
Abstract
Objectives:
Steroid-eluting stent implantation after endoscopic sinus surgery (ESS) effectively alleviates postoperative symptoms and polyp recurrence in patients with chronic rhinosinusitis with nasal polyps (CRSwNP). However, the efficacy of steroid-eluting stents for the treatment of olfactory dysfunction in CRSwNP and the influencing factors therein have not been studied.
Methods:
Fifty-nine patients with CRSwNP with olfactory dysfunction from Peking University Third Hospital who were hospitalized for ESS were recruited and randomly divided into a stent group (n = 30) and a control group (n = 29), and were assessed for symptom scores, olfactory function, endoscopic findings, and type 2 inflammatory mediators (IL-4, IL-5, IL-13, IL-33, eotaxin-3, periostin) expression.
Results:
Postoperative olfactory Visual Analogue Scale (VAS) scores, T&T olfactometer scores, SNOT-22 scores, and Lund-Kennedy (LK) scores were reduced in patients with CRSwNP (P < .01). Postoperative olfactory VAS scores, T&T olfactometer scores, SNOT-22 scores, and LK scores, IL-5, IL-13, and periostin were significantly lower in the stent group than in the control group (P < .05). Correlation analysis was performed and found that the postoperative olfactory VAS scores were strongly correlated with IL-5 and IL-13 (r = .496, P < .001 and r = .289, P = .026), and the postoperative T&T olfactometer scores were strongly correlated with IL-5 and IL-13 (r = .553, P < .001 and r = .398, P = .002).
Conclusions:
Steroid-eluting stent implantation after ESS is an effective treatment for olfactory deficits in patients with CRSwNP and may be related to the stent’s more effective reduction of local type 2 inflammatory mediators in the nasal cavity.
Keywords
Chronic rhinosinusitis (CRS) is a multifactorial, heterogeneous inflammatory disease of the nasal cavity and sinuses, in which persistent inflammation of the sinus mucosa leads to the formation of nasal polyps and typical symptoms such as nasal congestion, pus, headache, and olfactory dysfunction. 1 The prevalence of olfactory dysfunction in patients with CRS, especially chronic rhinosinusitis with nasal polyps (CRSwNP), can be as high as 80%, which seriously affects the quality of life of patients. 2 In recent years, many studies have identified type 2 inflammation as an important factor in the development of nasal polyps and olfactory impairment.3,4 Our team’s previous studies found that olfactory dysfunction after endoscopic sinus surgery (ESS) was also caused by elevated type 2 inflammation. 5 Therefore, it is extremely important to find new therapeutic approaches to control type 2 inflammation and thus improve postoperative olfactory function in patients with CRSwNP.
Glucocorticosteroids have significant anti-inflammatory effects, and nasal glucocorticosteroids are the first-line drugs for the treatment of CRS. Some scholars have reported that intranasal glucocorticosteroids or short-term oral glucocorticosteroids can significantly improve olfactory dysfunction in patients with CRSwNP, but some studies have pointed out that nasal glucocorticosteroids are ineffective in treating olfactory dysfunction.6 -8 Steroid-eluting stents have the dual role of physically supporting the opening of the operative cavity and controlled slow-release of glucocorticosteroids, which, when implanted in the sieve sinus cavity, can greatly reduce mucosal swelling, sinus atresia, and the likelihood of re-intervention in the postoperative period.9 -11 A recent study found that steroid-eluting stents were effective in reducing nasal type 2 inflammation and sinusitis symptoms. 12 However, to the best of our knowledge, there are no studies on the efficacy of glucocorticoid stents for the treatment of olfactory impairment in CRSwNP. Therefore, in this study, we aimed to evaluate the therapeutic efficacy of glucocorticoid stents for postoperative olfactory impairment in patients with CRSwNP.
Materials and Methods
This study was a prospective, randomized controlled study. Patients with CRSwNP with an olfactory impairment who met the inclusion criteria were randomized into a stent group and a control group (Figure 1). General clinical data, olfactory function, and severity of disease symptoms including SNOT-22 score, 13 Lund-Kennedy (LK) score, 14 and Lund-Mackay (LM) score 15 were collected from all patients preoperatively. Preoperative peripheral blood and nasal secretions were retained from the patients. ESS was performed for all patients and the polyp tissue was retained intraoperatively. The patients were followed up and reviewed 3 months after ESS.
