
Abstract
Introduction
Benign paroxysmal positional vertigo (BPPV) is the most common cause of vertigo, with approximately 17% to 42% of vertigo patients suffering from BPPV, and the lifetime prevalence of BPPV is 2.4%.1,2 BPPV is caused by dislodged otoliths resulting from injuries, infections, diabetes mellitus, migraines, osteoporosis, immobilization, or aging. Since each semicircular canal is in a different plane in space, the vestibule will be irritated due to the change in position when displaced otoliths collect in 1 or more semicircular canals, resulting in vertigo and nystagmus. 3 Recurrent episodes of vertigo lasting ≤1 minute caused by head movements are the typical symptom of BPPV, which usually recur within a few weeks if left untreated despite short-lived episodes. 4 Canalith repositioning maneuver is a common method for effectively treating BPPV, whose success rate is approximately 80% with a single application and increases to 92% with repeated applications. 5 However, some BPPV patients experience residual dizziness, postural instability, relapses, and psycho-emotional consequences for at least 1 month after canalith repositioning maneuvers, which may further affect the physical and mental health of such patients. 6 Age and gender have been found to be influencing factors for the development and recurrence of BPPV. BPPV is more likely to occur in older people than in younger people, with a peak incidence at the age of 50 to 60 years old, and it is also more common in women than in men (a male-female ratio: 1:2-1:3).7,8 However, the effects of incidence features and psychological factors on the presence of residual symptoms after the BPPV canalith repositioning maneuver have been rarely studied.
In this study, therefore, the incidence features, psychological factors, and presence or absence of residual symptoms after the canalith repositioning maneuvers in BPPV patients were detected, and the risk factors for the presence of residual symptoms were explored, thereby providing clinical data for the clinical prevention and treatment of BPPV.
Materials and Methods
Subjects
Subjects (193 in total) were recruited from BPPV patients who visited our hospital for treatment from July 2019 to December 2023 and were followed up in the outpatient clinic for 4 weeks after treatment. They were aged 36 to 73 years old, with a mean of (56.28 ± 7.15) years old, including 74 males and 119 females. The body mass index (BMI) was 18.82 to 29.57 kg/m2, with an average of (24.20 ± 2.35) kg/m2.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: (1) patients meeting the Bárány Society’s diagnostic criteria for BPPV 9 : recurrent episodes of positional vertigo or postural vertigo induced by a change in the direction of gravity of the head, the duration of vertigo attacks <1 min, and positional nystagmus could be induced by the Dix-Hallpike test or Roll test, (2) those aged >18 years old, and (3) those who could cooperate with outpatient follow-up for 4 weeks after treatment. Positional vertigo refers to vertigo triggered by specific changes in head position relative to gravity, commonly observed in BPPV when patients move into certain positions (eg, lying down, rolling over, or looking up). This type of vertigo is short-lived and directly linked to head movements that alter the orientation of the semicircular canals. On the other hand, postural vertigo refers to a sensation of dizziness or unsteadiness experienced when maintaining certain body positions or changing body posture (eg, standing up or bending over). It can occur without distinct head movements and is often associated with impaired balance, potentially influenced by vestibular dysfunction.
Exclusion criteria included: (1) patients with other dizziness-related diseases, (2) those with other organ diseases, (3) those who underwent medication or canalith repositioning maneuvers prior to consultation, or (4) those with disturbance of consciousness.
Methods of Canalith Repositioning Maneuvers
All canalith repositioning maneuvers were performed by 2 experienced clinicians with over 5 years of specialization in vestibular rehabilitation and BPPV management to ensure accuracy and consistency. Repeat repositioning maneuvers, if required, were conducted by the same clinician who performed the initial maneuver to maintain consistency in technique. Epley’s and Semont’s maneuvers were performed for patients with posterior semicircular canal-BPPV. Epley’s maneuver involved sequential head positioning to guide displaced otoliths back to the utricle, while Semont’s maneuver involved rapid lateral head movement to dislodge otoliths from the posterior canal. Additionally, Barbecue’s and Gufoni’s maneuvers were conducted for patients with horizontal semicircular canal-BPPV. Barbecue’s maneuver involved a series of head rotations in the horizontal plane, while Gufoni’s maneuver required a quick lateral movement to displace otoliths from the horizontal canal. For patients with anterior semicircular canal-BPPV, modified Epley’s maneuver was carried out to address the unique orientation of the anterior canal, adjusting head positions to optimize otolith repositioning.
Outcome Measures
Baseline data such as patients’ age, gender, BMI, history of diabetes, history of hypertension, smoking history, drinking history, educational level (university and above, or high school and below), and nature of work (physical or mental) were recorded. Symptoms and test results were collected before and 4 weeks after canalith repositioning maneuvers. Incidence features, including the time of disappearance of residual symptoms, the incidence rate of residual symptoms (number of subjects with residual symptoms at the time of follow-up/total number of subjects treated), the time from onset to consultation, the times of repositioning, and the type of BPPV were recorded.
