
Abstract

Significance Statement
This case highlights the diagnostic challenges of intraosseous lipomas of skull base, rare lesions often discovered incidentally, presenting with generalized symptoms, such as headache, or site-specific complaints. Emphasizing the role of diagnostic imaging, it underscores the need for accurate radiologic interpretation to differentiate this benign entity from more sinister pathologies, guiding appropriate management and avoiding unnecessary workup or biopsies.
Case Presentation
A 30-year-old female without significant past medical history presented with a 6 month history of intermittent, nonspecific headache, occasionally more prominent at the vertex. She denied any visual disturbances, nausea, vomiting, specific triggers, or other neurological symptoms. Over the past 2 years, her entourage had noted mild cognitive decline including slowed response times and difficulty focusing on tasks. She had not been personally concerned by these changes until the recent onset of headaches. She reported no rhinological symptoms.
Physical examination was unremarkable, with no focal deficits observed. The mental status examination revealed notable psychomotor slowing, with the patient exhibiting a slower response to questions and a mild cognitive difficulty, particularly with tasks involving short-term recall. Magnetic resonance imaging (MRI) revealed a left-sided lesion of sphenoclival area, protruding into the left sphenoidal sinus and extending to the pterygoid process (Figure 1). Computed tomography scan demonstrated thin bony septa within the lesion and a mean density consistent with fat, thereby confirming the diagnosis of intraosseous lipoma (IOL) (Figure 2).
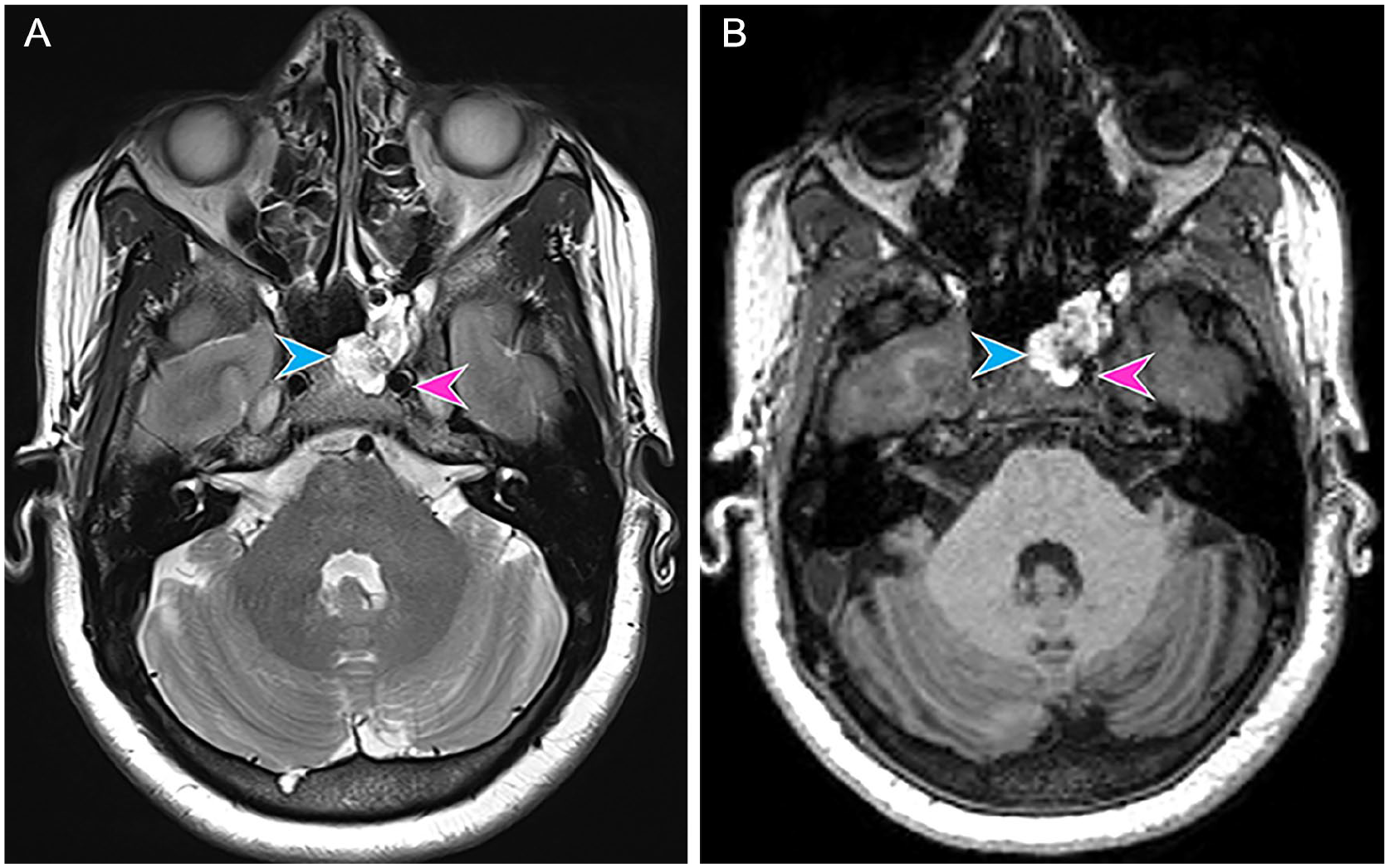
Magnetic resonance imaging sequences. Axial T2-weighted (A) and unenhanced T1-weighted (B) sequences demonstrate a left sphenoclival lesion, located anteriorly and medially to the left internal carotid artery (pink arrowheads), appearing well-delineated by a thin hypointense rim with a hyperintense center on T2-weighted and T1-weighted sequences (blue arrowheads).

