
Abstract
Keywords
Idiopathic sudden sensorineural hearing loss (ISSNHL) refers to unexplained sensorineural hearing loss that occurs within 72 hours. 1 According to the 2015 guidelines, sudden deafness includes low-, high-, and flat-frequency hearing loss, and total deafness. 2 ISSNHL is one of the most difficult emergencies in the field of otolaryngology, with unknown causes and poor therapeutic outcomes. Sudden deafness is related to heredity, allergy, viral infection, vascular disease, 3 acquired diseases, or genetic tendencies.4,5 If left untreated, sudden deafness can lead to irreversible hearing loss.
The time from the onset of ISSNHL to the start of treatment for sudden deafness is closely related to the prognosis of ISSNHL2,6,7; the earlier the treatment, the better the prognosis of patients. However, in clinical practice, many patients delay treatment, resulting in a poor prognosis. This study aimed to analyze patient data and identify potential factors that affect the time to treatment (TT) in patients with ISSNHL.
Materials and Methods
General Materials
A total of 324 patients who were diagnosed with sudden deafness and treated in our department between September 2021 and May 2024 were included. The patients were self-referred to our department. They did not receive any diagnosis or treatment for ISSNHL at any other medical institution before coming to our outpatient and being admitted for treatment at our department after experiencing deafness. General patient information was collected. The exclusion criteria were as follows: (1) presence of ear diseases that could affect the diagnosis of ISSNHL, including conductive hearing loss, chronic otitis media, congenital malformation, or tumor; (2) severe organ dysfunction; and (3) incomplete clinical data. All patients were treated in accordance with the 2015 guidelines for sudden deafness. 2
Evaluation Indicators
A detailed medical history of baseline characteristics, such as sex, age, accompanying symptoms, comorbidities, medical insurance, and linear distance was collected. Linear distance refers to the straight-line distance from the patient’s current address (accurate to the community) to the outpatient hospital building. The selection of points and distance surveying relied on Baidu Maps. 8 Ear examination, otoscopy, acoustic impedance, otoacoustic emission, auditory brainstem response, and ear magnetic resonance imaging were performed to exclude other factors that might affect hearing. Hearing examinations performed on the same day measured air-conducted and bone-conducted pure tone average (PTA) at 0.125 0.25, 0.5, 1, 2, 4, and 8 kHz. The tests were performed by an audiologist in a standardized shielded room. Patients were classified into low-frequency descending (hearing loss at frequencies below 1000 Hz with a hearing loss of ≥20 dBHL), high-frequency descending (hearing loss at frequencies above 2000 Hz with hearing loss of at least 20 dBHL), flat-frequency descending (hearing loss at all frequencies, with an average hearing threshold of ≤80 dBHL), and total deafness (decrease in hearing at all frequencies, with an average hearing threshold of ≥81 dBHL) groups. The classification criteria were based on the 2015 guidelines. 2 The degree of hearing loss was assessed using the average hearing thresholds (0.25-4 kHz) for the frequencies causing damage in both ears before and after treatment. According to the 1997 WHO classification criteria for hearing impairment, based on the results of pure tone hearing threshold measurements, the PTA of affected ears at 4 frequencies (0.5, 1, 2, and 4 kHz) was calculated. The average improvement in the PTA was then calculated. The efficacy evaluation was either deemed effective or ineffective. An average PTA improvement of less than 15 dB compared with the pretreatment hearing threshold was considered ineffective, and ≥15 dB was considered effective. Patients’ first visit duration and various indicators were analyzed.
Statistical Methods
Count data are expressed as frequencies or percentages. Normal distribution is represented as mean ± standard error deviation. Based on the data representation, SPSS (version 20.0; IBM, Armonk, NY, USA) was used to analyze the research data, with a test standard of P = .05. According to the type of variables, T-test and the chi-squared test were used to examine the differences between the 2 groups. Pearson analysis is used to analyze correlations. A logistic analysis was used to identify influencing factors.
Results
Characteristics of Patients with Long TT
Research suggests that seeking medical attention for more than 7 days is a contributing factor for poor prognosis in cases of sudden deafness 9 ; therefore, we used 7 days as the boundary. Patients were divided into 2 groups based on their TT: the short-term (ST) group (disease duration ≤ 7 days) and the long-term (LT) group (disease duration >7 days). The results are summarized in Table 1.
Comparison Between ST and LT Groups.

Abbreviations: LT, long-term; ST, short-term.
Analysis of Factors Related to Patient’s TT
Correlation analysis was performed between the TT and average pretreatment hearing threshold, linear distance. The results showed a significant correlation (average pretreatment hearing threshold: Pearson correlation = −.136, P = .014, linear distance: Pearson correlation = .168, P = .002).
A binary logistic analysis of sex, pretreatment mean hearing threshold, and linear distance was performed based on the TT. The results showed that sex, pretreatment mean hearing threshold, and linear distance were independent factors influencing the duration of treatment, as shown in Table 2.
Logistic Analysis.
