
Abstract
Introduction
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a sinonasal inflammatory disease, with prevalence in general population of 1% to 4%, responsible for a significant impact on quality of life. 1 Several conditions are known to be associated with nasal polyps (NP), including asthma and aspirin hypersensitivity. 2 Endoscopic sinus surgery (ESS) has generally been reported to be a safe and effective procedure and is usually indicated in patients with CRSwNP refractory to maximal medical treatment. 3 However, with an overall polyps recurrence rate from 4% to 60% regardless of surgical technique and a large heterogeneity in recurrence rate within the group of CRSwNP, it is clear that not all clinical and immunologic factors associated with recurrence are known. 4
The main goals of this study were to evaluate ESS outcome in CRSwNP management and to identify independent predictive factors of recurrence.
Methods
This is a retrospective medical chart review including patients diagnosed with CRSwNP who underwent ESS, from January 2002 to December 2021, in our department. The diagnosis of CRSwNP was established by using the definition of EPOS 2020. 3 Surgery was offered to patients who failed to improve after a trial of maximal medical treatment, including topical long-term and systemic short-term steroids. Exclusion criteria included patients with unilateral disease, fungal sinusitis, antrochoanal polyps, concomitant benign, or malignant sinonasal tumors and those with a follow-up period inferior to 12 months. Revision surgery was offered to patients who had symptomatic NP recurrence, persistent for more than 6 months after medical treatment.
Charts were reviewed for the following variables age, sex, smoking status, occupational exposure, comorbidities (asthma, aspirin exacerbated respiratory disease, and allergic rhinitis), and previous sinus surgeries.
Allergic rhinitis (AR) was diagnosed based on typical symptoms following exposure to allergen complemented by results of total serum immunoglobulin E (IgE) concentration and/or positive skin prick tests. Asthma and aspirin-exacerbated respiratory disease (AERD) were diagnosed by a pneumologist. Hypersensitivity to aspirin was diagnosed based on history of adverse respiratory reactions triggered by aspirin and/or nonsteroidal anti-inflammatory drugs intake. AERD or Samter’s triad was defined by presence of NP with asthma and intolerance to inhibitors of cyclooxygenase-1 (COX-1).
The patients in our series were classified according to their past history and comorbidities (asthma, AERD, allergic rhinitis, etc. . .
Ear, nose, and throat (ENT) examination findings, computed tomography (CT) scan score, hematologic parameters, medical and surgical treatment, and histopathologic findings were also collected.
NP were classified endoscopically according to Jankowski classification. 5 Preoperative CT scan was classified according to the Lund–Mackay (LM) scoring system (range 0-24). 6 A complete blood cell count with differential cell count was performed in all patients, and eosinophil parameters were collected.
All patients underwent ESS under general anesthesia with endotracheal intubation, which included at least polypectomy. Frontal and sphenoid sinuses were approached according to CT and intraoperative findings. Middle turbinate was resected when it was extensively involved by NP disease and/or to obtain surgical access. After surgery, patients started a 7-day course of antibiotic and a regular saline douching. The first follow-up visit was scheduled 2 weeks after surgery for debridement and then patients started intranasal corticosteroid spray. Systemic corticosteroids were not prescribed perioperatively. Patients were evaluated 1, 3, and 6 months postoperatively and then every 6 months for at least 1 year.
Histological analysis showed tissue hypereosinophilia in every patient. None of the patients had undergone aspirin desensitization or monoclonal antibody therapy. Recurrence was defined as the presence of NP after surgery. The need for revision surgery was determined according to patients concerns and ENT examination.
Statistical Analysis
Categorical variables were described as counts or proportions and continue data were expressed as means (standard deviation). Chi-square test, Fischer’s exact test, ANOVA test, Shapiro–Wilk, and Kolmogorov–Smirnov normality tests with a 95% confidence interval were used to compare categorical variables.
In univariate analysis, we conducted a study of 13 variables that we considered possible risk factors for the occurrence of polyp recurrence in patients operated on in our department.
Multivariate logistic regression analysis was performed for the variables selected in the univariate study to obtain independent prognostic factor of recurrence and to assess their relative importance.
Statistical analysis was performed using statistical package for the Social Sciences® (version 26.0, SPSS®); P was considered statistically significant for values below .05.
Results
A total of 280 patients were enrolled in the study, which had a male gender predominance (male-to-female ratio of 1:11) and a mean age of 41.44 ± 14.25 years. The mean follow-up time was 2.7 ± 2.45 years. Descriptive clinical characteristics are listed in Table 1.
Descriptive Characteristics of Study Population (n = 280).
