
Abstract

Significance Statement
Autosomal recessive osteopetrosis (ARO) is a rare inherited disease characterized by insufficient osteoclast activity, increased bone formation, leading to obstructive sleep apnea (OSA). The literature is limited to patients treated with adenotonsillectomy and/or tracheostomy. We report the first case of OSA in ARO treated with targeted surgery to relieve nasal airway obstruction and avert the need for tracheostomy, with marked and sustained clinical, radiographical, and physiological improvement in OSA metrics, up to 4 years post-op.
Autosomal recessive osteopetrosis (ARO), also known as “marble bone disease,” is a rare hereditary condition characterized by insufficient osteoclast activity causing defective bone resorption, a marked increase in bone mass, and defective bone marrow. 1 Overgrowth of the skull base foramina causes hydrocephalus and cranial nerve compression and resulting blindness, deafness, nystagmus, and facial nerve paralysis.2-4 Other symptoms may include seizures secondary to hypocalcemia, abnormal midface anatomy, micrognathia, small thorax, anemia, thrombocytopenia, immunodeficiency, and hepatosplenomegaly secondary to extramedullary hematopoiesis. 5 Obstructive sleep apnea (OSA) is one of the potentially-life-threatening conditions commonly encountered in these patients. 6 The available literature on the management of OSA in this population is limited to reports of adenotonsillectomy followed by tracheostomy. Here, we present a case of severe OSA in a patient with ARO, where the need for tracheostomy was averted through targeted surgery to alleviate nasal obstruction.
A 7-year-old female, diagnosed with ARO at the age of 18 months, was referred to the pediatric otolaryngology service after recent immigration. She presented with longstanding nasal obstruction, rhinorrhea, loud snoring at night, frequent witnessed apneas, and increased respiratory effort. Nasopharyngoscopy demonstrated abundant nasal secretions bilaterally and inability to pass a 2.2 mm flexible nasolaryngoscope beyond the posterior aspect of the inferior turbinate on either side. There was no tonsillar hypertrophy or micrognathia.
Computed tomography of the sinuses confirmed nasopharyngeal airway obstruction due to hyperostosis of the vomer: The coronal diameter of the bony choana measured approximately 2 mm on each side (Figure 1). There was no significant adenoid hypertrophy.

This figure presents preoperative computed tomography images with representative axial (A), coronal (B), and sagittal (C) views. Hyperostosis of the vomer and resulting nasopharyngeal obstruction are indicated by red arrows.
A nocturnal home pulse oximetry suggested severe OSA with McGill Oximetry Score (MOS) of 4, markedly-abnormal 4% desaturation index (4%DI) of 113.8 events/hour, several clusters of desaturations, and significant pulse rate variability. For several medical and social reasons, this patient was not a candidate for stem cell transplant at the time. She was taken to the operating room for endoscopic management of nasal obstruction.
A posterior septectomy was performed via endoscopic transseptal approach through a left-sided Killian incision. The vomer was hypertrophic and hyperostotic, extending into and obstructing the superior nasopharynx. The hyperostotic bone was removed with a combination of endoscopic drill and nonpowered instrumentation. The removal of the pathological bone created a widely-patent nasopharyngeal airway, as seen endonasally.
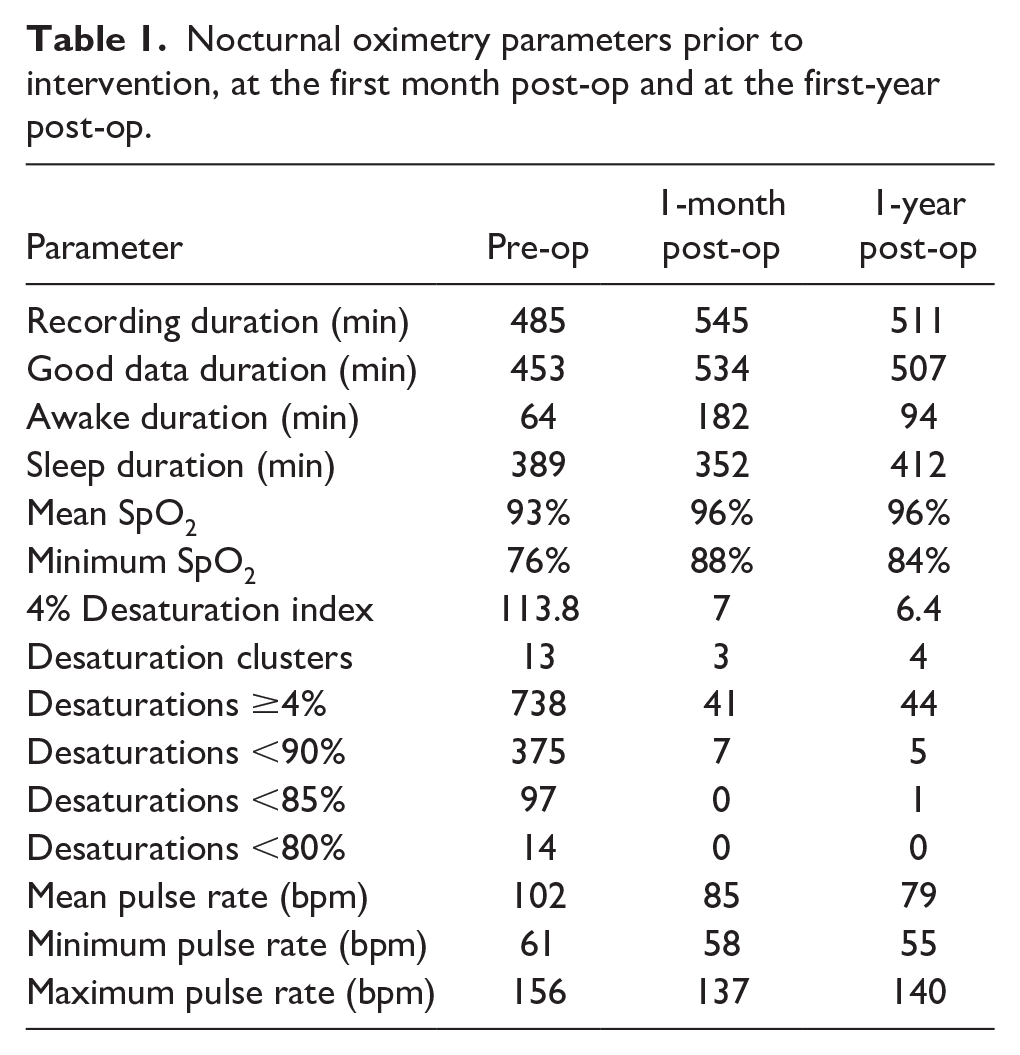
Postoperative oximetry performed at the 4th week demonstrated a marked improvement. The 4%DI decreased to 7.0 events/hour (from 113.8) (Table 1). These improvements were maintained at the first1 year follow-up (4%DI 6.4 events/hour). Clinically, the parents noted a marked symptom improvement, with resolution of snoring, labored breathing, nasal obstruction, and rhinorrhea. Clinical and radiological improvement persisted at up to 4 years post-op (Figure 2).
Nocturnal oximetry parameters prior to intervention, at the first month post-op and at the first-year post-op.