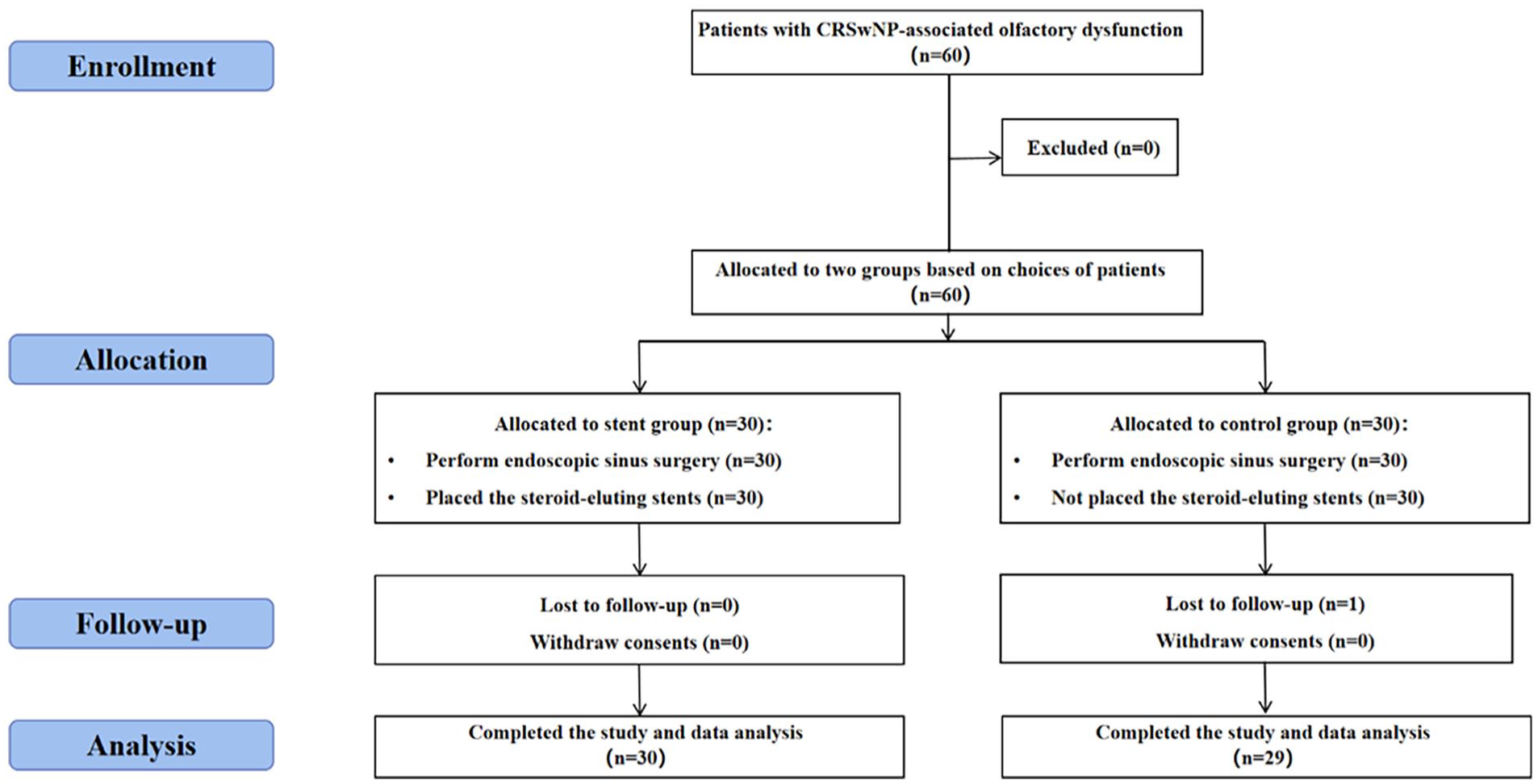
Flow diagram of this study. CRSwNP, chronic rhinosinusitis with nasal polyps.
Subjects
This study enrolled patients between November 2022 and January 2024 who were admitted to Peking University Third Hospital for ESS. All the patients met the diagnostic criteria for chronic sinusitis with nasal polyps per the guidelines mentioned in the European Position Paper on Rhinosinusitis and Nasal Polyps 2012 (EPOS-2012). 16 The exclusion criteria are: (1) younger than 18 years or 80 years and older; (2) patients with comorbidities such as nasal sinus tumors and fungal sinusitis; (3) patients with a history of intracranial and olfactory region tumors, congenital anosmia, accompanied by systemic factors that may affect olfactory function such as autoimmune diseases, cystic fibrosis, and other disorders; (4) patients with allergies to the device materials or their degradation products (e.g., mometasone furoate); (5) patients with a history of immunodeficiency, glaucoma or high intraocular pressure, cataract, severe diabetes or hypertension. The study was approved by the Ethics Committee of Peking University Third Hospital (Ethics Committee Approval M2023079), and written informed consent was obtained from each patient.
Assessment of Olfactory Function
Olfactory function was tested using the olfactory Visual Analogue Scale (VAS) score and the T&T olfactometer. The olfactory VAS score is a scale where the patient draws a rating of their symptoms on a scale of 0 to 10 representing the gradual worsening of symptoms. The T&T olfactometer 17 is an odorless filter paper with 1 cm of olfaction dipped in the front of the paper and placed in front of and below the nostrils of the subject. The mean of the patient’s detection thresholds for these 5 odors was calculated. According to the test results, they were divided into normal smell (≤1.0) and olfactory dysfunction (>1.0).
Blood and Tissue Eosinophils
Absolute values and percentages of serum eosinophils were detected by the Biochemical Laboratory of the Department of Laboratory Medicine of the Third Hospital of Peking University in patients after preoperative fasting. Nasal polyp tissues were analyzed by hematoxylin-eosin staining by the Pathology Laboratory of the Third Hospital of Peking University, and 5 high magnification fields of view (400×) were randomly selected in the sections, and eosinophil counts were carried out by 2 doctors, and the mean values were taken to calculate the results.
Nasal Secretion Type 2 Inflammatory Mediators’ Collection and Laboratory Analyses
A 2.0 × 1.0 × 0.5 cm gelatin sponge was placed into the middle nasal passages of both nasal cavities for 5 minutes, and nasal secretion was collected. We used the enzyme-linked immunosorbent assay (Dogesce, Beijing, China) to measure IL-4, IL-5, IL-13, IL-33, eotaxin-3, and periostin levels, according to the manufacturer’s protocols.
Surgical Procedures and Perioperative Care
The surgical protocol was ESS, fully opening the sinuses to create a common cavity. At the end of the procedure, a steroid-eluting stent (Xiangtong; Puyi Biotechnology, Shanghai, China) was implanted in the ethmoid sinus in the stent group. The stent contains 652 μg doses of corticosteroid mometasone furoate and is released for more than 30 days. The surgical cavity was filled with hemostatic sponges in both groups. The perioperative medication and postoperative treatment for all patients were essentially identical. Nasal glucocorticoid spray (budesonide nasal spray, 128 μg each time, once a day) and topical nasal saline rinse were given for 3 months after surgery. To prevent infections, systemic antibiotics were administered for 3 days after the operation, and no oral glucocorticoid medication was given in either group.
Statistical Analyses
Continuous variables were presented as mean ± standard deviation. Independent samples t-tests or paired t-tests were used to conduct the tests. Dichotomous variables were expressed as frequencies and percentages. Differences between groups were compared using the chi-square (χ²) test. Correlation analysis was performed using Spearman’s analysis to show the correlation between the data. All statistical analyses were performed using SPSS 26.0 (SPSS Inc.,Chicago, IL, USA) software. Statistically significant differences were considered as P < .05.
