
Abstract

Otitic hydrocephalus completes the list of intratemporal complications of otitis media in most every textbook. It is a rare disorder principally of children and adolescents characterized by signs of increased intracranial pressure during an episode of acute otitis media or mastoiditis. Patients present with symptoms of increased intracranial pressure including headache, drowsiness, photophobia, choking of the optic disk (papilledema), nuchal rigidity, vomiting, positive Kernig’s sign, and at times trigeminal pain, a sixth nerve palsy, or other focal symptoms. 1 If lumbar puncture is performed, cerebrospinal fluid (CSF) pressure is increased, but microbiologic cultures are negative, differentiating it from meningitis of otitic origin.
The neurologist, Sir Charles Symonds of the Royal National Throat, Nose and Ear Hospital, London, coined the term otitic hydrocephalus in 1931. After consulting upon several affected children and studying the earlier work of Heinrich Quinke (1896), the father of the lumber puncture, Symonds observed: “The writer is convinced that [this condition is] a not very uncommon complication of otitis media. There may occur a state of increased intracranial pressure due to the presence of an excess of normal cerebrospinal fluid. . . The writer suggests ‘otitic hydrocephalus,’ a title which implies no active process of inflammation . . . including fluid both within the ventricles and the subarachnoid space. The aetiology and pathology of the condition remain obscure—including either an excessive secretion from the choroid plexus or a defective absorption through the arachnoid villi.”
2
Shortly thereafter in 1936 Matthew Ersner and David Myers presented a series of cases of otitic hydrocephalus and proposed a mechanism for the phenomenon. Ersner was the first professor of otology at Temple University, and David Myers was his student and the future chairman of the department. They had previously advocated obliteration of the sigmoid sinus via a mastoidectomy approach to treat infectious lateral sinus thrombosis. 3 Two children treated in this way developed symptoms consistent with otitic hydrocephalus. Based on their clinical observations, they proposed that thrombosis of the lateral sinus obstructed venous outflow and impaired CSF absorption, resulting in increased intracranial pressure. It must be remembered that they were working in the pre-antibiotic era, operating with hammer and gouge. Cerebral venograms were not yet available—the first performed just a few years earlier by Antonio Egas Moniz in Portugal.
Their theory gained support in 1939 when W. James Gardner published a case series of 10 patients with otitic hydrocephalus. 4 Eight of them were found to have sinus thrombus confirmed either at autopsy or during mastoidectomy. Gardner also performed contrast encephalograms. He found no evidence of ventricular enlargement, indicating that the increased intracranial pressure was not due to interventricular obstruction. He recommended treatment of increased CSF pressure by serial lumbar puncture or subtemporal decompression.
The development of cerebral venous imaging techniques provided support for the vascular theory of otitic hydrocephalus. In 1994, Karen Jo Doyle, Derald Brackmann, and James House presented an adult case of otitic hydrocephalus. 5 Magnetic resonance venography demonstrated decreased venous flow from a partially obstructing clot in the right transverse and superior sagittal sinuses. They proposed that partial occlusion of the superior sagittal sinus led to obstruction of the arachnoid villi, impairing CSF absorption.
The incidences of both lateral sinus thrombosis and otitic hydrocephalus have dropped dramatically since the advent of effective antibiotic therapy for acute otitis media. Given its rarity, the mechanism of increased intracranial pressure remains uncertain. Recent series confirm that sagittal sinus thrombosis is not necessary to produce otitic hydrocephalus, but pseudotumor symptoms are more likely when there is extensive cerebral venous sinus involvement. 6 Symonds, Ersner and Myers were right (Figures 1 and 2).

Fundus photograph of papilledema of right eye from increased intracranial pressure (image courtesy of Yi Zhang, MD, PhD).
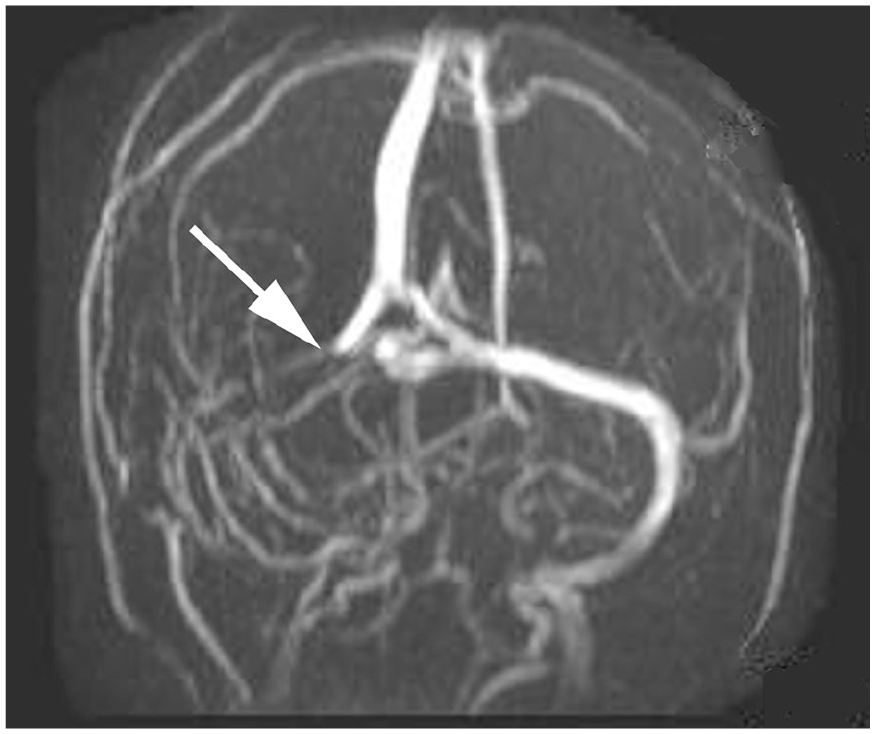
Coronal magnetic resonance venogram demonstrating absent flow in the occluded right transverse and sigmoid sinuses (arrow). Image courtesy of Vinay Shah, Radiopaedia.org, rID: 20045.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Level of Evidence
5—Expert opinion