The Dizziness Handicap Inventory (DHI) was used to assess the balance function of patients before repositioning and at the follow-up visit. 10 DHI covers physical, functional, and emotional dimensions, with a total score of 100 points, and the higher the score, the more severe the dizziness. Besides, the Hospital Anxiety and Depression Scale (HADS) was employed to assess the patients’ mental health. 11 HADS covers 2 dimensions (anxiety and depression), with 7 items for each dimension. Each item was scored 0 to 3 points, with a total score of 21 points, and a higher score indicated a more serious mental problem (>7 points: psychologically unhealthy, presence of depression or anxiety, and <7 points: good mental health). Moreover, the sleep quality of patients was evaluated by the Pittsburgh Sleep Quality Index (PSQI). 12 PSQI includes 7 items. Each item was scored 0 to 3 points, with a total score of 21 points, and the higher the score was, the worse the sleep quality would be (>7 points: sleep disorders).
The patients were assessed by 2 clinical specialists, each with over 5 years of experience in neurology and otolaryngology, ensuring consistency and accuracy.
Statistical Analysis
SPSS 22.0 software was utilized for statistical analysis. The DHI, HADS, and PSQI scores before and after treatment and measurement data in univariate analyses were described by mean ± standard deviation ( ± s), and compared by the independent-samples t-test. Count data were described by cases and compared by the χ2 test. With statistically significant factors as independent variables, the risk factors for and their correlations with the presence of residual symptoms after BPPV canalith repositioning maneuver underwent multivariate logistic regression analysis and Spearman correlation analysis, respectively. Receiver operating characteristic (ROC) curves were plotted using the significantly correlated factors to analyze the predictive efficiency of incidence features and psychological factors for residual symptoms. P < .05 was considered statistically significant.
Results
DHI, HADS, and PSQI Scores of BPPV Patients Before and After Treatment
After repositioning and a 4-week follow-up, the DHI scores, HADS anxiety and depression scores, and PSQI scores of the BPPV patients all significantly decreased (P < .05) (Table 1).
DHI, HADS, and PSQI Scores of BPPV Patients Before and After Treatment ( ± s, Point).
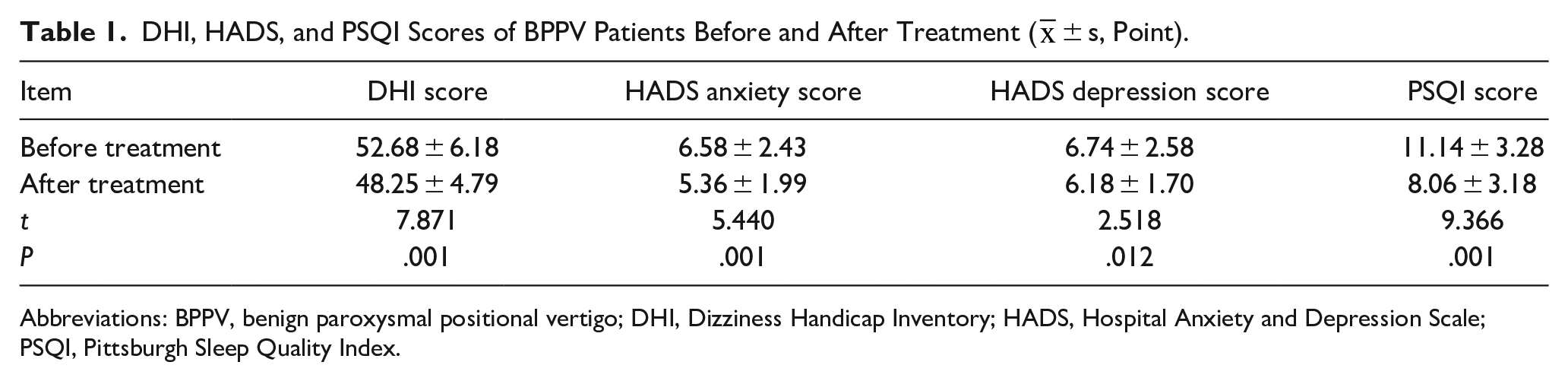
Abbreviations: BPPV, benign paroxysmal positional vertigo; DHI, Dizziness Handicap Inventory; HADS, Hospital Anxiety and Depression Scale; PSQI, Pittsburgh Sleep Quality Index.
Presence or Absence of Residual Symptoms After Treatment in BPPV Patients
After repositioning and a 4-week follow-up, 72 out of 193 patients (37.31%, 72/193) had residual symptoms including dizziness (58.33%, 42/72), a sense of instability (31.94%, 23/72) and a sense of traction in the head and neck (19.44%, 14/72). The remaining 121 patients (62.69%, 121/193) had no residual symptoms.