Representative axial computed tomography image at the 2nd year post-op, demonstrating stability in nasopharyngeal airway patency.
ARO is a rare hereditary disease with genetic and clinical heterogeneity. These patients have multifactorial etiology for the development of OSA due to the narrowing of the pharyngeal lumen from bony overgrowth, adenotonsillar hypertrophy, and/or micrognathia from disordered bone overgrowth. 5 Stocks et al. described the otolaryngologic manifestations of ARO, and reported OSA in 5 out of 9 (56%) cases, 3 of whom required tracheostomy. 6 There is no previous report of endoscopic repair or its efficacy. 5 Avoiding a tracheostomy in a complex pediatric patient is of critical importance for patient and caregiver quality of life. Our case demonstrates that targeted alleviation of airway obstruction may be an effective method for the treatment of OSA in patients with ARO and may preclude the need for tracheostomy in carefully-selected patients.
This case also highlighted the utility of at-home nocturnal pulse oximetry and the MOS in the diagnosis and surveillance of patients with OSA. At our institution, home oximetry provided valuable diagnostic information, expedited the treatment of this patient, helped guided perioperative care in a setting where access to polysomnography is limited.7,8 This patient’s MOS improved from MOS4 to MOS1 after intervention, aknowledging that the MOS was initially validated only in healthy children. Perhaps more indicatively, the 4%DI reduced significantly, from 113.8 to ~7 events/hour. Polysomnography will be required to further characterize the etiology of these residual desaturations and differentiate obstructive versus central events. Though, when clinical improvement is observed and residual OSA is mild, recent expert consensus suggested observation to be a reasonable option in patients with high medical complexity and/or perioperative risk. 9
This clinical vignette demonstrates the efficacy of targeted alleviation of airway obstruction for the treatment of OSA in ARO. Targeted interventions should be considered in carefully-selected ARO patients with OSA and may preclude the need for tracheostomy.
Footnotes
Acknowledgements
None.
Author Contributions
S.M.: chart and literature review, manuscript drafting, and final approval. E.C.: performance and monitoring of sleep parameters, interpretation and verification of oximetry data, and manuscript review and final approval. R.T.B.: performance and monitoring of sleep parameters, interpretation and verification of oximetry data, and manuscript review and final approval. J.C.Y.: chart and literature review, manuscript drafting and final approval.
Data Availability Statement
Not applicable for case reports.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics
Not applicable for case reports.
Informed Consent/Patient Consent
Written informed consent was obtained from the patient’s legally-authorized representative.
Trial Registration Number
Not applicable.
Grant Number
Not applicable.