Results
Baseline Demographics and Laboratory Examination
A total of 59 patients with CRSwNP were included in this study, see Table 1. There were 30 patients in the stent group who received intraoperative steroid-eluting stent implantation and 29 patients in the control group treated without it. There were no significant differences in gender, age, disease duration, smoking history, surgical history, and concomitant diseases such as asthma, aspirin intolerance triad, and allergic rhinitis between the 2 groups. The preoperative LM scores, blood eosinophil percentage, tissue eosinophil percentage and absolute blood eosinophil count in the stent group and the control group were statistically indistinguishable (P > .05).
Baseline Demographics and Pre-ESS Disease Severity.
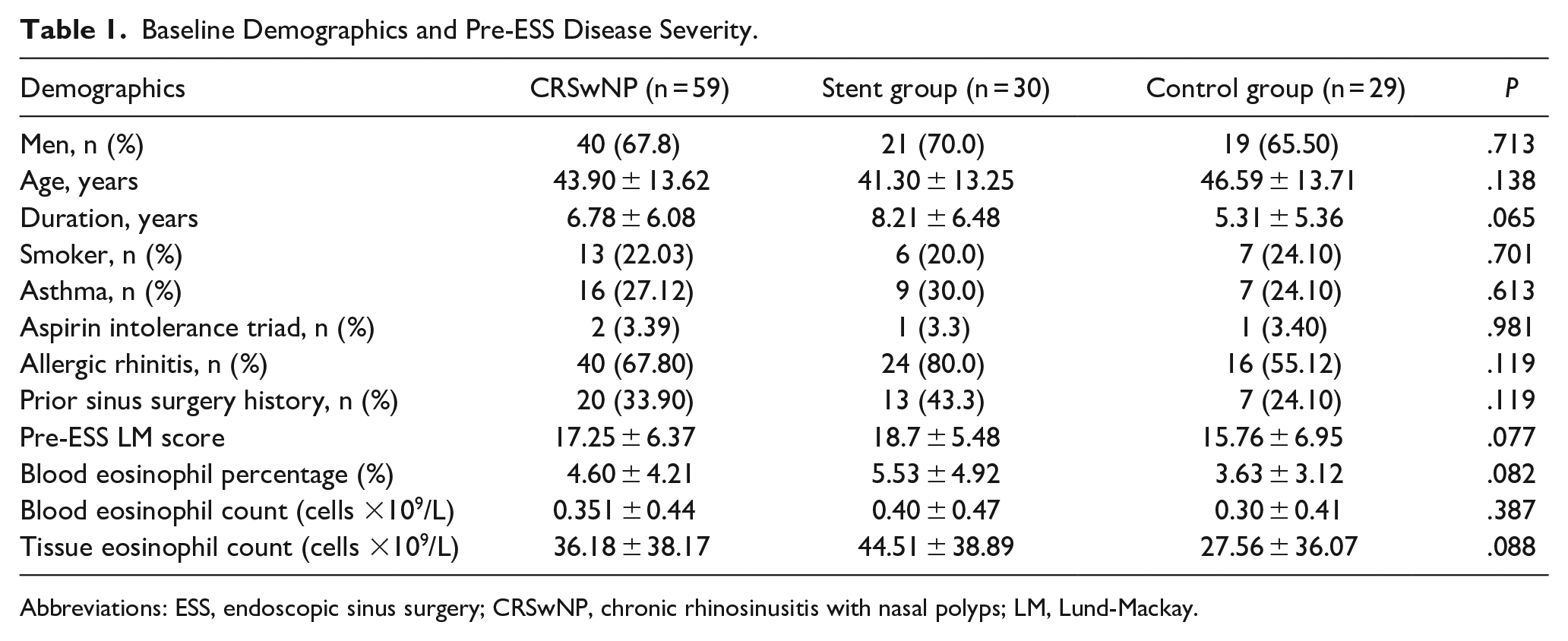
Abbreviations: ESS, endoscopic sinus surgery; CRSwNP, chronic rhinosinusitis with nasal polyps; LM, Lund-Mackay.
Clinical Characteristics of Olfactory Function, SNOT-22 Scores, and LK Scores
Preoperative olfactory VAS scores, T&T olfactometer scores, SNOT-22 scores, and LK scores were not significantly different between the stent group and control group (P > .05). However, postoperative olfactory VAS scores, T&T olfactometer scores, SNOT-22 scores, and LK scores were significantly lower in the stent group than those were in the control group (P < .01), as shown in Figure 2.