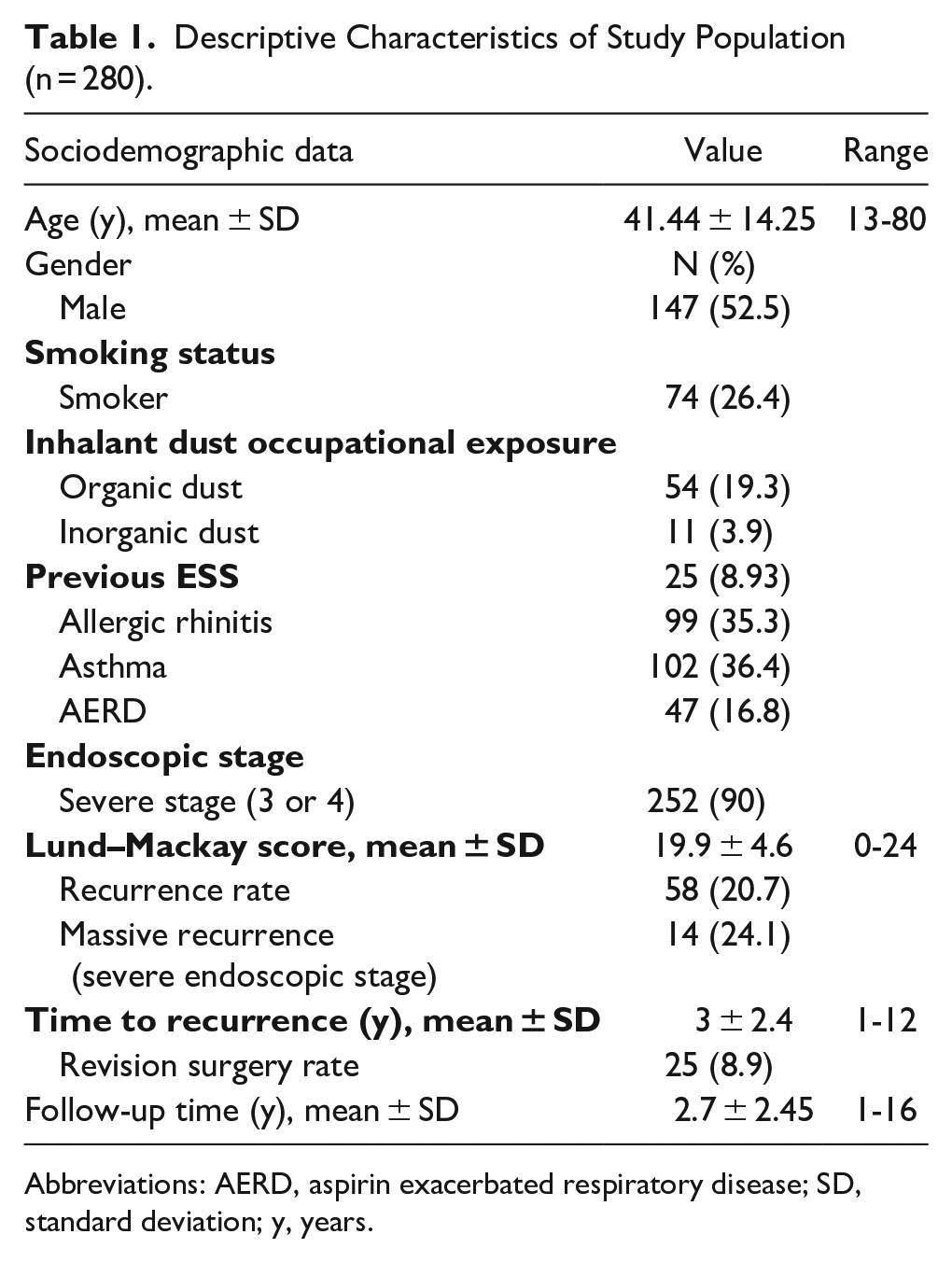
Abbreviations: AERD, aspirin exacerbated respiratory disease; SD, standard deviation; y, years.
Most patients were nonsmokers (n = 206, 73.6%). Regarding occupational exposure, 23.2% (n = 65) reported a positive dust inhalant exposure history. Asthma was the most common comorbidity, and it was present in 102 patients (36.4%). Samter’s triad was present in 16.8% of patients (n = 47), which represented 46.1% of the asthmatic group. Allergic rhinitis had a prevalence of 35.3% (n = 99). Endoscopic examination was performed in all cases, and the majority of the patients (90%) were staged as having stage 3 or 4 polyposis. All patients underwent preoperative CT scan. The mean LM score was 19.9 ± 4.6, and 73.2% of study population had a severe paranasal sinus obliteration (score 17-24). Patients with AERD had the most severe LM score (21.5/24) (Figure 1).
