airway disease.2,3 It has been recognized to be both a risk factor and a disease modifier for asthma in children. 4
Asthma and chronic rhinosinusitis (CRS) frequently coexist. The unified airway theory based on the epidemiological link between CRS and asthma has been confirmed by pathophysiologic and therapeutic observations. 5 Similarities in the histopathological composition between the nasal mucosa and the bronchial mucosa have been seen in children with CRS, allergic rhinitis (AR), and asthma. 6
Obesity has been associated with CRS in adults; however, studies exploring this association in children are limited. A recent systematic review with meta-analysis identified only 1 study that explored that association in children. 7 A large population-based study by Sidell et al found no association between childhood obesity and CRS or AR. 8 The limitations with this study are related to the diagnoses of CRS made based on ICD-10 codes, which may not be accurate, and the lack of control for comorbidities such as asthma and OSA. Therefore, more studies are needed to confirm the presence or absence of association between obesity and CRS.
The objective of this study was to evaluate the association between obesity and the unified airway, namely CRS and asthma in children while controlling for comorbidities.
Materials and Methods
This is a cross-sectional study of all pediatric patients (age 18 years and younger) presenting to West Virginia University Otolaryngology clinic between July 2020 and February 2024. Inclusion criteria were age 2 to 18 years and diagnosis of CRS as defined by the clinical presentation and the presence of objective evidence of disease on CT scan or through direct endoscopic visualization. 9 Endoscopic evidence of CRS includes the presence of nasal polyps, mucosal edema, or purulent drainage, which were scored according to the modified Lund-Kennedy scoring system.10,11 CT scans were scored according to the Lund-Mackay scoring system (0-2 for each of the maxillary, ethmoid, frontal, and sphenoid sinuses, and the osteomeatal complex). 12 Patients selected for the study were then stratified based on body mass index (BMI). The obese group was classified as patients with a BMI at or above the 95th percentile in accordance with the Centers for Disease Control BMI-for-age growth chart. 13 Chart review was performed to collect data including demographics and comorbid conditions. OSA was diagnosed based on a polysomnography, AR based on positive skin or blood testing, and asthma based on published guidelines Global Initiative for Asthma guideline.
Univariate analyses and multivariate binary logistic regression model were used to compare differences between obesity and nonobesity groups. Analyses were carried out using Stata 18 with 2-tailed P-value set at .05.
Results
A total of 406 pediatric patients met criteria, with 130 children (32%) with obesity. The mean age for the cohort was 10.5 years (SD of 4.9) with 42.2% of them being 12 to 18 years (adolescents), and 44.5% were female. Children with CRS (N = 131) had a mean CT Lund-Mackay score of 7.2 (SD of 6.3, N = 63) and a mean endoscopy modified Lund-Kennedy score of 2.7 (SD of 2.9, N = 81). Table 1 shows patients’ characteristics and univariate analysis comparing children with and without obesity. Children with obesity were older (11.3 years vs 10.2 years, P = .039) and more likely to have asthma (28.5% vs 15.2%, P = .002) and OSA (26.2% vs 13%, P = .001). Figure 1 shows the multivariate logistic regression analysis. It shows an association between obesity and asthma (OR = 1.84, P = .029), but not with CRS (OR = 1.08, P = .856) or AR (OR = 1.05, P = .856).
Univariate Analysis and Comparison Between Children With and Without Obesity.

Abbreviations: BMI, body mass index; CRS, chronic rhinosinusitis; OSA, obstructive sleep apnea.
Values in bold denotes statistical significance.
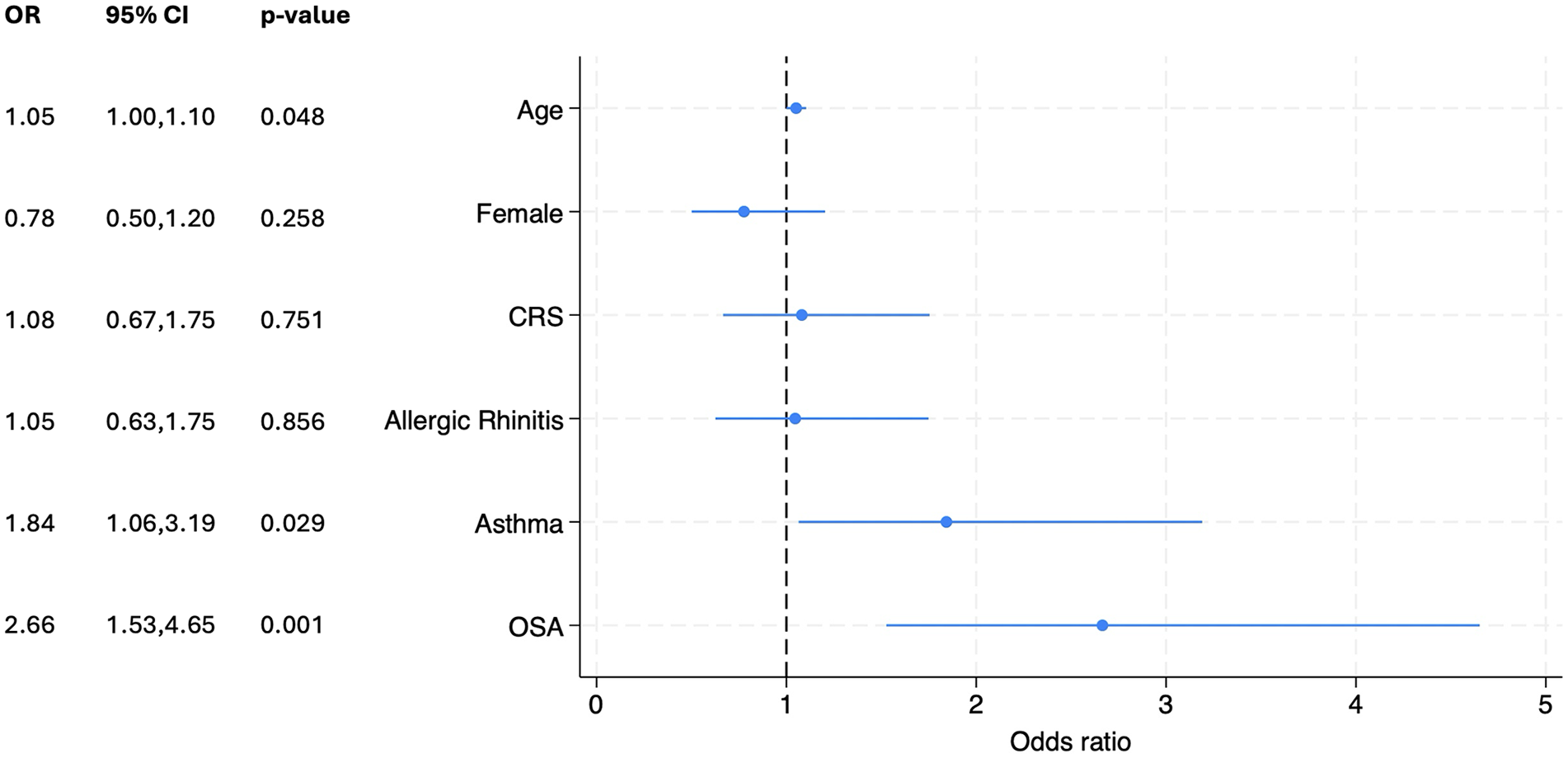
