
Abstract
Keywords
Introduction
Singers, both professional and non-professional, attend the Otorhinolaryngology and Head-Neck Surgery (ORL-HNS) clinic with complaints related to their voice quality, like inability to attain high notes, recent loss of melody, and easy fatigability. Often, no organic lesions attributing to the present problem are found in fiber-optic laryngoscopy and stroboscopy. The problem in such events can be explained by non-organic factors, like respiratory kinematics, that is, the breathing pattern of the singers and its effect on their quality of voice.
Passive recoil of the chest wall and lungs is required for the generation of effective expiratory airflow. 1 The breathing pattern in human beings during singing and speaking differs from that during quiet respiration. This is due to dynamic alteration in respiratory kinematics (movements of the rib cage, diaphragm, and abdomen). Training during singing involves the development of optimal posture, efficient breathing, measured control of airflow, and voicing during phonation. In professional singers, the breathing kinematics result in improved range and power in the speech. The general conception is that the range of speech of professional singers depends on the vital capacity of the lungs. However, breathing kinematics/patterns play an equally important role. 2 It has been observed that a predominantly thoracic breathing pattern is often responsible for the professional voice to suffer in pitch. In such subjects (professional singers, in this context), voice therapy is offered to change the breathing kinematics from predominantly thoracic to predominantly diaphragmatic-abdominal, thus altering the dynamics of voice repulsion and improving pitch. 3 The diaphragm-abdomen complex effectively increases subglottic pressure and volume by assisting thoracic wall movements, and its role has been verified through electromyographic studies that have been noted in the classic literature.4,5 Thus, understanding the importance of the diaphragm-abdomen complex in respiratory kinematics is crucial in maintaining the voice qualities of professional voice users like singers, which is one of the major components in the speech rehabilitation of the affected subjects.
In addition, the treatment of the professional voice that has pitch problems is essentially multidisciplinary, with the active participation of the laryngologists, speech-language pathologists, and the patients themselves who need to be compliant and motivated. 6 Otolaryngologists in practice are the points of first contact for care services for professional voice users (including singers) before they are referred to speech and language pathologists for further evaluation and specialized management. 7 A considerable group of general otolaryngologists seeks active participation in the proceedings and the evolution of treatment results. A dedicated Voice Clinic necessary for the specialized evaluation of the professional voice is often established within the domains of the otolaryngology outpatients’ department, and the initial evaluation (such as history, fiber optic laryngeal examination, etc.) is performed by the otolaryngology residents themselves. The present attempt to understand the respiratory kinematics associated with acoustic parameters (pitch, in this case) and their effect on the professional singing voice is designed from the perspective of general otolaryngologists and for their understanding. The study, in the most simplified manner and design, evaluates the change in the pitch pattern of the singing voice (range of pitch, extremes of the range, and difference in range of pitch) after voice therapy in professional singers. The voice therapy here was directed at altering the respiratory kinematics in these singers who had predominantly thoracic respiration and presented voice problems such as easy fatigability and difficulty raising their voice to a higher pitch.
Materials and Methods
Study Design and Setting
This is a prospective, interventional (before-after/pre-post), and analytical study. It was conducted at the Voice Clinic of the ORL-HNS Department of a tertiary care teaching institute in eastern India from March 2021 to February 2023. Professional singers attending the Voice Clinic with complaints of easy voice fatigue and difficulty raising their singing voice to the higher notes were considered for the study and were subjected to the selection criteria.
Selection Criteria
The inclusion criteria included trained professional singers aged 25 to 50 years, both men and women, all having a predominantly thoracic breathing pattern, who successfully developed predominantly abdominal breathing after 1 month of monitored voice therapy. Smokers, the presence (or history) of any respiratory disorder and pulmonary pathology (determined by pulmonary function tests and chest skiagram), hypothyroidism, and those with underlying laryngeal pathology determined by flexible laryngoscopy and stroboscopy (like laryngopharyngeal reflux, fungal laryngitis, mass lesions such as nodules and polyps, muscle tension dysphonia) were excluded.
Post-Selection Work Flow
Before voice therapy, the selected candidates were subjected to voice recording. This was followed by an acoustic analysis of the voice using Praat software (https://www.fon.hum.uva.nl/praat/) that recorded the pitch range of the singing voice. The pitch range was calculated by subtracting the lowest pitch from the highest pitch of the range. Subsequently, the singers underwent voice therapy (vide infra) in the form of a change of breathing kinematics, postural correction with the help of visual feedback from the mirror, and a change of breathing pattern from thoracic to abdominal. The total duration of therapy allowed was 1 month. At the end of therapy, the singers, who now had the abdominal type of respiration, were re-evaluated through the objective assessment of their singing voice quality using the Praat software. Both before and after voice therapy, the pitch range, the extreme values of the pitch range, and the difference (change or improvement) in the pitch range after voice therapy were observed.
Voice Therapy
Voice therapy for these singers was performed in 4 steps:
Primary voice recording (vowels a/u/e and a sample high note song) and video recording to make them aware of the faulty postures and movement of the thorax and/or shoulder during habitual breathing and singing. Acoustic parameters considered here as primary data sources were the maximum duration of phonation and the pitch range.
Demonstration of abdominal breathing in silent movement of the abdominal-diaphragmatic muscle complex while keeping the thorax and shoulders at rest. Visual and tactile demonstrations were provided to the singers with mirrors and keeping hands on the lower abdomen/diaphragm to feel the muscle movement with breathing.
Training to generate voice from abdominal-diaphragmatic breathing by contracting the lower abdomen during voice production, singing, and training through the Lax Vox® tube (https://laxvox-institute.eu/en/; https://www.laxvox.com/). Acoustic parameters considered here for comparison were the maximum phonation duration and pitch range. Subjective relaxation in voice production was observed with abdominal pressure without fatigue.
Demonstration of high note production in singing voice with diaphragmatic breathing to practice in the singing model (the objective is to have the desired pitch-range elevation).
Statistical Analysis
The results were tabulated in Microsoft Excel spreadsheets (Microsoft Corporation; Redmond, Washington, USA) and analyzed with IBM SPSS (International Business Machines Corporation; Statistical Package for Social Sciences) Statistics software version 22.0.0.0 (Armonk, New York, USA; SPSS Inc., Chicago, Illinois, USA). Paired t-test analysis was carried out to compare the pitch range, its extreme values, and the difference in pitch range in professional singers before and after voice therapy. Factors such as the age of the singers (both male and female) and the duration of their singing career were correlated with pitch range before and after voice therapy, and the difference in pitch range after voice therapy. The correlation coefficients (r-value) were interpreted based on the guidelines provided in the review article by Akoglu.8,9 The level of statistical significance was established at P < .05.
Ethical Standards
This study was carried out following all the standard institutional protocols of the Scientific Technical Advisory Committee. The study was reviewed by the Institutional Ethics Committee, Deben Mahata Government Medical College and Hospital, Purulia, West Bengal, India, and approved for continuation adhering to all institutional rules and regulations according to Memo No. IEC/DMGMCH/2021/02. Written informed consent was obtained from each participant in the study. The methodology adopted to prepare this work was in accordance with the ethical standards of relevant national and institutional guidelines on human experimentation, as laid down in the Declaration of Helsinki of 1964, as revised in 2013 in Fortaleza, Brazil.