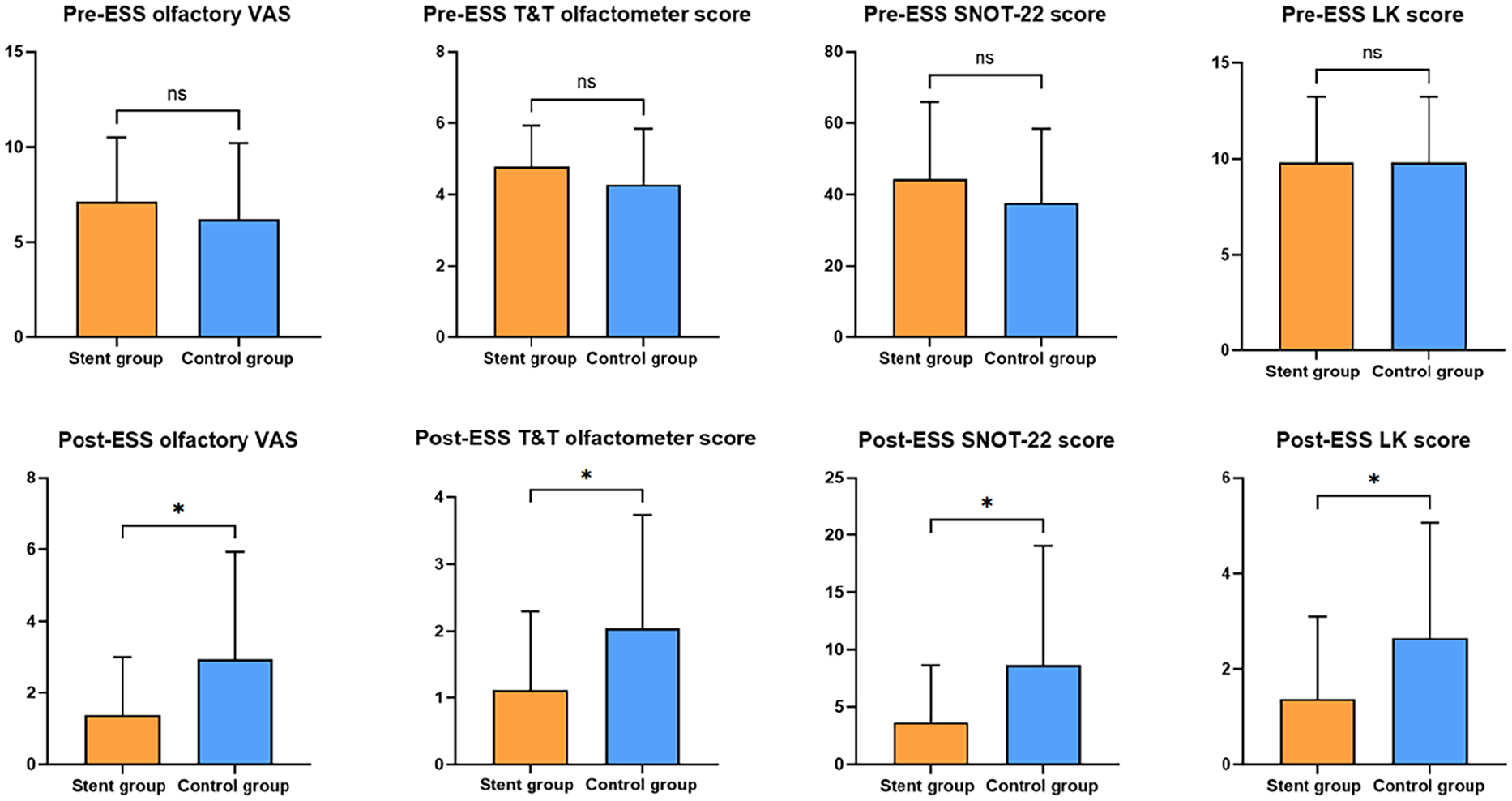
Pre-ESS and post-ESS olfactory Visual Analogue Scale (VAS), T&T olfactometer score, SNOT-22 scores, and Lund-Kennedy scores between the stent group and control group. ns, no significance; ESS, endoscopic sinus surgery.
Patients with CRSwNP had reduced postoperative olfactory VAS scores and reduced T&T olfactometer scores. Postoperative SNOT-22 scores and LK scores also decreased significantly in the stent and control groups, with statistically significant differences (P < .01), as shown in Figures 3 4.
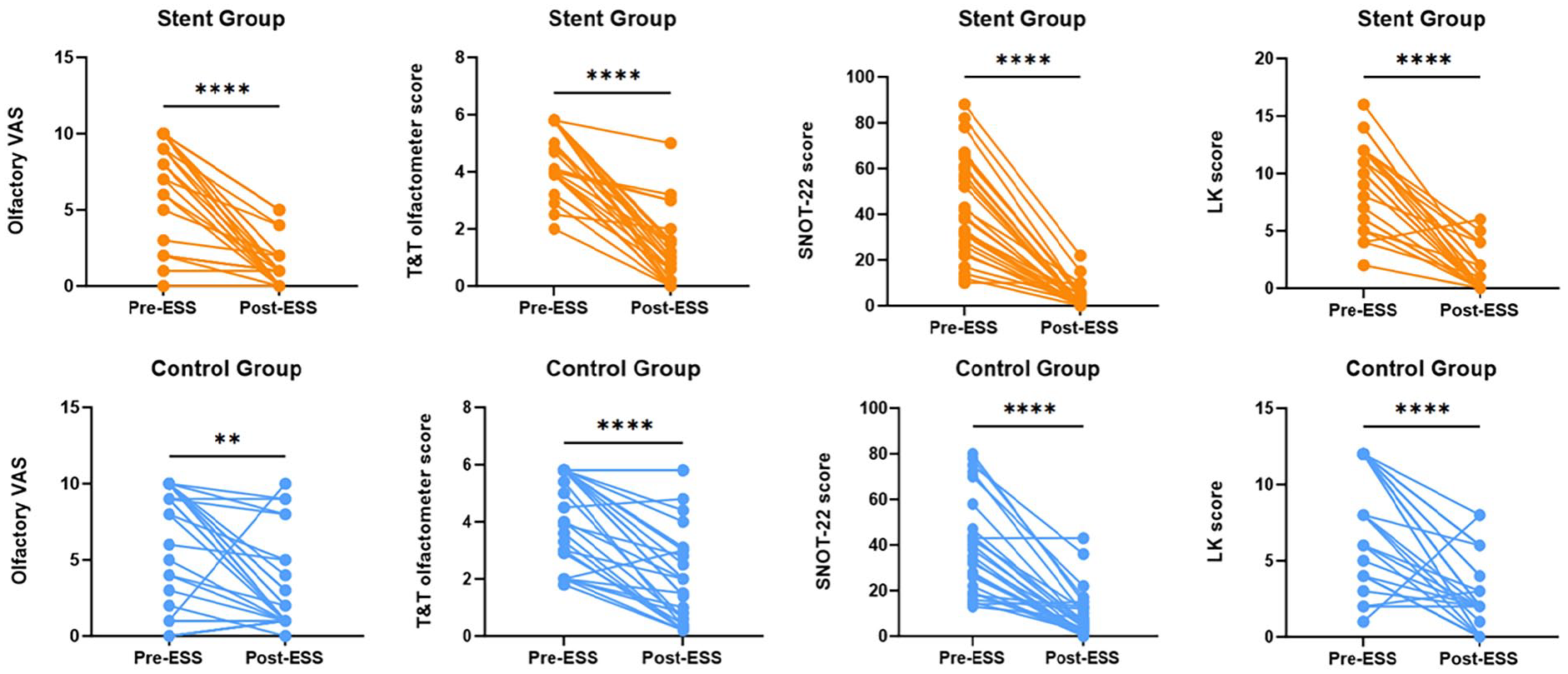
Pre-ESS and post-ESS olfactory Visual Analogue Scale (VAS), T&T olfactometer score, SNOT-22 scores, and Lund-Kennedy scores. ns, no significance; ESS, endoscopic sinus surgery.