Results of Univariate Analysis on the Presence of Residual Symptoms After Repositioning in Patients with BPPV
Nature of work, time from onset to consultation, times of repositioning, type of BPPV, DHI score, HADS anxiety score, and PSQI score were associated with the presence of residual symptoms after repositioning in patients with BPPV (P < .05) (Figure 2). Age, gender, BMI, history of diabetes mellitus, history of hypertension, smoking history, drinking history, educational level, and HADS depression score had no associations with the presence of residual symptoms after repositioning in patients with BPPV (P > .05) (Table 2).
Results of Univariate Analysis on the Presence of Residual Symptoms After Repositioning in Patients with BPPV.
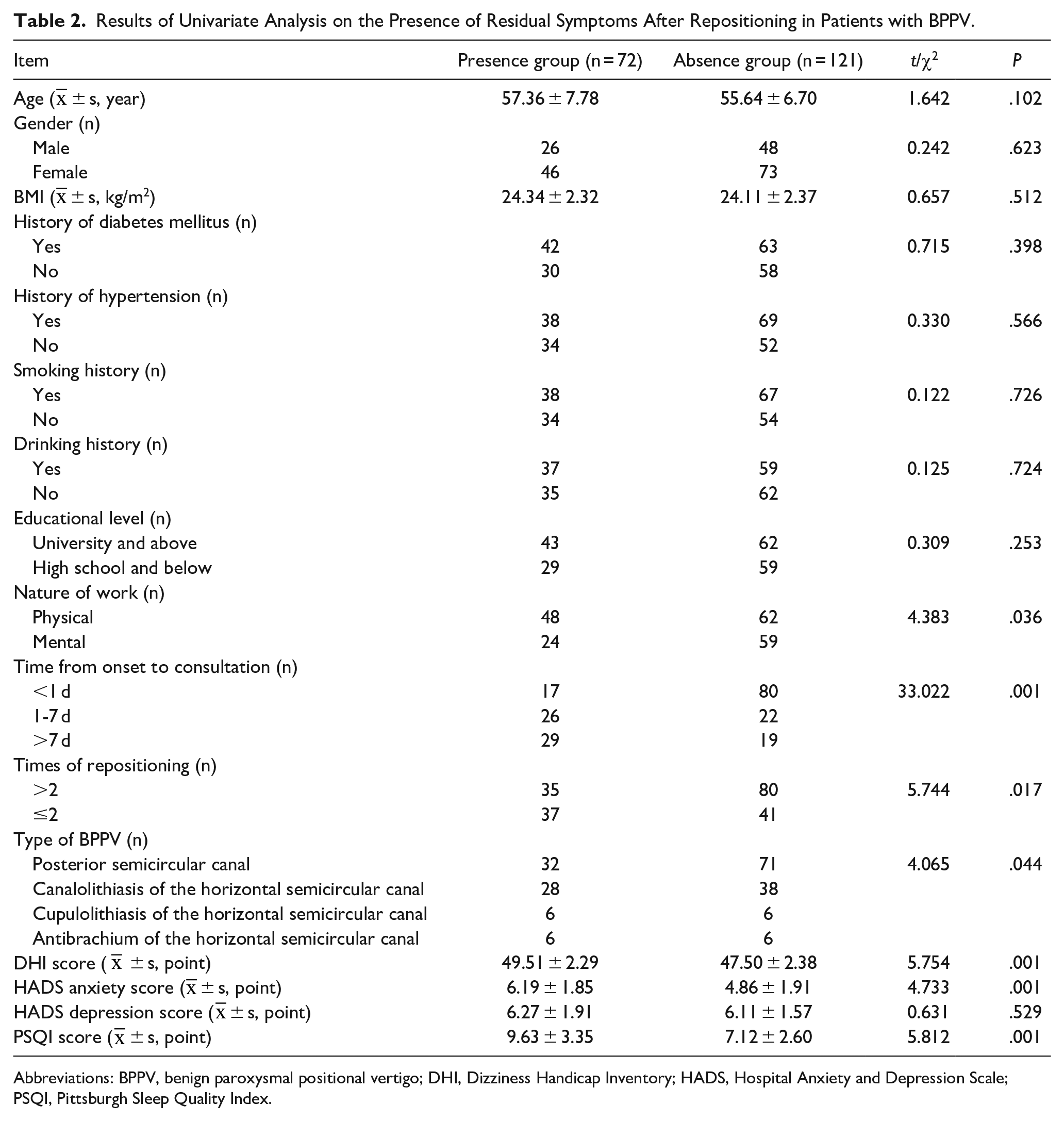
Abbreviations: BPPV, benign paroxysmal positional vertigo; DHI, Dizziness Handicap Inventory; HADS, Hospital Anxiety and Depression Scale; PSQI, Pittsburgh Sleep Quality Index.