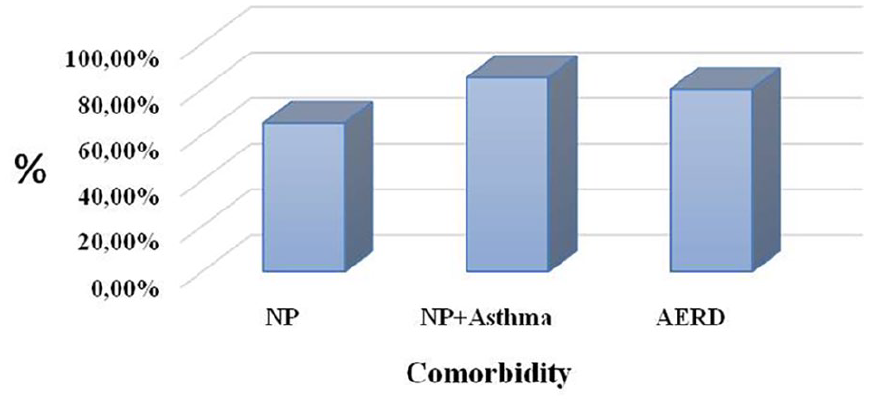
Distribution of severe LM score according to comorbidity. LM, Lund–Mackay.
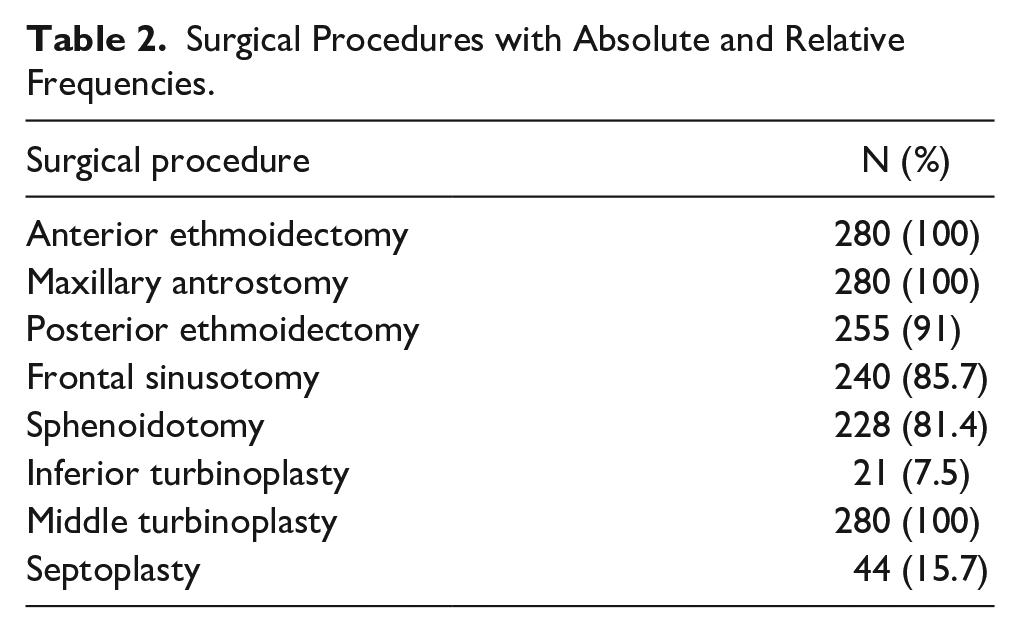
In our series, surgery was indicated for patients refractory to maximal medical treatment in 73.9% of cases. ESS was performed bilaterally in every case and always included the anterior ethmoidectomy, maxillary sinus antrostomy, followed in frequency by posterior ethmoidectomy associated with other procedures as needed (Table 2). In patients in whom frontal sinusotomy was necessary, a type I drainage (Draf I) was established by anterior ethmoidectomy, which identified the frontal recess, without touching its mucosa. Routine histopathologic evaluation confirmed the CRSwNP diagnosis and revealed elevated tissue eosinophilia in 152 patients (54.3%). Topical steroids were prescribed to all the patients after surgery, with a medication compliance rate of 81.4%.
Surgical Procedures with Absolute and Relative Frequencies.
