
Abstract
Kaposi’s sarcoma (KS) is a tumor involving blood vessels and lymphatic tissue. It is caused by human herpes virus-8, typically in HIV infection in individuals with AIDS. There are 4 major types of KS including classic, endemic, immunosuppression, and AIDS-related. Endemic KS is unique among the different types as it is associated with patients with HIV-seronegative and can present either as an indolent tumor or as a fast-growing mass. The authors discuss a unique presentation of metastatic, endemic KS in a patient with HIV-negative, non-immunosuppression, which has yet to be described in the United States. A 38-year-old male with a history of same-sex partners, presented with a new oral lesion that had appeared 6 weeks ago. He was negative for human papillomavirus or HIV infection. A computed tomography (CT) scan demonstrated destructive lesions of the hard palate. The specimens obtained from biopsy were consistent with endemic KS. A Positron Emission Tomography – computed tomography (PET-CT) scan showed widely-metastatic disease. Case reports have described a rare subtype of HIV-seronegative KS in men who have sex with men. However, these are typically-indolent tumors with exclusively-cutaneous manifestation. This is a unique case of aggressive, widely-metastatic endemic KS metastatic in a patient with HIV-negative.
Introduction
Kaposi sarcoma (KS) was first described by Moriz Kaposi, a Hungarian dermatologist, in 1872. It is a tumor that affects blood vessels and lymphatic tissue and is caused by human herpes virus-8 (HHV-8), usually in combination with an immunocompromised state. 1 KS has the potential to manifest itself in multiple areas of localization, including the lower extremities, facial skin, and oropharyngeal mucosa. 2 KS with a primary lesion at the cutaneous or mucosal head and neck sites is rare. 3 When KS is multifocal, it is commonly associated with human immunodeficiency virus (HIV) infection in individuals with acquired immunodeficiency syndrome (AIDS). 4
There are 4 main types of KS, including classic, African/endemic, immunosuppression, and AIDS-related.1,5 AIDS-related is the most common form of KS. Endemic KS is unique among the different types as it is associated with patients with HIV-seronegative, can present as either an indolent tumor or as a rapidly-growing mass, and can present in the third or fourth decade of life. 5 The authors discuss a unique presentation of metastatic endemic KS in a patient with HIV-negative, non-immunosuppression, which has yet to be described in the United States.
Case History
The authors present a 38-year-old male with a history of obesity, asthma, gout, and septic arthritis, presented with a new oral lesion that had developed within the last 6 weeks. The patient had never noticed the lesion, and there was no mention of such a large intraoral lesion by anesthesia when he was in the hospital for the treatment of his septic arthritis with arthroscopy just 2 months earlier (Figure 1).

Bilateral oral cavity lesions of the hard palate with left-sided lesion larger than the right-sided lesion.
He first noticed a lump on the left upper gingiva, which had been growing consistently per patient. He presented to the Otolaryngology—Head & Neck Clinic after noticing new growths in the bilateral superior oral mucosa and the left posteroinferior gingiva. He denied any associated fever, chills, or unexplained weight loss, but endorsed new night sweats. He had a history of tobacco use and no alcohol use. He had no known exposure to human papillomavirus (HPV) or HIV. He had not received the HPV vaccine. He had no history of transplant surgery and denied any family history of head and neck cancer. The patient did endorse a history of same sex partners with consistent condom use.
Oral lesion biopsies were obtained in the clinic as part of the next step in the evaluation of this patient. These outpatient specimens were diagnostically inconclusive. Radiographic studies with maxillofacial computed tomography (CT) demonstrated destructive lesions of the left maxilla extending laterally into the gingiva and posteriorly into the lingual surface of the mandible measuring 3 cm and a second lesion involving the lateral surface of the mandible measuring 1.5 cm. There was also destruction of the hard palate as well as bilateral lymphadenopathy. Magnetic resonance imaging was also obtained that confirmed the CT findings. With radiographic images showing a destructive process and outpatient biopsies unable to provide a diagnosis, the patient was scheduled for an operative biopsy.