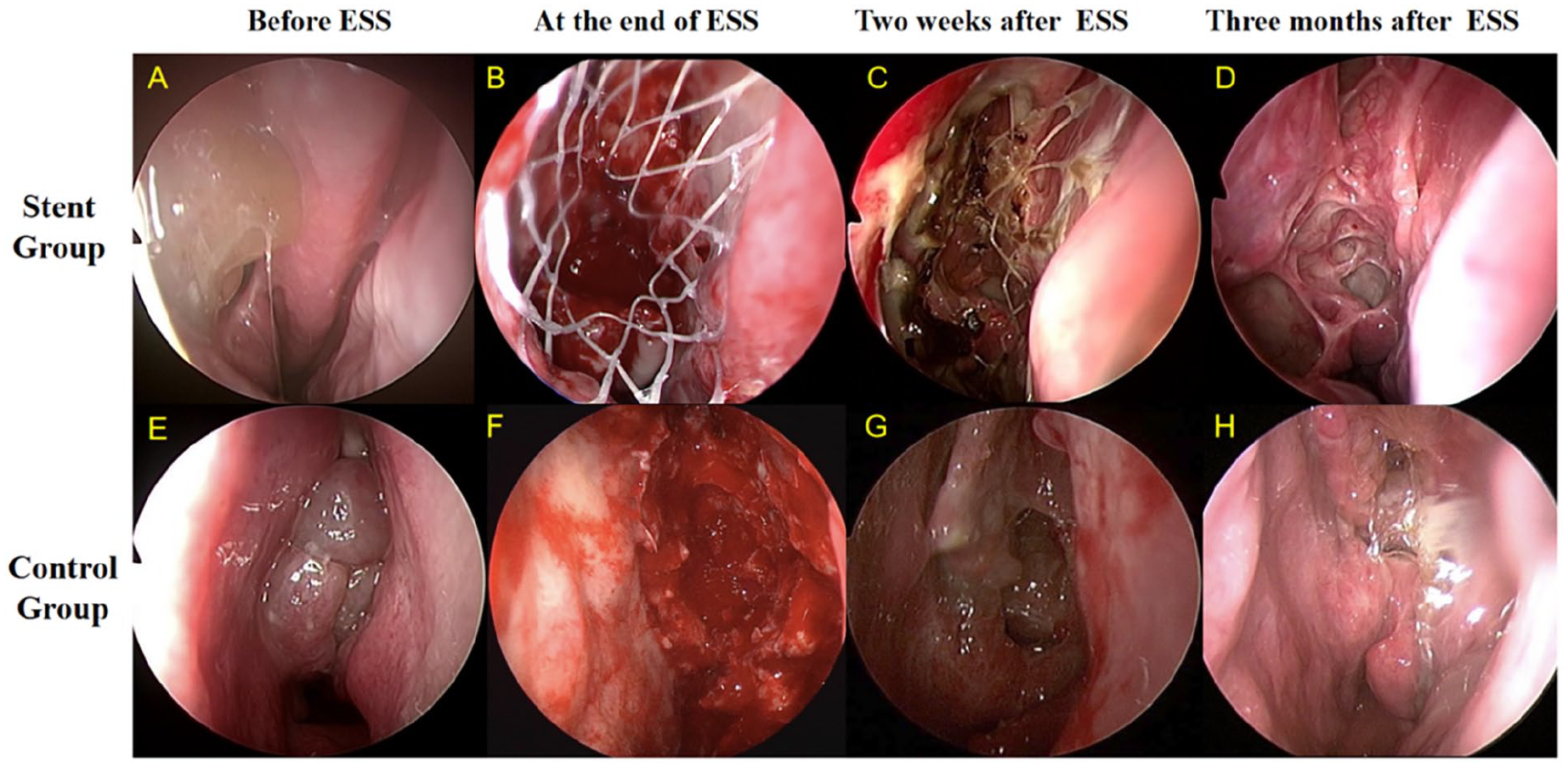
Nasal endoscopic images of the stent group and control group. (A, E) Shows preoperative nasal sinus lesions. (B, F) Shows the ethmoid sinuses after sinus endoscopy. (C, G) Shows ethmoid sinuses at week 2 postoperatively. (D, H) Shows ethmoid sinuses at month 3 postoperatively.
Type 2 Inflammatory Mediators’ Level
As shown in Figure 5, in the stent group, there was no difference between the 2 groups in IL-5, IL-13, IL-33, Eotaxin-3, and periostin, except for higher IL-4 levels in the preoperative period than in the control group. Postoperative IL-5, IL-13, and periostin concentrations were significantly lower in the stent group than those in the control group (P < .05). Type 2 inflammatory mediators were significantly lower in the CRSwNP patients after surgery, especially IL-4 and Eotaxin-3 (P < .05), but IL-33 was slightly elevated. In the stent group, postoperative IL-5, IL-13, and periostin decreased postoperatively; however, in the control group, postoperative IL-5, IL-13, and periostin concentrations were not significantly different before and after surgery (Figure 6).