Level of Evidence
The present study has been assigned an evidence level of 3 following the Oxford Centre for Evidence-Based Medicine (March 2009). 10
Results
Of the 60 professional singers considered for the study, 55% were men and the rest were women. The mean age of the male singers was 34.24 years (range = 25-45 years; SD = 4.84) and that of the female singers was 35.92 years (range = 27-48 years; SD = 6.70). The average duration of the professional singing career of the study population was 12.56 years (range = 6-25 years; SD = 3.96).
All the singers included in the present study had thoracic breathing prior to therapy. The overall pre-therapy pitch range was 92.8 Hz (SD = 15.7; CV = 16.91). The average pre-therapy pitch range of the male singers was 85.84 Hz (range = 98-200 Hz; SD = 8.58; CV = 9.99), and that of the female singers was 101.29 Hz (range = 200-343; SD = 18.24; CV = 18).
Following 1 month of voice therapy, it was revealed that the singers had adopted an abdominal type of breathing during singing. The overall post-therapy pitch range was 189.21 Hz (SD = 26.56; CV = 14.03). The average post-therapy pitch range of the male singers was 178.54 Hz (range = 85-300 Hz; SD = 25.77; CV = 14.43) and that of the female singers was 202.25 Hz (range = 100-407; SD = 21.49; CV = 10.62).
The differences between the low and high pitch and the change in the pitch range before and after voice therapy have been graphically represented in Figures 1 and 2. The maximum and minimum change in pitch range was 123 and 5 Hz, respectively (average = 92.72 Hz) in the male singing voice, and 184 and 54 Hz, respectively (average = 102.07 Hz) in the female singing voice.
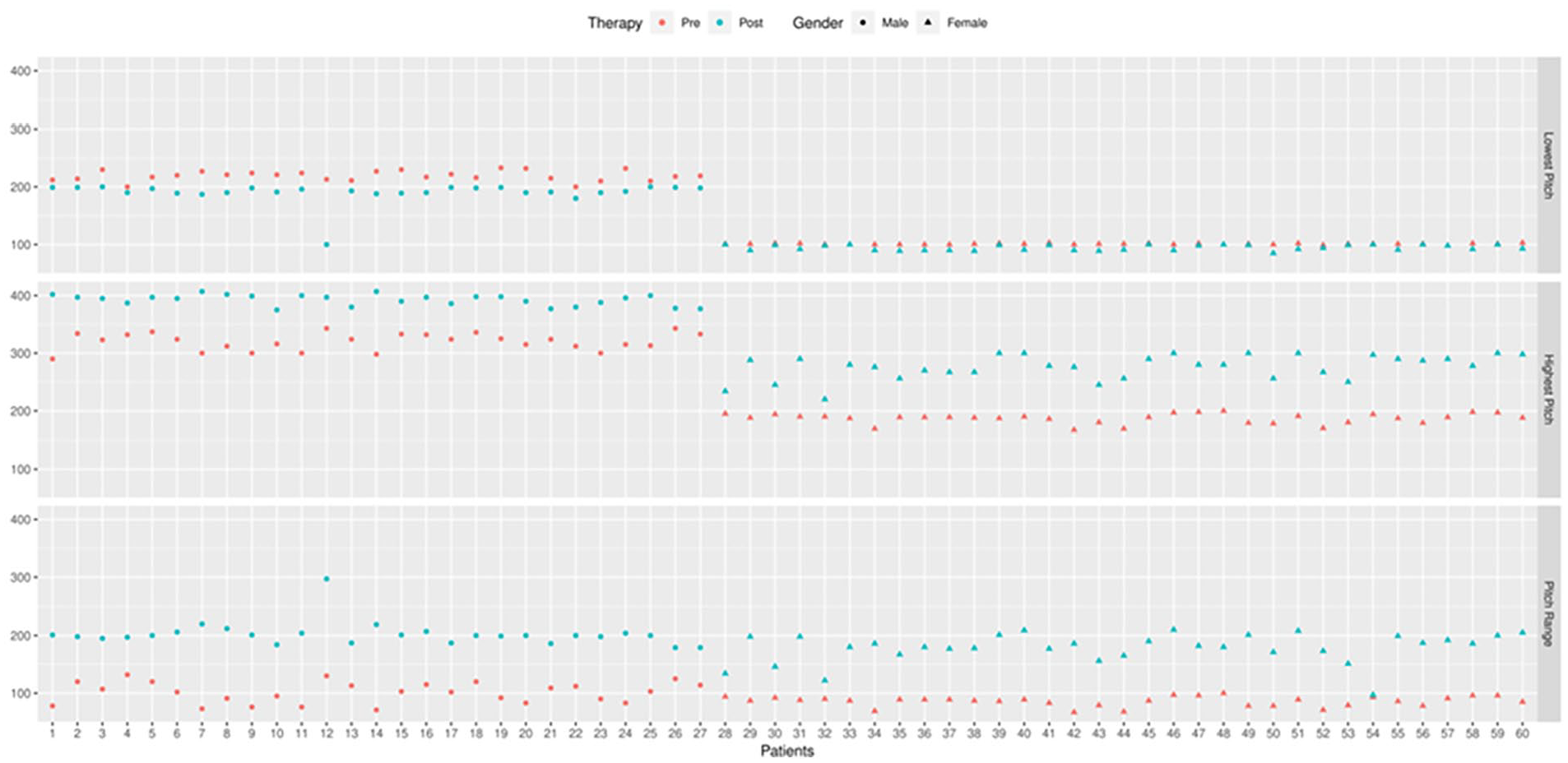
Scatter plot diagram showing the difference in pre- and post-therapy change of low pitch, high pitch, and pitch range in the individual patients in the study population.