The operative biopsies were sent for evaluation by a head and neck pathologist at an outside institute. The specimens sent for review were found to include slit-like vascular channels (Figure 2A), as well as large, more dilated vascular spaces with irregular staghorn growth. The neoplasm was also characterized by the presence of squamous mucosa showing submucosal multinodular spindle cell proliferation with fascicular growth of cells with elongated nuclei with indistinct borders and lightly-eosinophilic cytoplasm (Figure 2B). The immunohistochemistry (IHC) stained slides showed that the neoplastic cells were positive for CD31 (Figure 2C), CD34, ERG, D2-40, and HHV-8 (Figure 2D), but negative for cytokeratins. The specimens sent were consistent with the endemic KS, given the patient’s HIV-negative status and the absence of immunosuppressive sources such as transplant medications. A Positron Emission Tomography – computed tomography (PET-CT) scan showed hypermetabolic retropharyngeal adenopathy noted to be greater on the left than the right. Multiple small, but focally-hypermetabolic cervical nodes seen in levels 1 to 4 bilaterally. Additionally, there was hypermetabolic adenopathy involving nodes below the diaphragm bilaterally, as well as hypermetabolic osseous lesions corresponding with subtle sclerosis on CT, concerning for osseous metastases. The results of the PET-CT were consistent with metastatic stage IV disease. After discussion at head and neck tumor board, the patient was started on palliative doxorubicin.
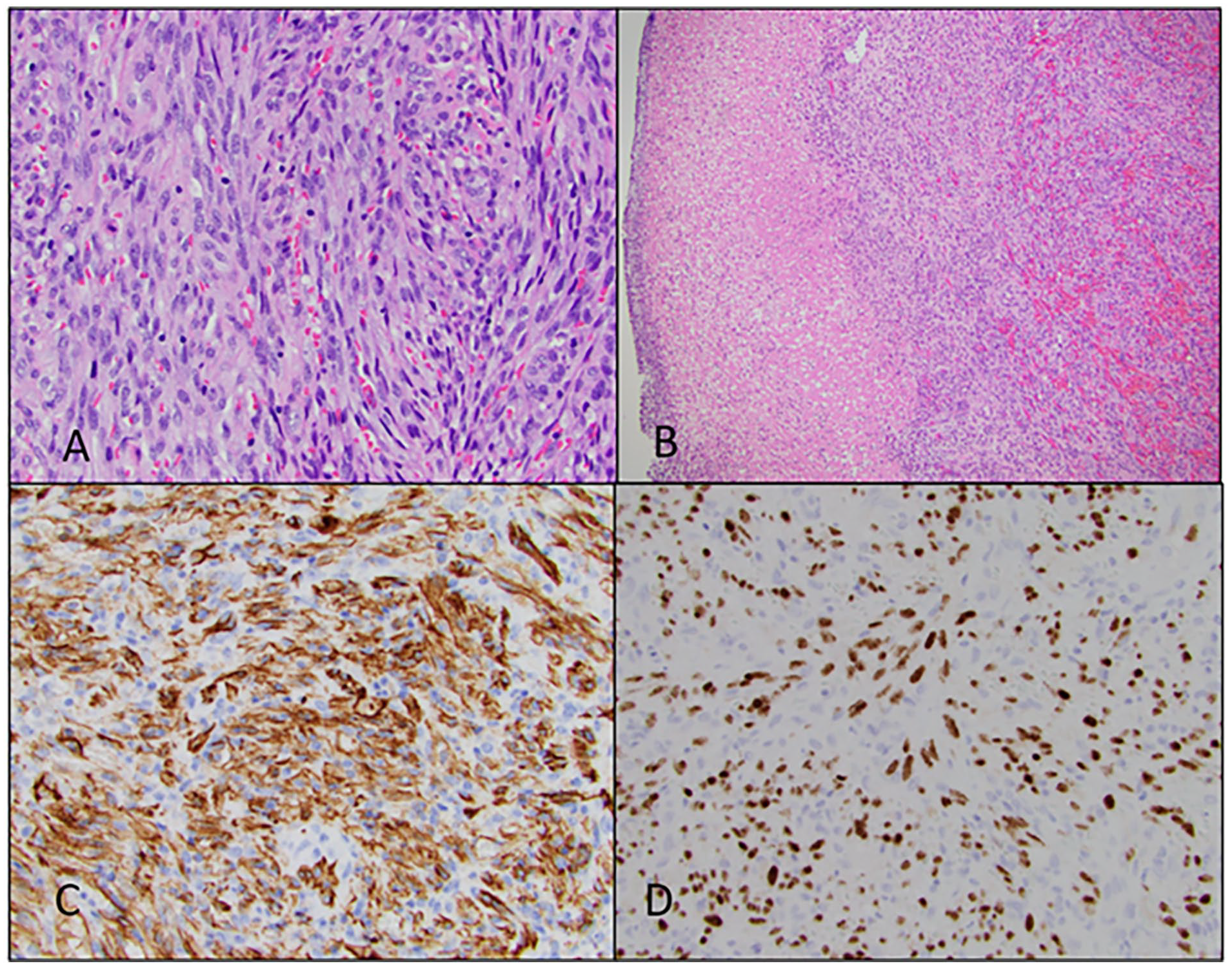
(A) H&E, 40×, fascicles of spindle cells with slit-like spaces containing extravasated red cells and eosinophilic globules. (B) H&E, 10×, superficial ulceration with underlying spindle cell proliferation with extravasated red cells. (C) CD31 IHC stain, strong cytoplasmic immunoreactivity for CD31. (D) HHV-8 IHC stain, diffuse, strong nuclear immunoreactivity for HHV-8. HHV-8, human herpes virus-8; IHC, immunohistochemistry.
Discussion
KS is a vascular tumor that appears as violaceous patches, plaques, and nodules. KS has a broad clinicopathological variation that is influenced by location of lesions, clinical appearance of the lesions, and epidemiological classification. 6 This applies to AIDS-related KS, classic KS in older males, endemic KS in younger men and children from central Africa, and iatrogenic KS affecting transplant patients or the immunosuppressed.5,6 One of the studies on viral spread of HHV-8 indicates that it is spread by horizontal transmission through an oral route, which is supported by high rates of viral shedding in the saliva of infected individuals. 7 The clinicopathological behavior of KS can be greatly affected by the subtype of the lesion. Classic KS typically presents in elderly males (60-70 years) of Mediterranean, eastern European or South American descent with indolent cutaneous tumors on the lower extremities. Occasionally, it may involve the gastrointestinal (GI) tract or lymph nodes. Iatrogenic or immunosuppression-induced KS presents with cutaneous or GI tumors, which may be indolent or aggressive with risk of GI hemorrhage. AIDS-related KS presents with multifocal cutaneous lesions with mucosal and visceral involvement. This subtype is particularly prone to rapid progression, which requires immediate highly-active antiretroviral therapy for reversal. 