Postoperative recurrence was diagnosed when endoscopic NP were detected. The main recurrence site was the ethmoid region. In the follow-up time, we found recurrence in 58 patients (20.7%), on average 3 ± 2.4 years after surgery. NP recurrence distribution in postoperative period was: 23 patients (39.6%) recurred in the first year, 12 patients (20.7%) in the second year, 8 patients (13.8%) in the third year, and 15 patients (25.9%) from fourth year after surgery. Recurrences of NP were massive in 14 cases (24.1%). Twenty-five patients required revision surgery, which represents 8.9% of the study population and 43.1% of patients who had recurrence of nasal polyposis. The influence of prognostic factors on recurrence is described in Table 3.
Analysis of Predictive Factors of Recurrence.
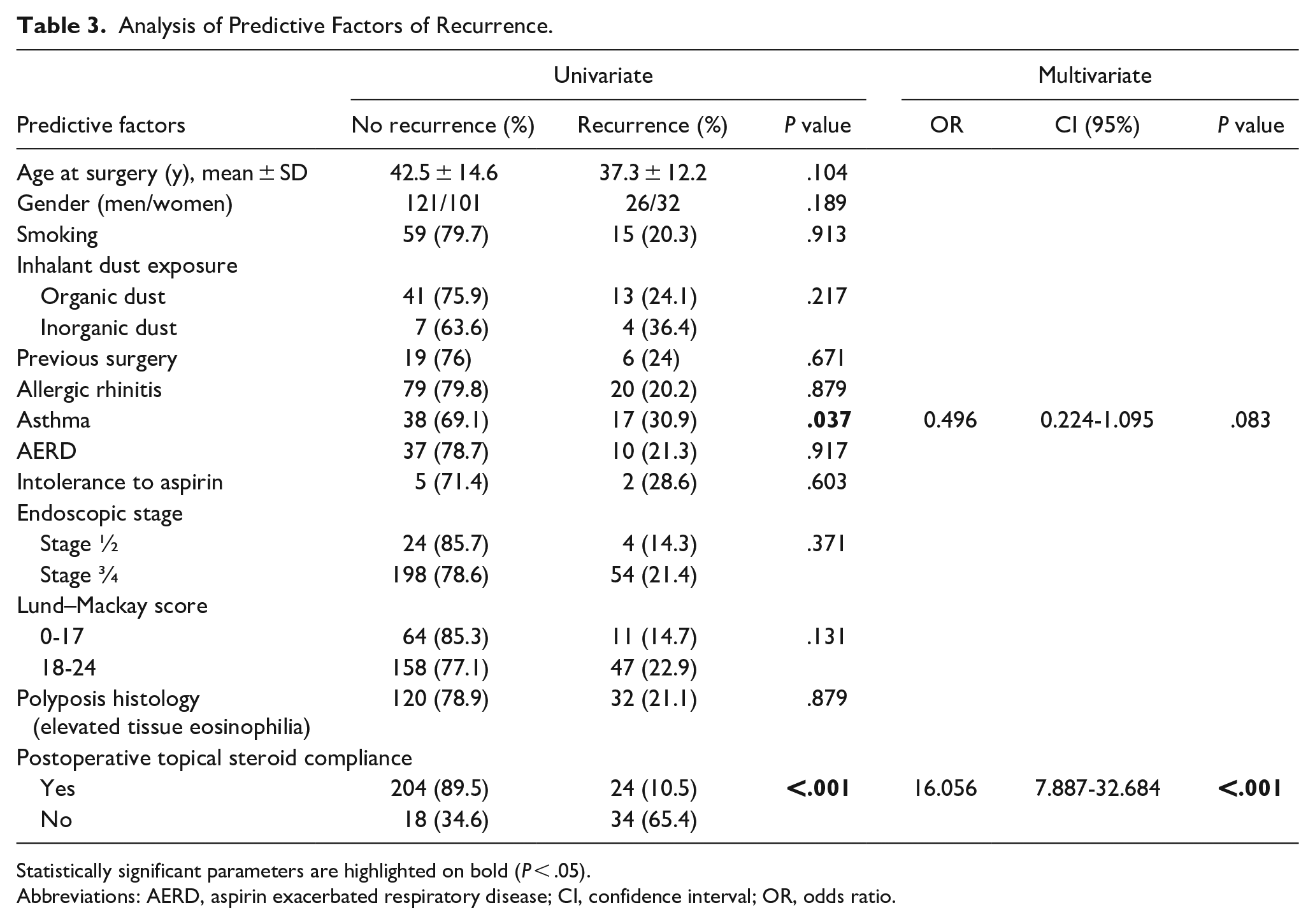
Statistically significant parameters are highlighted on bold (P < .05).