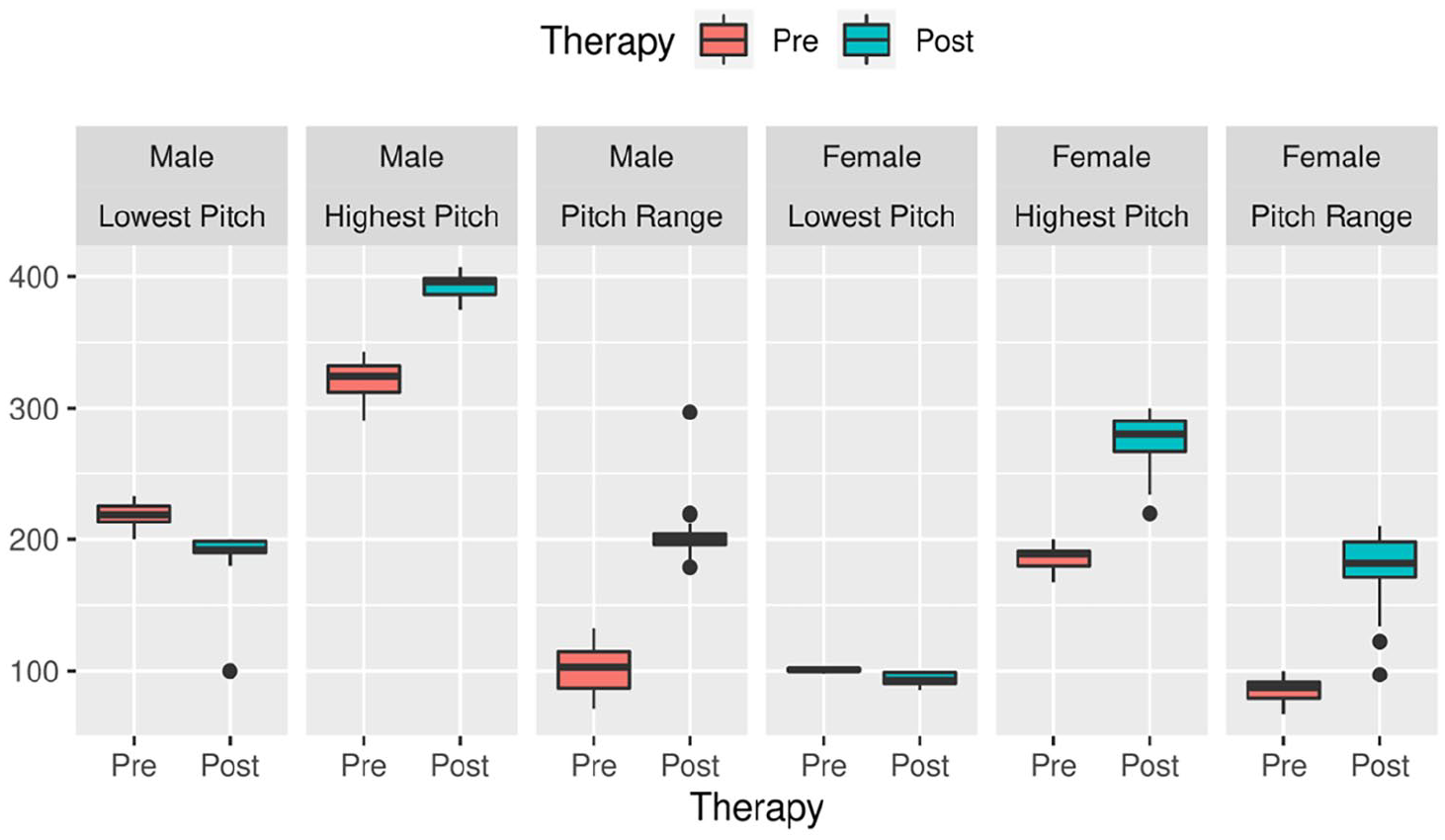
Box plot diagram showing the difference in pre- and post-therapy change of low pitch, high pitch, and pitch range with an average of all the components with respect to the gender of the study population.
Table 1 shows the mean differences between pre and post-therapeutic changes in the lowest and highest pitch of the voice during singing. The mean lowest pitch of the male and female singers was 100.88 ± 1.08 Hz and 219.07 ± 8.91 Hz, respectively, before voice therapy that decreased to 94.45 ± 4.71 Hz and 190.48 ± 18.79 Hz, respectively, after therapy. The changes before and after therapy were highly significant by the paired t-test in both male and female singers (t = 7.96 and 7.87, respectively, at a .0001 significant test level). The mean highest pitch in male and female singers, on the other hand, was 186.7 ± 8.81 Hz and 319.93 ± 14.87 Hz, respectively, before voice therapy; after therapy, it increased to 276.09 ± 21.26 Hz and 392.41 ± 9.48 Hz, respectively. In the present study, the increase in the mean highest pitch was highly significant after voice therapy using the paired t-test in male and female singers (t = 23.85 and 17.45, respectively, at a .0001 significant test level).
Mean Differences Between High and Low Pitch Values at Pre- and Post-Therapeutic Periods Among the Study Participants.
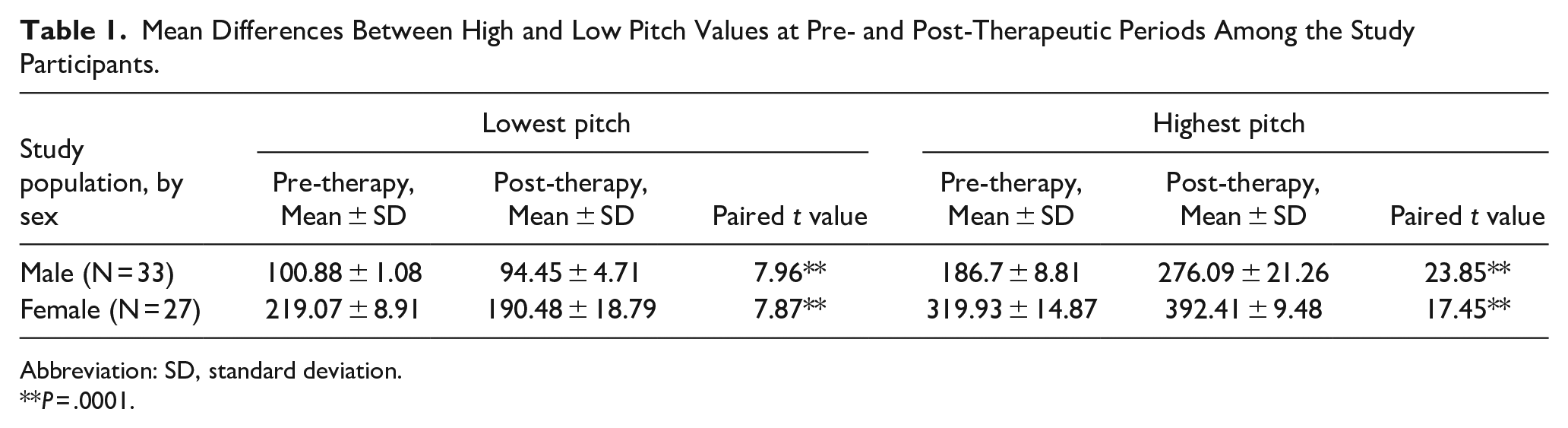
Abbreviation: SD, standard deviation.
P = .0001.
Table 2 shows the mean differences between pre and post-therapeutic changes in pitch range among subjects, by sex. The mean pitch range of male and female singers before voice therapy was 85.85 ± 8.58 Hz and 101.30 ± 18.24 Hz, respectively, which increased to 178.55 ± 25.78 Hz and 202.26 ± 21.49 Hz after therapy. The changes before and after therapy in pitch range were highly significant in both sexes by the paired t-test (t = 19.45 and 17.37, respectively, at a significant level of test of .0001).
Mean Differences Between Pitch-Range at Pre- and Post-Therapeutic Periods Among the Study Participants.
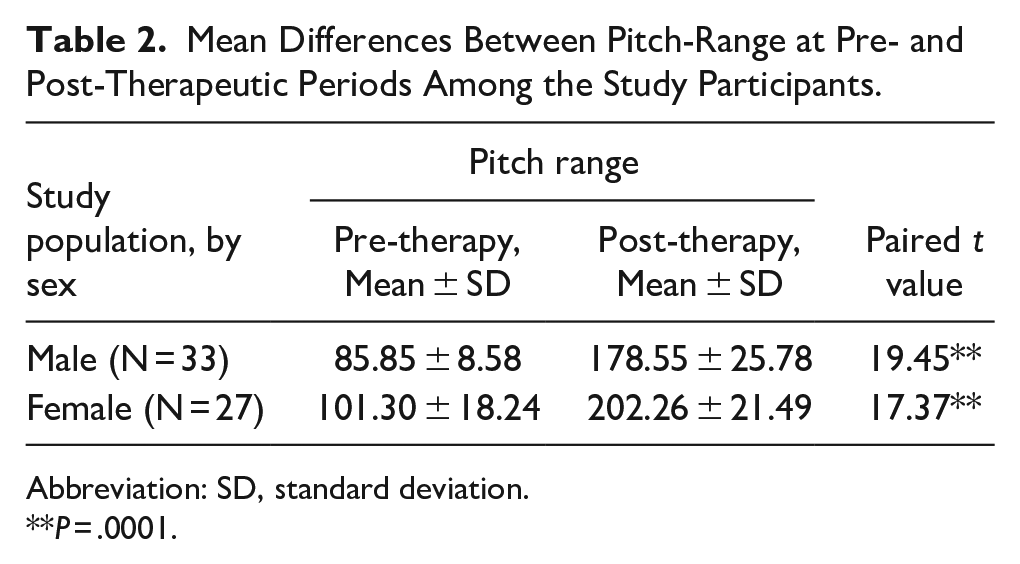
Abbreviation: SD, standard deviation.