Results of Multivariate Logistic Regression Analysis on Influencing Factors for the Presence of Residual Symptoms After Repositioning in Patients with BPPV
The results of multivariate logistic regression analysis showed that the nature of work, time from onset to consultation, DHI score, HADS anxiety score, and PSQI score were independent risk factors for the presence of residual symptoms after repositioning in patients with BPPV (P < .05) (Table 3; Figure 1).
Results of Multivariate Logistic Regression Analysis on Influencing Factors for the Presence of Residual Symptoms After Repositioning in Patients with BPPV.
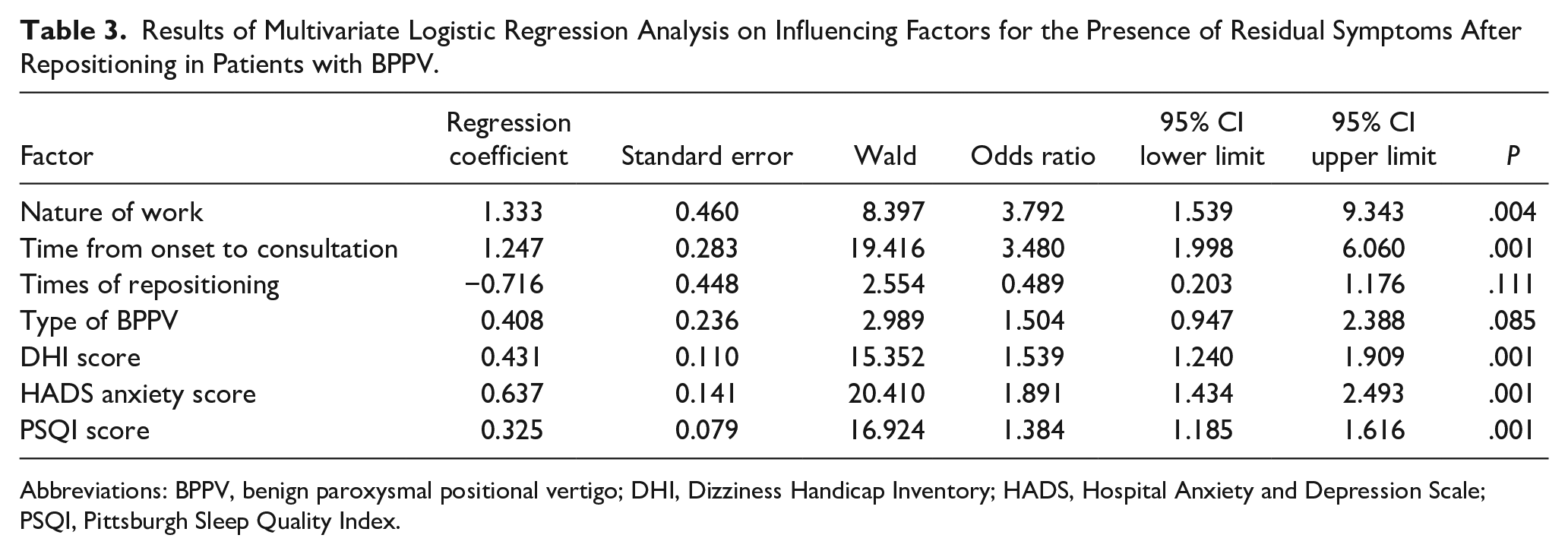
Abbreviations: BPPV, benign paroxysmal positional vertigo; DHI, Dizziness Handicap Inventory; HADS, Hospital Anxiety and Depression Scale; PSQI, Pittsburgh Sleep Quality Index.