Coefficient plot showing the multivariate logistic regression analysis for the association of obesity with chronic rhinosinusitis (CRS), asthma, and allergic rhinitis after adjusting for age, sex, and comorbidities. Positive association was found between asthma and obesity, but no association was found with CRS or allergic rhinitis.
Discussion
Obesity has become an increasing public health issue, and it is therefore important to know the comorbidities that are associated with the disease. While obesity has been found to be associated with CRS in adults in a number of studies, there is limited research on this subject in the pediatric population.7,14 In 2013, Sidell et al performed a cross-sectional analysis of school-aged children from 2006 to 2008 utilizing the Medical Expenditure Panel Survey to identify 42.1 million patients with acute otitis media, AR, and CRS. 8 While they found a significant association between otitis media and childhood obesity, there was no association between childhood obesity and CRS. Our study corroborates these findings.
While population-based studies are ideal to identify associations with small effect size due to the large sample size they provide, they also have limitations. First, it is difficult to control for comorbidities, which are often not included in the databases, and second, the diagnoses are based on current procedural terminology (CPT) codes and may not always be accurate. Our study has several advantages. It controls for comorbidities such as age and OSA; all the diagnoses included were based on published guidelines, including CRS that was confirmed by objective findings on CT scan or nasal endoscopy; it included children of all ages (2-18 years), which helps increase generalizability of the results to all the pediatric population.
Our study also found an association between obesity with asthma. This association is well documented in prior literature.4,15 These findings validate our results. Also, there is evidence that the presence of asthma is associated with a worse CRS severity and outcome in children. 16 One prior study has shown that the inflammatory markers in children with CRS are amplified in the setting of asthma. 5 Although obesity is associated with asthma, this association does not extend to CRS. Therefore, future research should investigate the pathophysiological mechanism of how obesity affects the lower airway selectively. Also, future research should investigate whether obesity affects treatment outcome in pediatric CRS.
The difference in the obesity and CRS findings between adults and children is intriguing. While the association between obesity and CRS has been consistently documented in adults, it is unknown why this is different in children. One possibility can be related to the differences in the endotypes and inflammatory markers between adult and pediatric CRS. Leptin, which is a hormone that is increased in obesity, is involved in increasing the production of proinflammatory cytokines such as tumor necrosis factor-α, IL-6, and IL-12, which may play a role in obesity-associated respiratory disease. 17 Further research is needed to evaluate these differences.
There are several limitations to our study. First, it is a retrospective observational study, which has inherent limitations including drawing conclusions regarding causality. Second, the sample size may not be large enough to detect a small association that may be present.
Conclusion
Although obesity is associated with asthma in the pediatric population, it was not associated with CRS. Further investigation is needed to explain how obesity selectively affects the lower airway without affecting the upper airway.
Footnotes
Acknowledgements
None.
Data Availability Statement
Data from the study are available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The study was approved by WVU IRB #2004956868.
Informed Consent/Patient Consent
Not applicable.
Trial Registration Number
Not applicable.