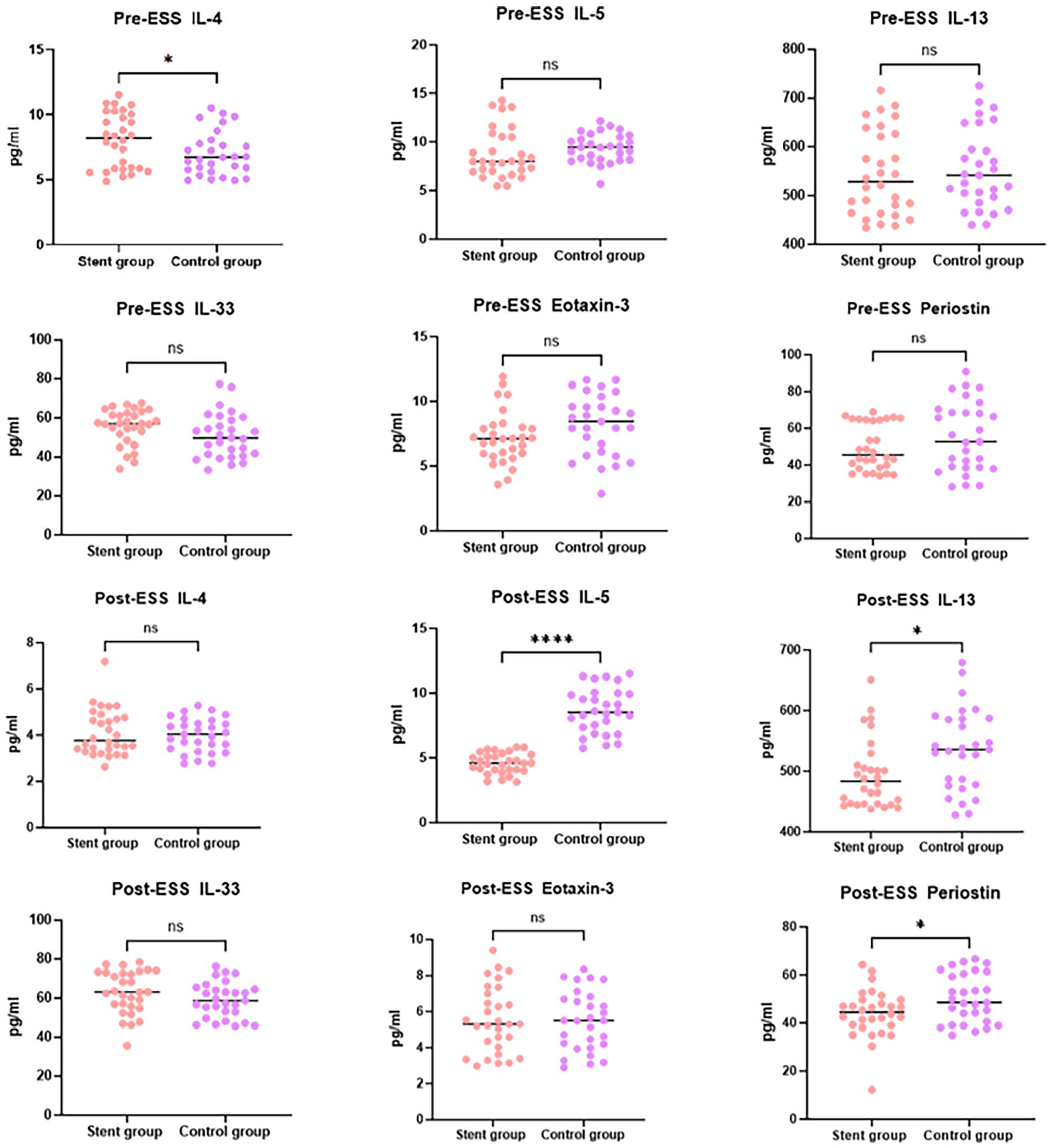
Comparison of type 2 inflammatory mediators between the stent group and control group. ESS, endoscopic sinus surgery; ns, no significance.
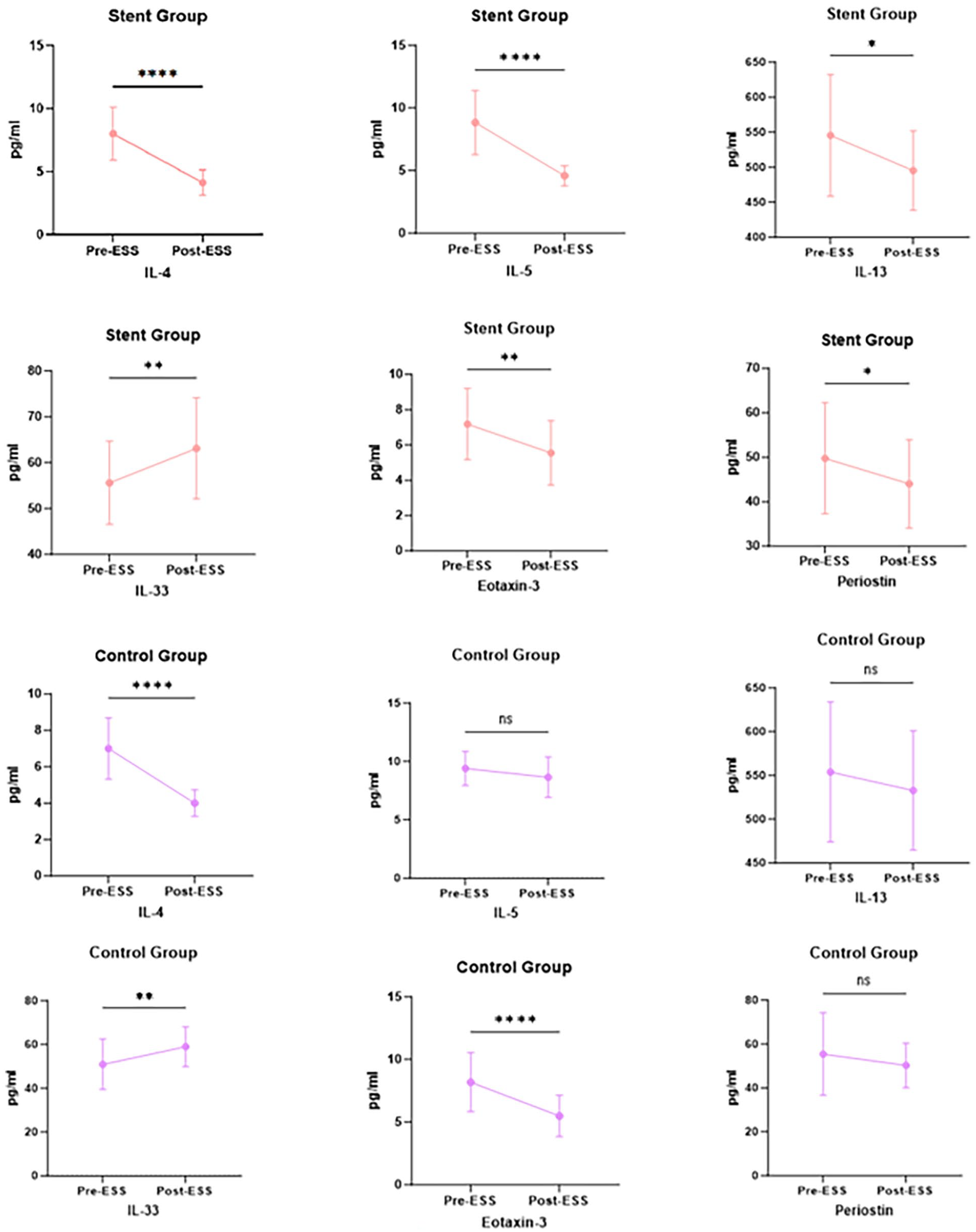
Comparison of type 2 inflammatory mediators before and after ESS. ESS, endoscopic sinus surgery; ns, no significance.