P = .0001.
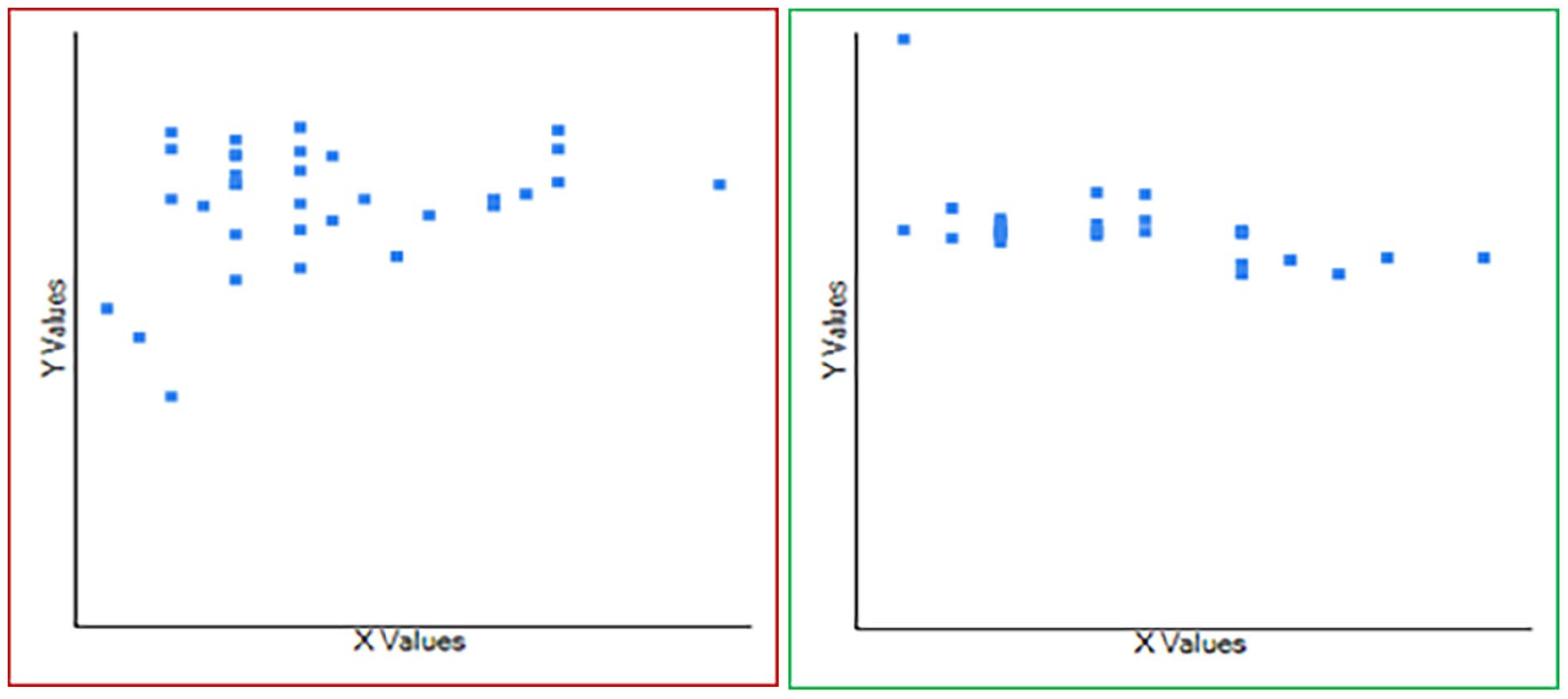
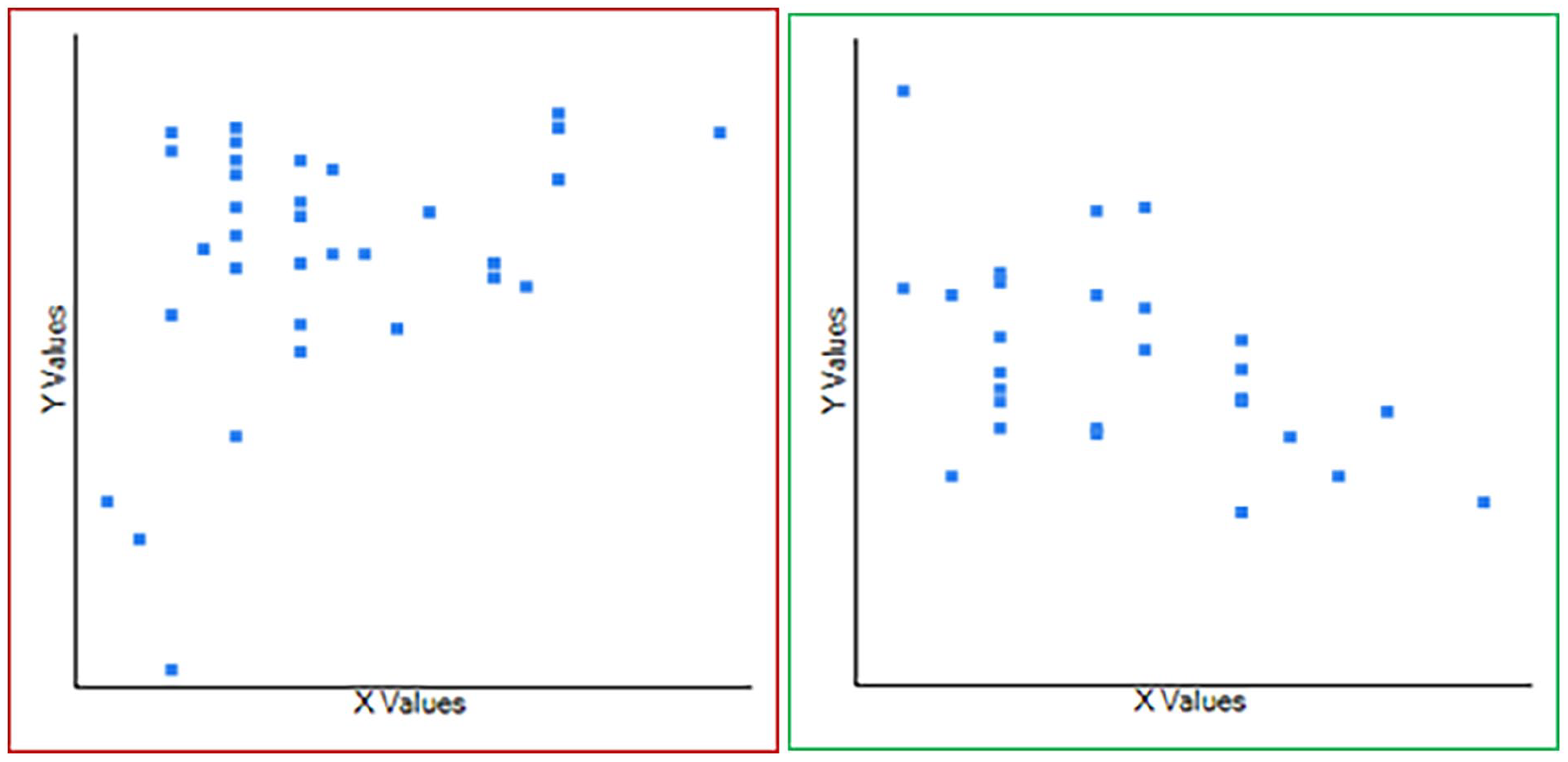
Age and pitch range before voice therapy were found to have a fair to moderate negative correlation among male singers (r = −.54) and a very poor positive correlation in female singers (r = .03) (Figure 3). Following voice therapy, a positive correlation of very poor strength was found between age and pitch range among male singers (r = .045) and a fair negative correlation among female singers (r = −.39) (Figure 4). The resulting difference in pitch range had a poor positive correlation strength with age (r = .21) in male singers but a fair negative correlation in female singers (r = −.30) (Figure 5).