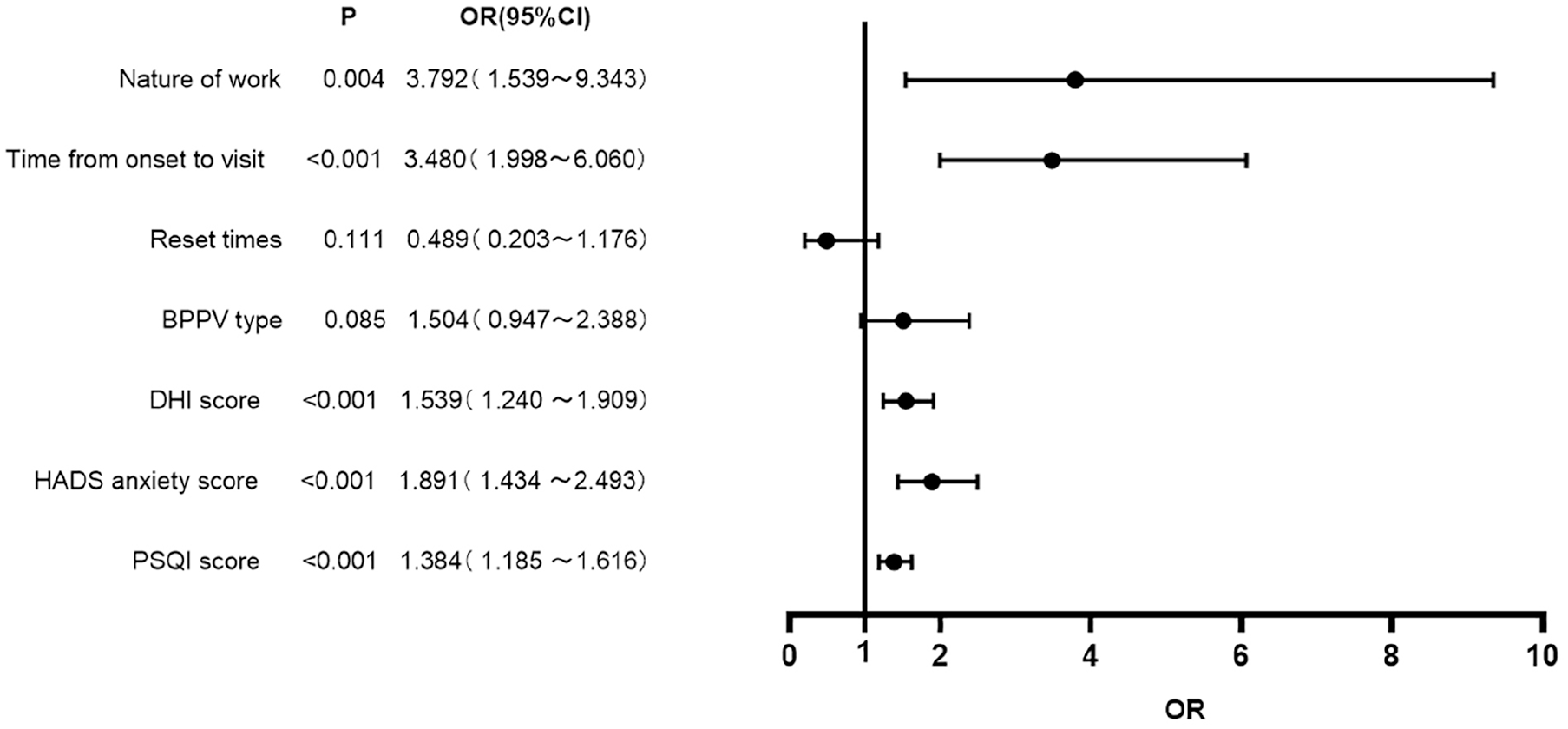
Forest plot of clinical characteristics based on multivariate logistic regression analysis.
Spearman Correlations of Influencing Factors with the Presence of Residual Symptoms After Repositioning in Patients with BPPV
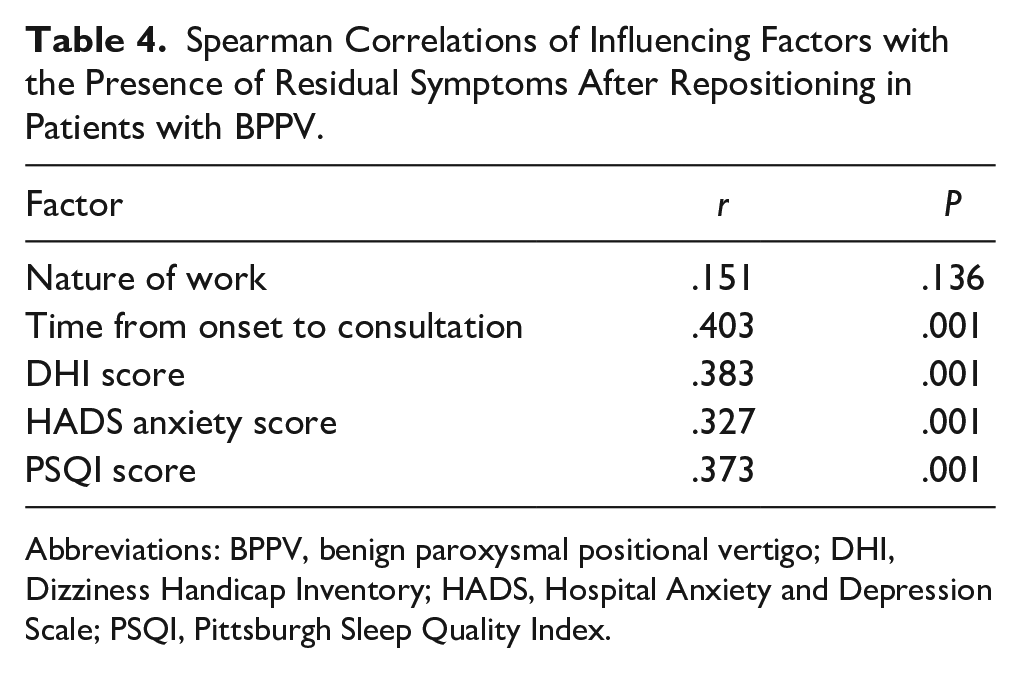
According to the Spearman correlation analysis results, the presence of residual symptoms after repositioning in patients with BPPV had significant positive correlations with the time from onset to consultation, DHI score, HADS anxiety score, and PSQI score (P < .05), while it had less correlations with nature of work (P > .05) (Table 4).