Correlation of Postoperative Olfactory Function with Type 2 Inflammatory Factors
Correlation analysis of postoperative olfactory function with type 2 inflammatory mediators revealed that postoperative olfactory VAS scores were strongly correlated with IL-5 and IL-13 (r = .496, P < .001 and r = .289, P = .026) and postoperative T&T olfactometer scores were strongly correlated with IL-5 and IL-13 (r = .553, P < .001 and r = .398, P = .002), as shown in Table 2.
Correlation of Postoperative Olfactory Function with Type 2 Inflammatory Mediators.
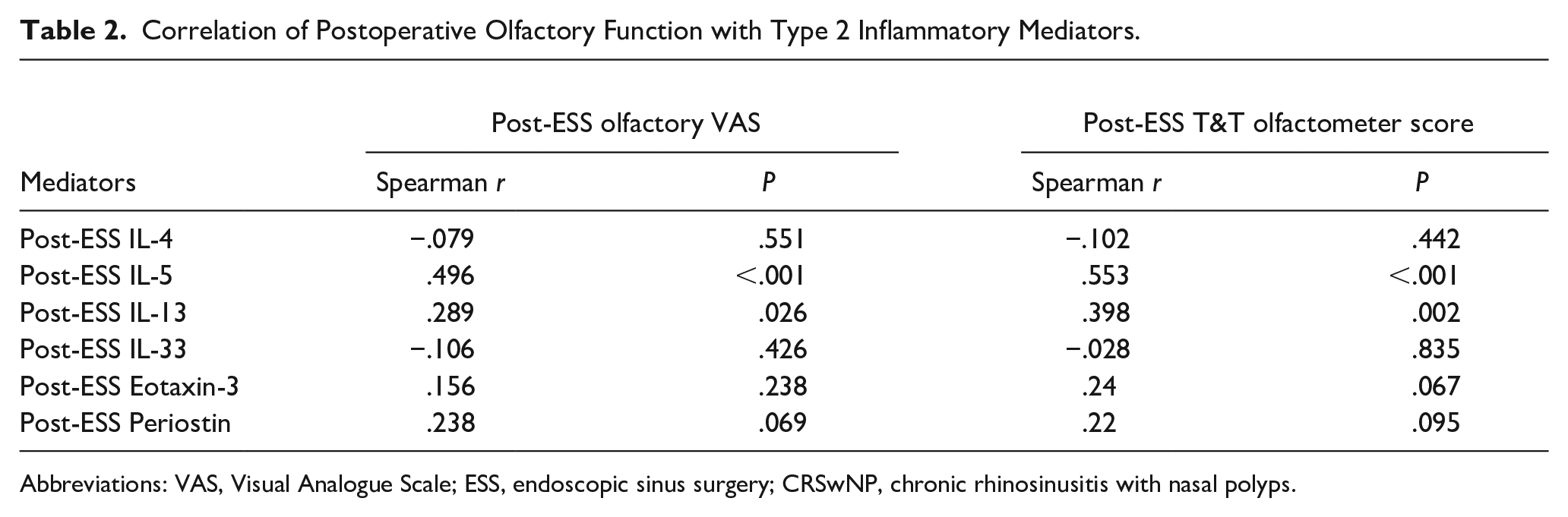
Abbreviations: VAS, Visual Analogue Scale; ESS, endoscopic sinus surgery; CRSwNP, chronic rhinosinusitis with nasal polyps.
Discussion
CRSwNP is a heterogeneous disease and patients with predominantly type 2 inflammation tend to be more symptomatic, especially with a high prevalence of olfactory loss, or poorly controlled by conventional medications and ESS treatments.18,19 Glucocorticoids effectively reduce type 2 inflammation, making them the primary treatment option for CRSwNP. 20 However, the side effects of systemic glucocorticoid administration can be significant. Nasal glucocorticoid therapy is also not entirely reliable in controlling efficacy due to certain limitations. ESS can significantly improve the clinical symptoms of patients in a short period; however, the persistence of inflammation and narrowing of the edema sinus ostium in the long term after the surgery affects the recovery of symptoms, such as worsening of nasal congestion, further decline in olfactory function, and even polyps recurring, which involves the efficacy of the surgery. 21 A recent multicenter randomized controlled trial demonstrated that glucocorticoid scaffolds were effective in reducing LK scores, sinus mucosal edema, and eosinophilic inflammation in patients with CRSwNP. 9 It has also been demonstrated that glucocorticoid stenting reduces symptoms and polyp recurrence in the early postoperative period compared to postoperative nasal packing (Nasopore pack) and dramatically reduces the incidence of re-surgical intervention. 22 Our study similarly found that in patients with glucocorticoid stenting a reduction in postoperative SNOT-22 scores, a significant improvement in clinical symptoms, and a reduction in nasal endoscopic LK scores on objective examination, stents significantly improve postoperative nasal edema, stenosis, and polyp recurrence in patients.