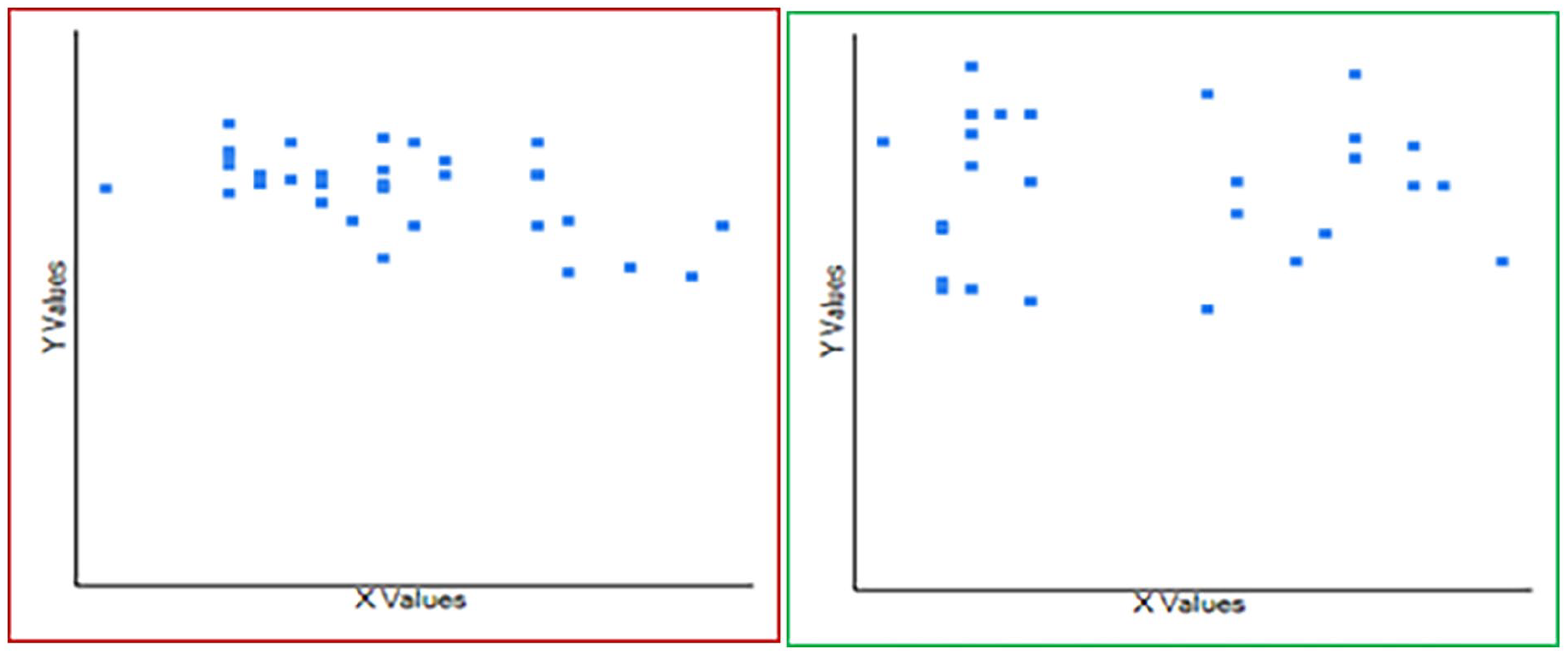
Correlation matrix between age and pitch range before speech therapy among the male (n = 33; red box) and female (n = 27; green box) singers. The X-axis denotes the mean age in years (34.24 ± 6.71 in men; 35.92 ± 6.70 in women). The Y-axis denotes the mean pitch range in Hertz (85.85 ± 8.58 in men; 101.30 ± 18.24 in women). A fair-to-moderate negative correlation (r = −.541; R2 = .2921) and a very poor positive correlation (r = .03; R2 = .0009) were noted, respectively.
Correlation matrix between age and pitch range following speech therapy among the male (n = 33; red box) and female (n = 27; green box) singers. The X-axis denotes the mean age in years (34.24 ± 6.71 in men; 35.92 ± 6.70 in women). The Y-axis denotes the mean pitch range in Hertz (178.54 in men; 202.25 in women). A very poor positive correlation (r = .045; R2 = .0021) and a fair negative correlation (r = −.39; R2 = .1539) were noted, respectively.