8 The endemic form affects young, middle-aged sub-Saharan African males or children with benign nodular lesions. The endemic subtype has a higher risk of invasion into soft tissue, bone, visceral organs, or disseminated lymphadenopathy. Since the 1980s, case reports have described a rare subtype of HIV-seronegative KS in men who have sex with men, which may represent a new subclassification called nonepidemic KS.8,9 This group includes middle-aged individuals without AIDS. Clinical presentation resembles classic KS, with cutaneous involvement of the lower extremities, trunk, and genitals and an indolent course such as classic KS. However, these are typically-indolent tumors with exclusively-cutaneous manifestation and rare mucocutaneous involvement (1 case on the buccal mucosa). 8
Determining whether a cutaneous lesion is consistent with KS rather than another benign or infectious vasoproliferative tumor can be challenging. Biopsy of the lesion for histopathology and IHC staining remains the gold standard for diagnosis. Patch or the early stage is characterized by a proliferation of small, irregular blood vessels, a lymphocytic infiltrate, and spindle cells. There may be extravasated blood vessels seen as well. In the plaque or intermediate stage, all the findings present in the patch stage are amplified and exaggerated. The nodular or late stage involves intersecting sheets and fascicles of spindle cells forming slit-like vascular spaces. Areas of necrosis and extravasated blood vessels may be present as well. 10 This patient’s KS lesion presented as an erythematous mucosal lesion on the hard palate that was locally destructive. The lesion histopathological characteristics were similar to other KS lesions being composed of fascicles of spindle cells with elongated nuclei, faintly-eosinophilic cytoplasm, and slit-like vascular spaces.1,3,11 Spindle-shaped cells are present in all forms of KS. This finding is a unifying feature and form the basis for diagnosis. 6 For the patient being presented, IHC staining of the specimens had consistent coexpression of CD31 and CD34 endothelial markers of vascular origin, as well as ERG, CD34, D2-40, and HHV-8. The patient was also positive for KS latency-associated nuclear antigen, which is the deciding diagnostic marker for KS and contributes to the identification of HHV-8 within KS lesions.6,9,11