Olfactory dysfunction is particularly common in chronic sinusitis with nasal polyp subtypes and type 2 inflammatory endotypes predominantly.23,24 Glucocorticosteroids are the only first-line agents in the treatment of olfactory deficits in patients with CRS and contribute to the early recovery of olfactory function in patients. 25 In addition, surgical removal of polyps and reduction of the inflammatory load when medication is ineffective are also clinically relevant, but not all patients with CRSwNP have impaired recovery of olfactory function after surgery. 26 A study using tretinoin-containing gelatin sponge tamponade in the postoperative olfactory cleft area improves recovery of olfactory function in CRS. 27 It is suggested that postoperative combined local hormone therapy is an option to improve olfactory function. They are considering that glucocorticoid stents not only have local anti-inflammatory effects but also have sinus enlargement and long-term slow release of hormones, which might be beneficial for the improvement of olfactory function. In our study, the subjective olfactory VAS score and T&T olfactory score decreased after glucocorticoid stent implantation, and the olfactory function recovered better. It is suggested that topical glucocorticoids are one of the effective supplements for postoperative treatment of olfactory dysfunction, especially in perioperative periods. Continuous release of glucocorticoids can alleviate tissue edema and improve olfactory function in patients with CRSwNP, which is of great benefit to the improvement of early olfactory dysfunction.
A recent study has shown that steroid-eluting stents can effectively relieve local inflammatory states in the nasal cavity. 28 Type 2 inflammation is an important inflammatory endotype of CRS, always with higher relapse rates.29,30 IL-5 and IL-13 are important in driving type 2 inflammation; IL-13 recruits lymphocytes, eosinophils, and basophils for endothelial expression of adhesion molecules, and once eosinophils have been recruited into tissues, IL-5 promotes eosinophil survival and activation, stimulating mucosal edema and eosinophilic polypogenesis. 31 Therefore, reducing the IL-5 and IL-13 inflammatory status in the nasal mucosa is the root cause of the development of type 2 chronic sinusitis. Recent studies have found that postoperative IL-5 and IL-13 concentrations are significantly lower in patients with implanted glucocorticoid stents compared with preoperative levels, suggesting that the type 2 inflammatory load is reduced after local stenting with slow-release glucocorticoid anti-inflammation. 12 Our study similarly concluded that after treatment with steroid-eluting stents, patients had lower concentrations of IL-5 and IL-13 in nasal secretions than patients undergoing surgery alone and that there was a substantial postoperative decrease in the concentrations of IL-5 and IL-13 only in patients with stents. To investigate whether postoperative type 2 inflammatory mediators affect the recovery of olfactory function after surgery, the present study found for the first time that IL-5 and IL-13 play a crucial role in the recovery of postoperative olfaction based on the correlation between postoperative type 2 inflammatory mediators and postoperative olfactory function, and that high postoperative levels of IL-5 and IL-13 are a risk factor for the poor recovery of olfactory function after surgery; therefore, it is important to further reduce the inflammatory status of nasal IL-5 and IL-13 after surgery for the treatment of patients with CRSwNP. Therefore, further reduction of nasal IL-5 and IL-13 inflammation is important for the treatment of olfactory dysfunction in patients with CRSwNP.
IL-4 contributed to the differentiation of B cells into plasma cells that specifically produce IgE, which exacerbated a type 2 inflammatory state. 32 In our study, we found a decrease in IL-4 concentrations in patients who underwent endonasal sinus surgery, but no significant difference in postoperative IL-4 concentrations was found between the stent and control groups; further studies are still needed to determine whether local hormones are ineffective in lowering IL-4 and whether more targeted IL-4 antibodies are needed in the future. Periostin not only promotes allergen-induced recruitment of eosinophils to tissues but also increases eosinophil adhesion to fibronectin by 5- to 8-fold. 33 The concentration of periosteal proteins decreased significantly after surgical combined glucocorticoid stent implantation, which may be of possible significance in improving postoperative mucus formation and runny symptoms. In addition, Eotaxin-3 is an important regulator with high specificity for eosinophil chemotaxis. 34 In this study, we further attempted to observe the changes in Eotaxin-3 concentrations before and after surgery and found that Eotaxin-3 concentrations were reduced after surgery, demonstrating that surgery was beneficial in reducing Eotaxin-3-mediated inflammatory load, but was not associated with the use of glucocorticoid therapy or not.
This study was conducted only on patients with chronic sinusitis with nasal polyps, and patients with chronic sinusitis without nasal polyps were not included in this study. In addition, the follow-up time of this study was 3 months postoperatively, which may require longer clinical observation for some polyp recurrence and olfactory function changes. Therefore, for increasing the sample size, inclusion of a patient population without nasal polyps as a control, and observation of long-term efficacy is an improved part of the next study.
Conclusion
Our findings suggest that implantation of a steroid-eluting stent after ESS is an effective treatment for olfactory deficits in patients with CRSwNP, possibly related to the stent’s more effective reduction of local type 2 inflammatory mediators in the nasal cavity.
Footnotes
Authors’ Note
Informed consent was obtained from all individual participants included in the study.
Author Contributions
Qiang Zuo has made an equal contribution to this study with Zhang Zhidi. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China (Grant No. 82271168) and by Puyi (Shanghai) Biotechnology Co., Ltd.
Ethics Approval and Informed Consent
All procedures performed and data collected in this study adhered to the guidelines of the Declaration of Helsinki committees. The study was approved by the Ethics Committee of the Peking University Third Hospital (Ethics Committee Approval M2023079). Written consent was obtained from each patient.