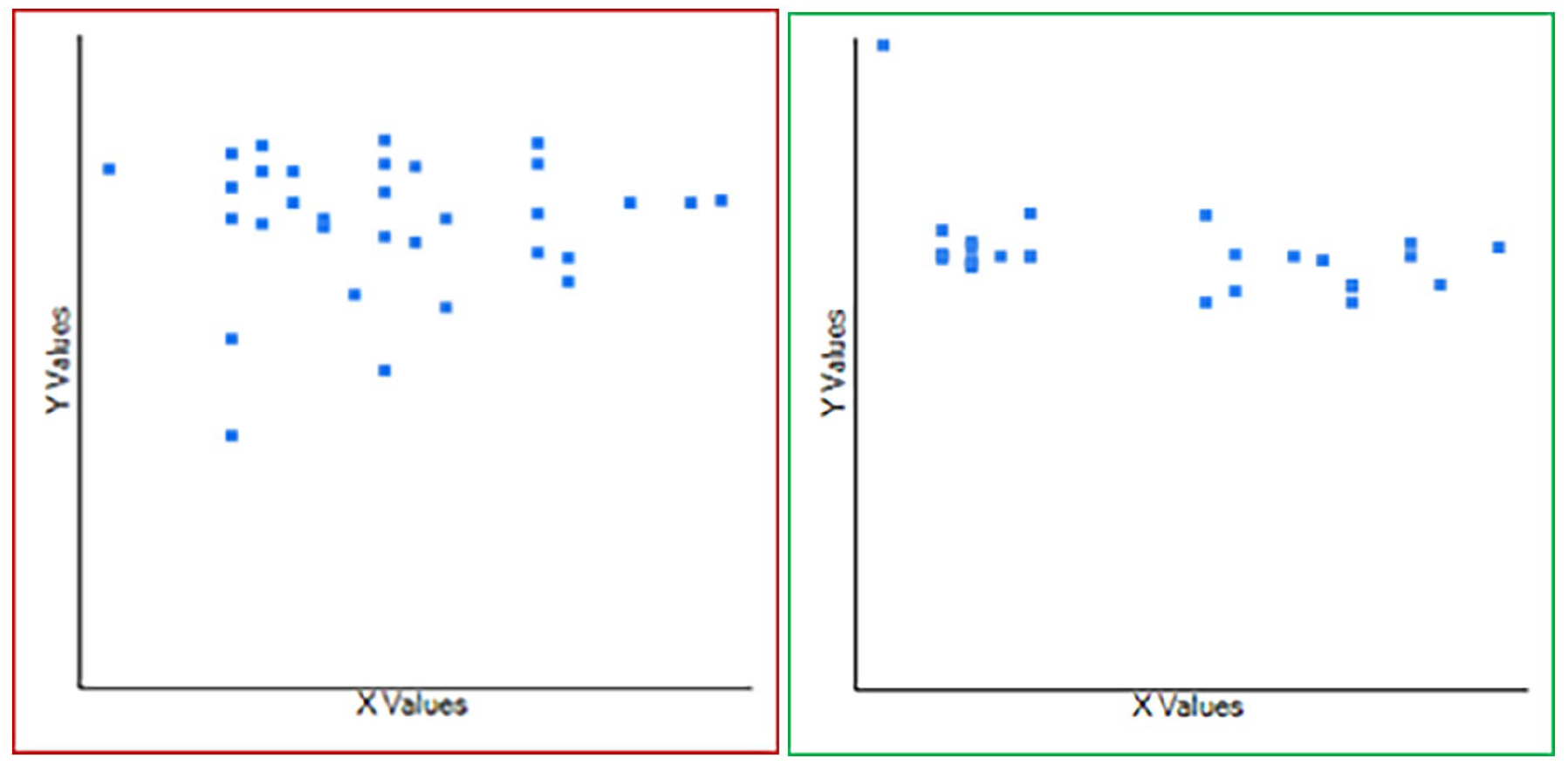
Correlation matrix between age and the difference in pitch range following speech therapy among the male (n = 33; red box) and female (n = 27; green box) singers. The X-axis denotes the mean age in years (34.24 ± 6.71 in men; 35.92 ± 6.70 in women). The Y-axis denotes the mean difference in pitch range in Hertz (92.70 ± 27.37 in men; 100.97 ± 30.20 in women). A poor positive correlation (r = .21; R2 = .04) and a fair negative correlation (r = −.3; R2 = .08) were noted, respectively.
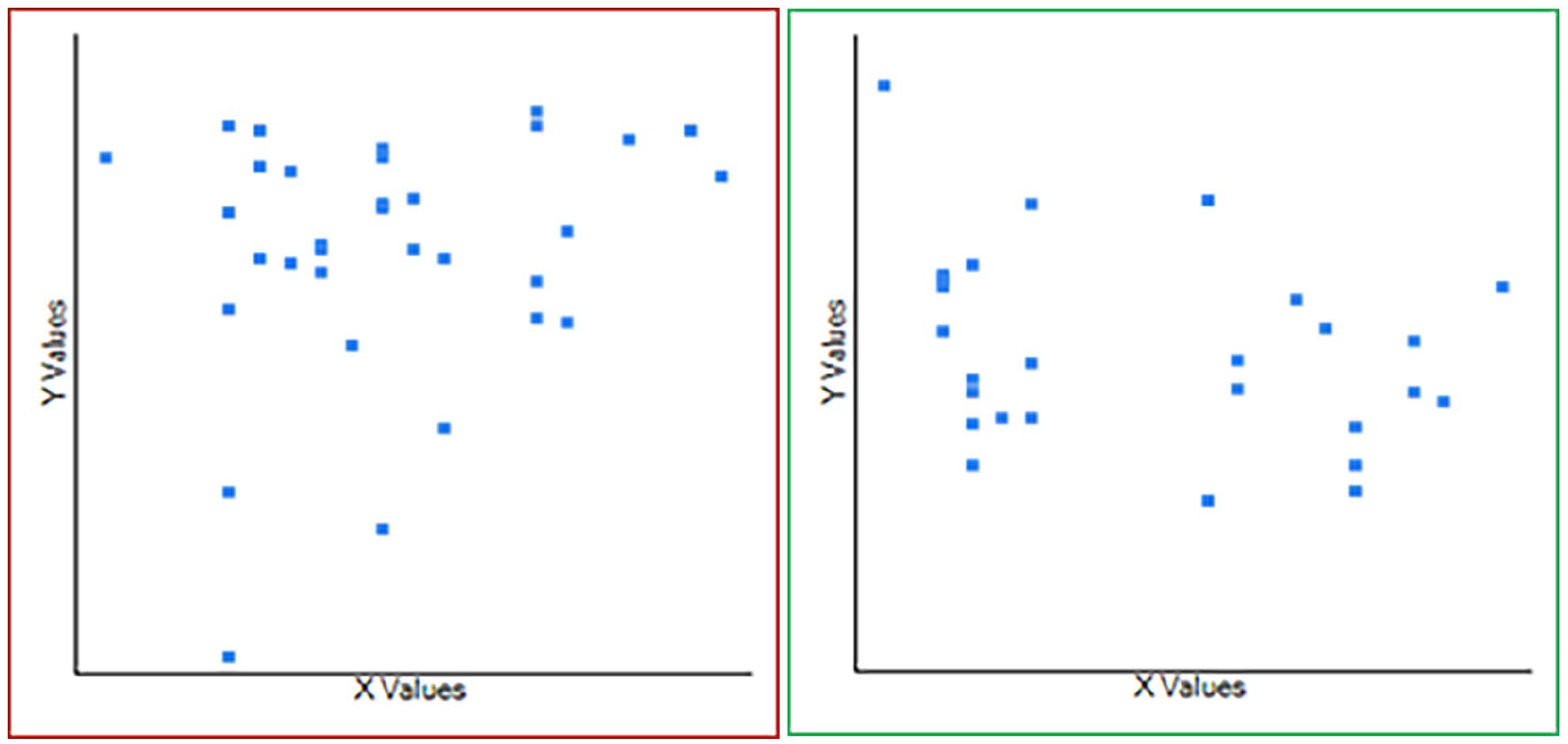
The present study also considered the duration of the singing career (in years) as one of the potential factors that could influence the outcome of respiratory kinematics after voice therapy. The duration of the singing period had a fair negative correlation with the pitch range before the initiation of voice therapy in men (r = −.36) and a poor positive correlation in women (r = .25) (Figure 6). The successful completion of voice therapy resulted in a fair positive correlation of the 2 variables in men (r = .3) and a fair negative correlation in women (r = −.5) (Figure 7). The difference in pitch range when computed against the duration of the professional career was found to have a fair positive correlation strength in male singers (r = .39) and a fair negative correlation in female singers (r = −.51) (Figure 8).