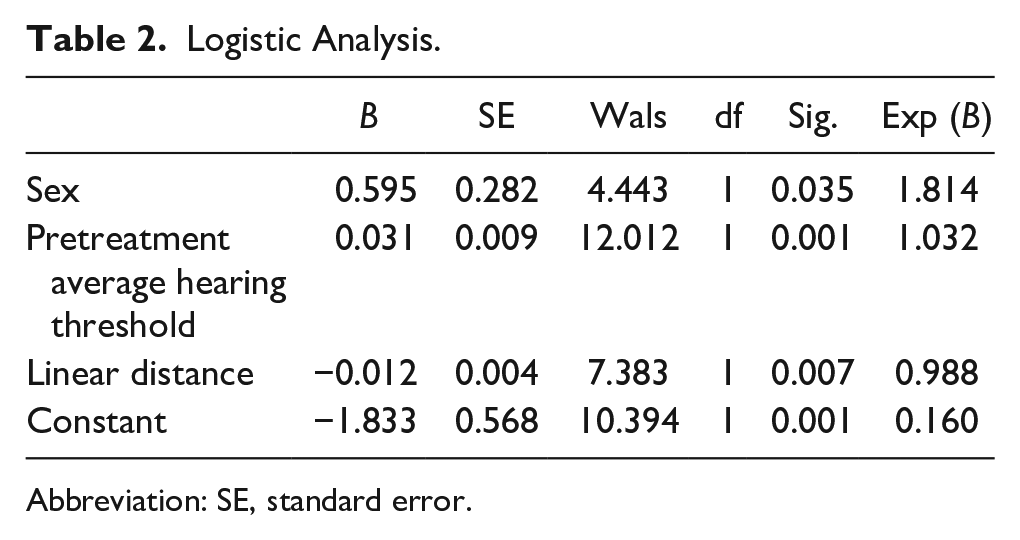
Abbreviation: SE, standard error.
Discussion
The time from the onset of ISSNHL to the start of treatment has been identified as a prognostic factor for hearing recovery, which is consistent with most literature.10 -12 Previous studies suggest that patients with ISSNHL should start treatment at least 7 days after onset.9,12
In this study, we found that the hearing thresholds of patients were significantly correlated with the TT. The average pretreatment hearing threshold was an independent factor influencing TT. The results also suggest that patients with total hearing loss have a relatively-short TT, and the 2 conclusions are interrelated. Severe hearing loss significantly affects daily life; therefore, a patient’s TT is also shortened. Patients with less hearing loss are relatively slow to seek medical treatment because of its minimal impact on daily life, resulting in delayed treatment and bad hearing outcomes.13,14
The proportion of female patients in the LT group was significantly higher than that in the ST group and was considered an independent prognostic factor. Previous studies have suggested sex-based differences in the morbidity of ISSNHL15 -17; however, hearing outcomes showed no sex-based difference. 14 The data collected in this study could not explain the reasons for the sex-related difference in TT, which requires further discussion.
It may be more meaningful to directly calculate the commuting time of patients to hospitals and clinics; however, relevant statistical data are lacking. We calculated and analyzed the linear distance between the patients’ current address and the hospital. The results showed that the linear distance is an independent factor influencing TT. Objectively, an increase in linear distance will lead to a longer commuting time. Patients who live near the hospital are more willing to seek medical advice.
Vertigo and tinnitus did not affect TT; however, they were not discussed separately in this study. Therefore, further studies should evaluate patients with varying degrees of tinnitus and dizziness to draw more accurate conclusions. Studies have shown that vertigo and tinnitus do not affect recovery from ISSNHL. The prognoses of deafness, tinnitus, and dizziness are related to the time of onset. Therefore, regardless of whether ISSNHL is accompanied by vertigo or tinnitus, it should be treated earlier for better recovery.18,19 Medical insurance coverage in the author’s area was relatively wide, with fewer nonmedical insurance cases, and no difference was observed in the medical insurance payment ratio between ST and LT. Diabetes hyperlipidemia and hypertension did not affect the patients’ TT.
Limitations
First, patients with a long TT usually fail to realize the exact time of onset, which might have affected the statistical results. Second, because this was a retrospective study, the sample size was small, and the researchers were unable to control for other interfering factors with high randomness. Third, considering the differences in transportation modes, linear distances might not accurately reflect the difficulty faced by patients seeking medical treatment at hospitals.
Conclusion
The average pretreatment hearing threshold and linear distance were independent risk factors for TT. Patients with mild hearing loss and those living at a long distance from the hospital had a longer TT. Female patients may tend to seek treatment later; however, this aspect needs to be evaluated in future studies. In clinical practice, it is necessary to study the scientific popularization of deafness and focus on key populations.
Footnotes
Author Contributions
F.Q. designed and performed the research, analyzed the data, and wrote the paper.
S.G. analyzed data and wrote the paper.
J.G. performed research and analyzed the data.
J.Q. designed and performed the research.
Data Availability Statement
The datasets in this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This study was approved by the Ethics Committee of Changzhou Third People’s Hospital: (02 A-A20230026).