Spearman Correlations of Influencing Factors with the Presence of Residual Symptoms After Repositioning in Patients with BPPV.
Abbreviations: BPPV, benign paroxysmal positional vertigo; DHI, Dizziness Handicap Inventory; HADS, Hospital Anxiety and Depression Scale; PSQI, Pittsburgh Sleep Quality Index.
Results of ROC Curve Analysis on Influencing Factors for the Presence of Residual Symptoms After Repositioning in Patients with BPPV
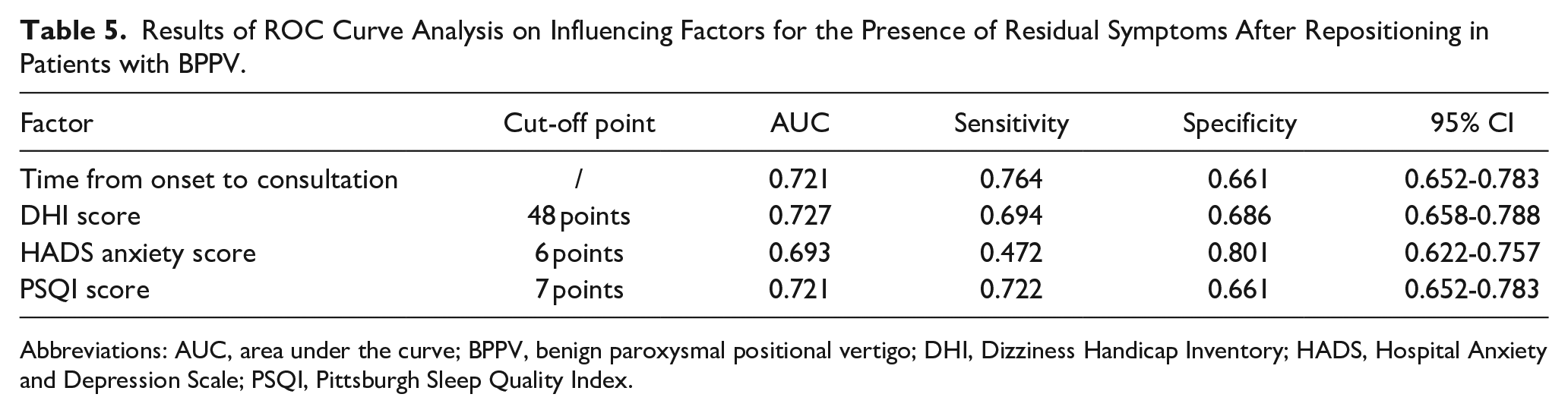
The statistically significant factors in the above multivariate logistic regression analysis were subjected to ROC curve analysis. The area under the ROC curve (AUC) of the DHI score for predicting the presence of residual symptoms after repositioning in patients with BPPV was the largest (0.727), and the time from onset to consultation and the HADS anxiety score had the highest sensitivity (0.764) and specificity (0.801), respectively (Table 5; Figure 2).
Results of ROC Curve Analysis on Influencing Factors for the Presence of Residual Symptoms After Repositioning in Patients with BPPV.
Abbreviations: AUC, area under the curve; BPPV, benign paroxysmal positional vertigo; DHI, Dizziness Handicap Inventory; HADS, Hospital Anxiety and Depression Scale; PSQI, Pittsburgh Sleep Quality Index.