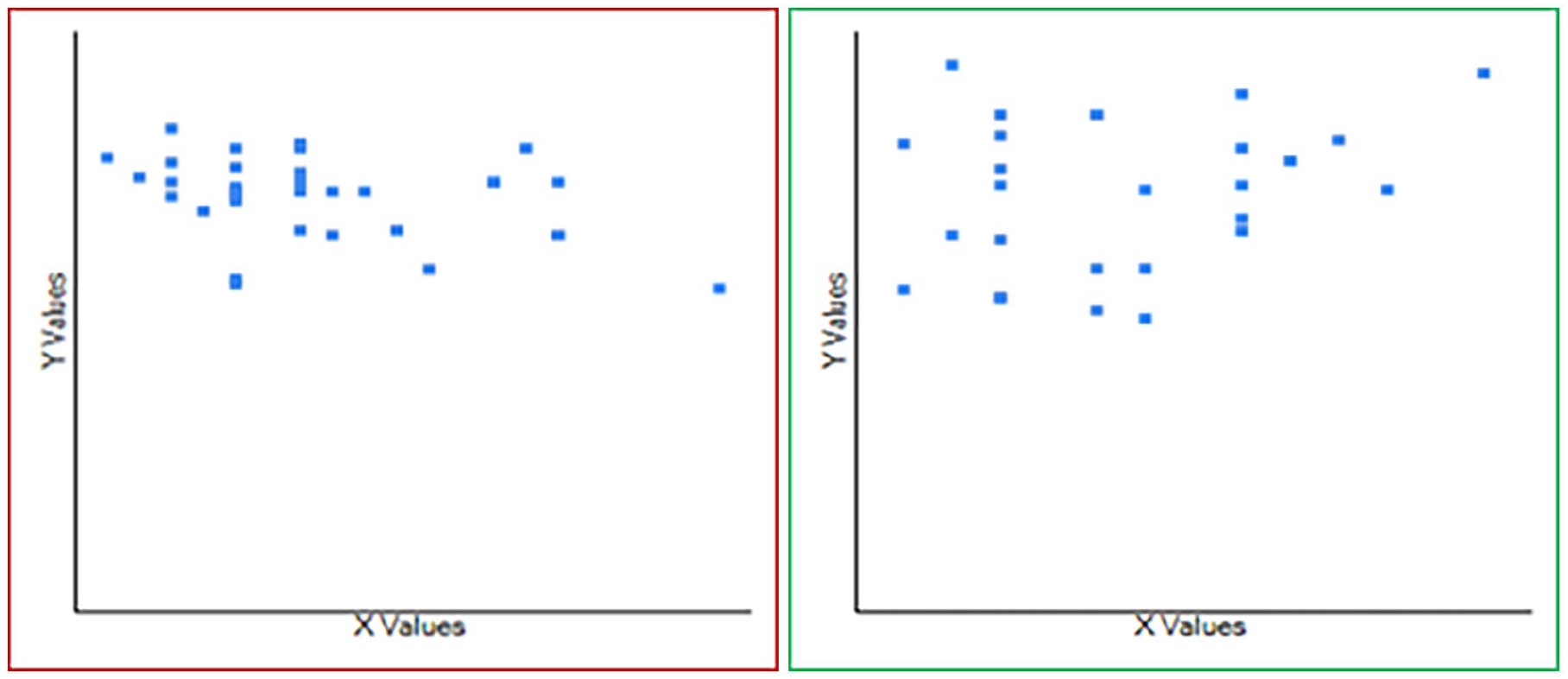
Correlation matrix between pitch range and duration of singing (in years) before speech therapy among the male (n = 33; red box) and female (n = 27; green box) singers. The X-axis denotes the mean duration of singing, in years (12.63 ± 4.56 in men; 12.48 ± 3.16 in women). The Y-axis denotes the mean pitch range in Hertz (85.85 ± 8.58 in men; 101.30 ± 18.24 in women). A fair negative correlation (r = −.36; R2 = .1283) and a poor positive correlation (r = .25; R2 = .0611) were noted, respectively.
Correlation matrix between pitch range and duration of singing (in years) after speech therapy among the male (n = 33; red box) and female (n = 27; green box) singers. The X-axis denotes the mean duration of singing, in years (12.63 ± 4.56 in men; 12.48 ± 3.16 in women). The Y-axis denotes the mean pitch range in Hertz (178.55 ± 25.78 in men; 202.26 ± 21.49 in women). A fair positive correlation (r = .3; R2 = .0871) and a fair negative correlation (r = −.5; R2 = .2514) were noted, respectively.
Correlation matrix between differences in the pitch range and duration of singing (in years) after speech therapy among the male (n = 33; red box) and female (n = 27; green box) singers. The X-axis denotes the mean duration of singing, in years (12.63 ± 4.56 in men; 12.48 ± 3.16 in women). The Y-axis denotes the mean pitch range in Hertz (92.70 ± 27.37 in men; 100.97 ± 30.20 in women). A fair positive correlation (r = .39; R2 = .15) and a fair negative correlation (r = −.51; R2 = .25) were noted, respectively.
Discussion
The present study evaluated the effect of the change in the breathing pattern from predominantly thoracic to abdominal by voice therapy in professional singers who present with easy voice fatigability and the inability to raise their pitch to a higher level during singing. With each subject acting as his/her control, a significant improvement in the acoustic parameter of the voice (pitch) was observed in everyone following voice therapy.
Pitch is the property of sound that can be graded on a frequency-related scale, and it is one of the many parameters that are altered by the type of respiration. The effect is most notable in the professional voice (singers), especially at higher pitches. Although pitch is closely related to and quantified as frequency, there exists a basic difference. The pitch is an auditory sensation and does not possess the purely objective physical property; it is a characteristic of the voice to perceive (“high” and “low” pitches make the music melodious”). 11 By contrast, the perceptive sensation of pitch is expressed as the fundamental frequency that measures the rate of vibration of the true cords during the production of musical vocal sounds.11,12 Vocal pitch is usually related to the size of the larynx and its structure. As a secondary function of the larynx, voice production with pitch as one of its many qualities depends on the lung reserve and the contour of the laryngeal framework and its physiology. The proposed theory of the “source filter mechanism” explains the generation of the human voice that involves the above structures.12,13 The lungs act as an air source driver or initiator, the glottis as a voice generator, the vocal/supralaryngeal tract (which normally makes a 90° angle between its supralaryngeal and oral axes in the erect head-neck position) as a resonator for the exhaled air volume, and finally the oral cavity and the oropharynx as articulators. 14 There are multiple systemic and local factors related to these anatomic areas that can alter the voice and one of its major qualifiers, the pitch. The pattern of respiration during the production of the singing voice is one of them.
Recent groundbreaking studies utilizing dynamic magnetic resonance imaging in interpreting the real-time effect of respiratory kinematics on the production of a singing voice revealed the crucial role of the diaphragm and abdominal muscles in professional voice users.15-17 These studies have helped otolaryngologists and speech-language pathologists understand the proposed causal links between voice disorders and the action of the respiratory muscles (chest and the abdomen/diaphragm complex). The respiratory kinematics is aimed at generating subglottic air pressure of adequate strength to produce a singing voice of necessary fundamental frequencies and their corresponding perceptive component (ie, the pitch). The diaphragm allows expansion of the thoracic cage during inspiration to accommodate the vital capacity in the lungs. However, it also has its passive role in expiration which is increasingly being recognized in the dynamic imaging studies mentioned above to be as important as the thoracic wall and the expiratory muscles of the abdomen for generating adequate subglottic pressure. During expiration, as air is expressed out of the lungs due to abdominal muscle contraction, the intercostal muscles partially counter chest contraction to prevent the collapse of the lungs. 17 Active elevation of the diaphragm and tonicity of the abdominal muscles ensure exit of expiratory air volume, and more importantly, generation of adequate subglottic air pressure against the closed glottis.18,19 For a singing voice, the elevation of the diaphragm against increased tidal volume (intrathoracic capacity) and prolonged expiratory time are of great importance for adding to the subglottic air pressure; the contribution of the abdomen-diaphragm complex is found to be greater than movements of the chest wall for this purpose.15-18,20,21 During singing, lung volume can be altered by changing body posture, and synchronous rib cage and abdomen-diaphragm displacement dictate the breathing pump. 22 That is, asymmetric abdominal movement with respect to the kinematics of the chest wall in the form of abdominal breathing is presumed to elevate both the diaphragm and the rib cage. This enables the development of the optimal subglottal pressure. 18 However, the action of the diaphragm on the chest wall during effective phonation is rather complex and anatomically partitioned, non-uniform, and asymmetric.23-26 Segmental or differential diaphragmatic movement is guided by the pitch jumps intended by the singers, and the results are also the function of the pulmonary capacity.15,23-26 A detailed discussion of this specific respiratory kinematics is beyond the scope of this article and the need for otolaryngologists in practice. However, a general guide for the readers’ understanding is provided in Figure 9. 15
The relationship between respiratory kinematics (including the action of the diaphragm) and changes in the pitch.