Computed tomography image. An unenhanced axial computed tomography image displays a lesion located anteriorly to the internal carotid artery (pink arrowhead) containing thin bony septa (orange arrowhead) with a hypodense center (blue arrowhead) and a mean density of –85 Hounsfield units, corresponding to fat.
Discussion
A benign tumor, IOL refers to a histological variant of typical lipoma and is widely reported to represent less than 0.1% of all primary bone neoplasms. 1 However, due to underreporting, its asymptomatic and incidental nature and misdiagnosis during radiologic interpretation, the true incidence is estimated between 1% and 8%. 1 It most commonly affects the long bones of the lower limb and calcaneous and therefore predominates the orthopedic literature. 1 There are isolated case reports involving skull bones including frontal, temporal, parietal, sphenoid, and ethmoid bone.1,2 Histopathologically, IOL can be identified by the early resorption of trabecular bone and the presence of fat. 1
According to the orthopedic literature, the average age of patients with IOL is 37 years. 1 Clinical presentation of IOL can range from being asymptomatic and discovered incidentally to manifesting generalized such as headache, and site-specific symptoms including nasal congestion, visual impairment, blepharoptosis, cosmetic deformity, and hypopituitarism due to expansion within the sphenoid bone and resultant mass effect.1,3
Milgram established a staging system for IOL, which evaluates the ratio of viable to necrotic fat cells within the lesion. 4 Propeck and colleagues subsequently correlated histopathology with radiologic features of the lesion in various modalities, improving both diagnostic frequency and accuracy. 5 An early-stage IOL presents resorption of trabecular bone and fat attenuation on computed tomography and isointense signal to subcutaneous fat on T1 sequences.1,4,5 Advanced stage IOL, consisting of a central area of fat necrosis, is typically the most difficult to distinguish from other osseous lesions given the similarity in radiologic appearance to bone infarct.1,5 However, resorption of trabecular bone, peripheral rim of discernable fat and central calcification on computed tomography combined with rather high signal intensity in center and low signal intensity rim will help accurate diagnosis.1,5
Cortical bone thinning and loss and trabecular bone destruction, radiologic features typically associated with aggressive expansile pathology, when observed within the skull bones may not indicate a sinister lesion. 1 Bone remodeling is more common in IOL of the skull than long bones, a feature associated with advanced stage lesion according to Milgram. 1 Thus, applying this classification to lesions of the skull bones is more challenging. 1 The spectrum of differential diagnosis of fat-containing lesion encompasses intraosseous hemangioma, arrested pneumatization, and hamartoma.1,6
Computed tomography alone is adequate to pose the diagnosis of IOL when the suspected lesion displays bony remodeling and fat content. 1 A measured attenuation inferior to 5 Hounsfield units is almost pathognomic for a fatty benign lesion. 1 In cases where diagnosis remains uncertain, MRI can be utilized to further characterize the lesion. Intraosseous hemangioma refers to an expansile lesion that may contain fat, with a lacelike pattern of bone trabeculae and displays prominent enhancement. 1 Arrested pneumatization is a benign anatomic variant most commonly encountered at a site of normal or accessory sphenoid sinus pneumatization.7,8 If the full constellation of findings, including thin sclerotic margins, internal fatty content, and curvilinear internal calcifications, are present, a confident diagnosis can be made.7,8
Regarding non-fat-containing benign lesions, fibrous dysplasia, chondroid lesions such as chondrosarcoma or chondroid chordoma, and advanced stage IOL should be considered part of the differential, as advanced fat necrosis with very few viable fat cells present is a feature of more aggressive pathology as well as stage 3 IOL. 1 Chondrosarcoma is a slow-growing, destructive, and expansile lesion presenting an internal amorphous or stippled chondroid pattern of calcification associated with moderate to marked enhancement.1,6
Awareness of imaging features can facilitate accurate diagnosis and reduce the need for extensive workup or surgery.
Footnotes
Consent to Participate
Written informed consent was obtained from participant included in the report.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.