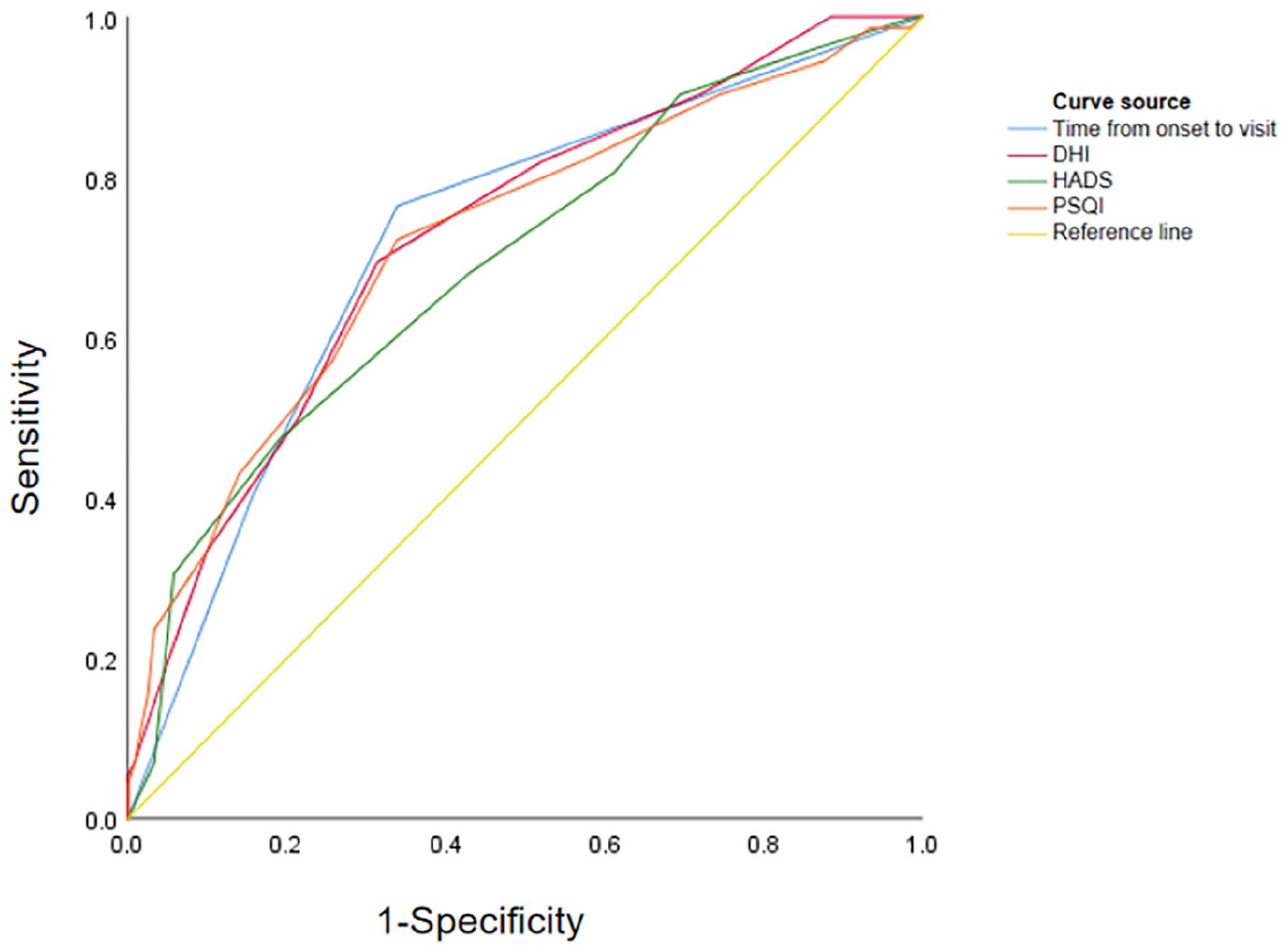
Results of ROC curve analysis on influencing factors for the presence of residual symptoms after repositioning in patients with BPPV. ROC, receiver operating characteristic curve; BPPV, benign paroxysmal positional vertigo.
Discussion
BPPV is the most common peripheral vestibular disorder mainly characterized by mild-to-severe dizziness, nausea, and vomiting resulting from a sudden and transient feeling of vertigo, which can last for days or even months, and can recur years later after relief of symptoms. 13 Manual repositioning is the most effective treatment for BPPV nowadays, which can effectively relieve the feeling of vertigo in a relatively short period of time, and eliminate vertigo and nystagmus in the postural test. However, some patients still suffer residual symptoms such as persistent dizziness or lightheadedness, unsteady standing, floating walking, or paroxysmal dizziness or unsteady standing when they look up, down, and turn around. Residual symptoms are thought to stem from incomplete clearance of otolith debris or delayed adaptation by the central nervous system. 14 Age and comorbid vestibular conditions, including vestibular migraines, have been linked to prolonged symptoms, likely due to slower compensation mechanisms. 15 Metabolic factors, such as vitamin D deficiency, are also associated with increased recurrence and persistence of symptoms, suggesting their influence on otolith stability. 16 Therefore, it is of great significance to investigate the influencing factors for the presence of residual symptoms after the BPPV canalith repositioning maneuvers.