To develop a sustained, predominantly abdominal breathing pattern, professional singers need training, which is initially provided by their mentors. In fact, such training is also needed by other professional voice users, such as actors, lawyers, and teachers, who require proper voice throw using pitch (or the fundamental frequency). 27 The ineffective use of the abdomen-diaphragm complex in this population is a key factor that compromises vocal output. As it is understood, proper voice throws during vocalization in singers with the needed fundamental frequency results from adequate and optimum subglottic pressure and depends on 3 essential and interdependent functional units: the thoracic respiratory system, the abdomen-diaphragm complex, and integrity of the laryngeal outlet. Proper functioning of the laryngeal outlet requires healthy glottal closure (adduction) and preserved physiology of the laryngeal framework, including the vocal fold mucosa. In the present study, only singers with normal laryngeal anatomy and functioning (evident from flexible laryngoscopy and stroboscopy) were included, thus ensuring a normal laryngeal outlet system during voice generation. The study therefore dealt with the other 2 factors that determined the respiratory kinematics and attempted to evaluate the acoustic outcomes by converting thoracic-predominant breathing to abdominal-predominant breathing through voice therapy in professional singers facing trouble with their pitch.
With the anatomically and physiologically intact laryngeal outlet and voice projection mechanism, the singers selected in this study had a reduced pitch range, with pitch breaks, especially at the high end of the vocal range. For compensation, they strained their voice to reach the pitch range, which, in turn, led to early voice fatigue. 28 Scheduled and programmed voice therapy helped them adopt abdominal (diaphragmatic) breathing resulting in a significant improvement in pitch range.
Rigorous statistical analysis of the dataset derived from this study re-asserted the beneficial role of voice therapy on respiratory kinematics. Statistically significant differences were observed in the lowest and highest values of pitch range after voice therapy in both male and female singers. Likewise, the differences (ie, improvement) in pitch range were also significant in both groups after therapy, that is, the spectrum of pitch range got significantly widened. This was due to the change in respiratory kinematics that shifted to abdominal breathing.
However, it was interesting to note that the age of the singers had little role to play in the change in pitch range after voice therapy, nor was it strongly related to pitch range before and after therapy (Figures 3-5). It is the normal aging process that effectively reduces the pitch range with time. 29 However, the outcome may differ by gender. Ultrastructural changes in vocal folds associated with aging are responsible for an increase in fundamental frequency in men and a decrease in women. 30 Therefore, although none of the participants in the present study cohort had presbylaryngis per se, it is expected to have, in general, a stronger negative correlation between pitch range and increasing age, or, at most, a much weaker positive relationship. The findings of this study corroborated this and also the gender-specific contrasting relationship after therapy between age, pitch range, and difference in pitch range in male and female singers.
Currently, there is a dearth of literature that has explored the effect of the duration of a singing career on the qualities of the voice of a singer and its relationship with respiratory kinematics. 29 A non-singer voice should have its pitch range narrowed with time; however, in professional singers, the pitch range is expected to remain preserved even at the end of a relatively prolonged singing career due to proper training and breathing exercises.31,32 The average singing career of the present study participants was 12.56 years, and voice therapy appeared to restore the pitch range of the male singers (Figures 6-8). However, it is difficult to explain why, even after voice therapy, the duration of the singing career in female singers was inversely related to pitch range. However, the strength of the correlation was not strong enough in either group to consider the results as conclusive evidence. Data are limited in this context and are mostly restricted to female singers. 30 Thus, the duration of the professional singing career as a function of the voice quality modulated by voice therapy is a promising consideration for future research.
The present study has some limitations. First, the sample strength, although large enough to maintain statistical rigor with reliability and reproducibility of the results, is rather selective and exclusive. That is, the study considered only those singers who successfully developed predominantly abdominal from predominantly thoracic breathing after 1 month of voice therapy. Prolonged voice therapy could have included more singers, thus strengthening the sample size. In addition, those who could not respond satisfactorily to the month-long voice therapy were excluded. However, this absolute subject selection within a fixed time frame was not without reason. It focused on the primary objective of the study, that is, to evaluate the change in respiratory kinematics and its effect on the quality of the singing voice (the pitch). Therefore, by excluding inadequate and inconsistent responses to voice therapy, the differential outcome of change in voice quality could be avoided. The analysis and results were therefore more specific, to the point, and unambiguous.
Second, only 1 quality of the professional (singing) voice has been considered here, that is, the pitch (its range, extreme values, and change in the pitch range). The study can be replicated and extrapolated to the other acoustic parameters as well. However, pitch being one of the most consistent and widely used parameters, the study methodology was kept simple but still satisfying its primary objectives.
Third, in this review, concurrent factors such as singers’ age and career duration that can influence voice quality independent of breathing kinematics and response to voice therapy have not been ignored. Yet, a formal multivariate analysis was not considered necessary in the current statistical methodology because the correlation between pre-/post-therapy/difference in pitch range and age or duration of singing bore no more than a fair strength. That is, the strength of the association was never strong enough to consider factors such as age and career duration as major influences to alter the outcome of voice therapy on voice quality.
Conclusions
This study re-emphasizes, through a strong methodology and statistical rigor, the importance of the diaphragm-abdomen complex as the principal breathing pattern to be adopted by professional singers with voice problems related to pitch breaks. Voice therapy did play a vital role in converting predominantly thoracic respiration to a predominantly abdominal one, which, through the generation of adequate subglottic air pressure, restored the quality of the singing voice. One of the novelties of this study was to consider the possible effects of the age of the singers and their professional career duration as potential influencers on the effect of voice therapy on the pitch. In this context, both factors failed to develop a moderate/very strong correlation with the pre- and post-therapy pitch range and their difference.
Footnotes
Authors’ Notes
This work was started at Deben Mahata Government Medical College and Hospital, Purulia, West Bengal, India, by authors 1 and 3 who are permanent Government employees under the West Bengal Medical Education Service. Subsequently, they were transferred to their present affiliation following the Government’s periodic transfer policy.
Data Availability Statement
The clinical data for this patient are available with the authors and can be reproduced on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Written informed consent has been obtained from the patient for the publication of this clinic document. The clinical and surgical principles adopted for their management complied with the ethical standards of relevant national and institutional guidelines on human experimentation, as laid down in the Declaration of Helsinki, 1964, as revised in 2013.
Grant Number
Not applicable.