KS of the head and neck is uncommon, but due to the rarity of sarcomas in this region, KS represents 20% to 25% of head and neck sarcomas. 3 Non-AIDS-related head and neck KS lesions have a propensity for the hard palate and the oropharynx. 10 This is due to the oral cavity being the site of the most viral shedding, as horizontal transmission through saliva is how the virus spreads. Reports of oral cavity endemic KS are scarce and classic KS with oral involvement only 5% were seen in patients with HIV-negative. 10 The case presented above fits a picture of an incredibly-rare oral mucosal lesion of endemic KS and serves to illustrate how difficult it can be to diagnose KS of the head and neck without a broad differential. When working up the oral cavity lesion, it is important to first make sure it is not a carcinoma, especially in patients with HIV-positive status, history of organ transplantation, or immunosuppression status. Bacillary angiomatosis, a rare AIDS-associated vasoproliferative lesion, must also be ruled out as it can mimic KS. This is carried out with demonstration of the causative microorganism, Bartonella henselae, with the Warthin-Starry stain.
Treatment for KS in patient with HIV-negative involves local excision, radiotherapy, and chemotherapy either single agent or combination. Radiotherapy is often an effective management strategy as this is a radiosensitive lesion. 2 Cutaneous tumors may be treated with intralesional chemotherapy, such as imiquod or allotretinoin gel. Treatment of metastatic disease requires single agent chemotherapy with either bleomycin, vinblastine, or an anthracycline. Other systemic options include all transretinoic acid, bevacizumab, sirolimus, or immunotherapy with interferon-α or immune checkpoint inhibitors; however, response rates for systemic treatment are generally low. 12 The patient was started on doxorubicin chemotherapeutic agent for a widely-disseminated disease with metastasis to the lymph nodes and bone.
Conclusion
There are several subtypes of KS and is often associated with HIV infection or immunosuppression. These subtypes are classic, African/endemic, immunosuppression, and AIDS-related. Each of these subtypes has a slightly-different way in which it presents and in different populations. KS of the head and neck is uncommon but has a propensity for the oropharynx and the hard palate of the oral cavity. While cases of HIV-negative classic KS are rare, they have been reported on. HIV-negative patients with endemic subtype of KS are incredibly uncommon and are not well reported. This is a unique case of aggressive, widely-metastatic oral cavity endemic KS in a patient with HIV-negative. This uncommon pathology merits documentation so that it can be added to our understanding of this disease.
Footnotes
Acknowledgements
There are no acknowledgments for this case report.
Authors’ Note
This case report was conducted in accordance with Lehigh Valley Health Network IRB standards and regulations.
Author Contributions
S.H.S.: primary author, literature review, and editor. M.M.: secondary author and literature review. C.S.N: principal investigator.
Data Availability
There are no data associated with this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This case report was conducted in accordance with IRB procedures and protocols.
Informed Consent
Written informed consent was obtained as part of this case report.
Trial Registration
Trial registration was not required for this case report.