In this study, 193 patients with BPPV were treated with repositioning. After repositioning and a 4-week follow-up period, the DHI scores, HADS anxiety scores, HADS depression scores, and PSQI scores of the BPPV patients all significantly decreased, but 72 patients still had residual symptoms, and the incidence rate of residual symptoms was 37.31%, similar to the findings of Jiang et al 17 It can be seen that residual symptoms after repositioning have a high incidence rate. The incidence of residual symptoms in BPPV patients after repositioning may be related to the vestibular system dysfunction, a small number of small otolith fragments remaining after repositioning, and tension and anxiety. 18 In this study, the nature of work, time from onset to consultation, times of repositioning, type of BPPV, DHI score, HADS anxiety score, and PSQI score were associated with the presence of residual symptoms after repositioning in patients with BPPV. The results of multivariate logistic regression analysis showed that the nature of work, time from onset to consultation, DHI score, HADS anxiety score, and PSQI score were independent risk factors for the presence of residual symptoms after repositioning in patients with BPPV. The presence of residual symptoms after repositioning in patients with BPPV had significant positive correlations with the time from onset to consultation, DHI score, HADS anxiety score, and PSQI score. The time from onset to consultation can affect patients’ social functioning and mental health, and the longer the duration of BPPV, the greater the mental stress and the more likely to have residual symptoms such as lightheadedness, unsteady standing, and floating walking.19,20 In addition, the DHI involving physical, functional, and emotional dimensions can effectively evaluate the presence or absence of residual symptoms in patients. In this study, AUC of the DHI score for predicting the presence of residual symptoms after repositioning in patients with BPPV was 0.727, and there was a significant positive correlation between the DHI score and the presence of residual symptoms. Therefore, the DHI score can serve as an important predictor for the presence of residual symptoms in patients with BPPV after repositioning. Moreover, the results of this study revealed that the degree of anxiety was positively correlated with the presence of residual symptoms, and the specificity of the HADS anxiety score for predicting the presence of residual symptoms after repositioning in patients with BPPV was 0.801, suggesting a significant predictive value. BPPV patients with psychiatric disorders such as anxiety and depression are more prone to residual symptoms after repositioning. When the vestibular system is abnormally irritated after BPPV occurs, the patients may have emotional changes and collapse into depression or anxiety. In turn, these negative emotions can affect the vestibular function, making patients more susceptible to vertigo and other residual symptoms after repositioning. Such a vicious circle causes great harm to the quality of life of patients.21-23 In a previous study, it was found by two-year follow-up on BPPV patients that sleep quality as assessed by the PSQI is strongly associated with recurrence of BPPV after repositioning. 24 Shortened sleep duration, prolonged sleep latency, decreased sleep efficiency, daytime dysfunction, and increased use of sleep medications can lead to the development of residual symptoms after the BPPV canalith repositioning maneuver. Patients with poor sleep quality may experience episodes of vertigo when lying in bed due to positional change, which can make them feel nervous and difficult to fall and stay asleep. Moreover, dizziness due to a change in the angle of the head during sleep may awaken patients.25,26
While our study utilized subjective measures such as DHI, HADS, and PSQI to assess dizziness impact, mental health, and sleep quality, it is worth noting that objective assessments such as Ocular Vestibular Evoked Myogenic Potentials (OVEMP) and Subjective Visual Vertical (SVV) are valuable tools for evaluating vestibular function. OVEMP can objectively measure otolith function and the vestibulo-ocular reflex pathway, providing insights into utricular and saccular health, 27 while SVV assesses a patient’s perception of verticality, indicating potential vestibular dysfunction. 28 Including these objective measures in future research can offer a more comprehensive understanding of vestibular impairment and residual symptoms following canalith repositioning maneuvers in BPPV patients.
This study is crucial as it addresses gaps in understanding factors influencing the residual symptoms after canalith repositioning maneuvers for BPPV, which affect the quality of life and healthcare use. By examining a standardized 4-week period after treatment and incorporating a range of risk factors besides age and gender, this study may help improve patient stratification and treatment approaches, guiding more targeted follow-up and care for high-risk patients. However, this study had some limitations, such as a short follow-up period, a small sample size, and no investigation of the recurrence rate of BPPV. In the future, the sample size together with cases of residual symptoms should be further expanded to observe the long-term effect and recurrence rate.
Conclusion
In conclusion, time from onset to consultation, DHI score, HADS anxiety score, and PSQI score are independent risk factors for the presence of residual symptoms after repositioning in patients with BPPV, which should be paid more attention to during clinical diagnosis and treatment. Patients should go to the hospital for repositioning as soon as they develop symptoms, thereby alleviating their mental stress, raising sleep quality, relieving residual symptoms as soon as possible, and improving social functioning.
Footnotes
Author Contributions
Study concept—S.Y.; Study design—S.Y., P.G.; Materials—Z.L.; Data Collection and analysis—P.C.; Writing—W.W.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by Beijing Haidian Hospital 2020 Hospital-Level Research Fund Project (No. KYQ2020028).
Ethics Statement
The study has received ethical approval from Beijing Haidian Hospital (BJHDRHS2023-12421).