Abbreviations: AERD, aspirin exacerbated respiratory disease; CI, confidence interval; OR, odds ratio.
In univariate analysis, the recurrence rate was significantly related to factors such as asthma status (asthmatic, P = .037) and postoperative topical steroid compliance (P < .001). The other variables did not show any statistically significant relationship with surgical success. A stepwise binary logistic regression model was developed on these significant prognostic factors, to assess independent determinants of nasal polyposis recurrence after ESS and its relative importance. After preliminary screening, final modeling for polyp recurrence found that patients who were noncompliant at daily topical steroids had 16,056 times greater chance of NP recurrence compared with patients who were compliant.
Discussion
This article aimed to evaluate ESS outcome in CRSwNP management and to identify predictive factors of recurrence.
The recurrence rate was of 20.7% over 12 years follow-up and a need of reintervention of 8.9%. A 2006 systematic review about ESS effectiveness in the treatment of CRSwNP found a recurrence rate between 4% and 60%, with a median value of 20% across all evaluated studies and a need for revision surgery in the range of 3% to 42%, with a median of 6%. 7 Recently, some authors demonstrated that, over a long-term period of follow-up, about 80% of patients with CRSwNP experienced recurrence and about 37% needed revision surgery. 4 Although we found NP recurrence in up to 4 years after surgery, more than 70% of them were found in the first 3 years of follow-up. Bassiuoni and Wormald reported similar results, with 79% and 95% of recurrences in the first 2 and 3 postoperative years, respectively. 8
There are wide differences in the published literature about prognostic factors that can identify the most susceptible patients to CRSwNP recurrence. This fact can be explained by different methodologies and types of studies used, and the type of statistical analysis performed.
Some authors have studied the age of patients as a factor that may influence postoperative endoscopic outcomes.
For Kim et al, 9 the adult population showed better postoperative endoscopic results. These results were explained by a decline in neutrophil inflammation with age.
For Lee and Lee, 10 the endoscopic findings were worst in the pediatric group, whereas the geriatric group showed the best results.
In fact, pediatric patients generally have lower immunity than do adult patients. They also have a poor understanding of their disease and show lower compliance with medication and postoperative management. 11 In our series, we did not found association between age and recurrence in patients with CRSwNP.
According to Meng et al, 12 gender was not related to NP recurrence. About smoking, authors show that there was no significant difference between smokers and nonsmokers postoperative endoscopy. 13 Ours results are in accordance with these studies.
The association of asthma and NP has been widely described in literature. 2 NP occurs in 7% to 14% of all asthmatic patients, whereas asthma is reported in 26% to 48% of patients with NP. 3 Asthma history was present in 36.4% of our study population, a similar rate to previous reports.
In the literature, asthma is well-known factor associated with polyps recurrence.4,12,14 Our study shows that presence of asthma was a significative factor related to recurrence in univariate analysis (P = .037). However, this factor was not retained according to the multivariate analysis model, may be due to the reduced number of cases.
A subset of patients with NP and asthma develop upper and/or lower airway reaction following intake of a COX-1 inhibitor. Such patients have AERD also known as Samter’s triad or Fernand Widal syndrome. 15 We found AERD in 16.8% of our study population, which is in agreement with previous studies that report an incidence of 8% to 26%.16,17
Previous studies revealed a higher NP CT score on patients with asthma or Widal syndrome.2,18 Some authors identified severe CT score as a risk factor to recurrence. 19 On the other hand, other authors did not found any relation between CT score and surgical outcome. 12 In our study, patients with severe paranasal sinus opacification was not a significative factor related to recurrence of NP (P = .131).
Prior findings suggested that recurrence rates are higher in patients with asthma alone or with Samter’s triad. Mendelsohn et al 20 described that patients with asthma present a polyps recurrence rate at 5 years of 45% and a revision surgery rate at 5 years of 25%, whereas patients with Samter’s triad present a polyps recurrence rate at 5 years of 90% and a revision surgery rate of 37%.
Furthermore, other studies have demonstrated that aspirin intolerance seemed significantly more frequent in recurrent CRSwNP versus non-recurrent CRSwNP. 4
The role of atopy in chronic rhinosinusitis is unclear. It is particularly controversial in chronic rhinosinusitis with NP 21 Previous studies have reported NP to occur more frequently in non-atopic patients. 22 Some authors4,12,21 show that allergy is not a determinant of treatment failure and recurrence, whereas others suggest that it is related with poor prognosis and increased risk of recurrence. 11 By our data, AR had a prevalence of 35.3%, and it was not a predictive factor related for recurrence.
Occupational exposures are considered a risk factor for the disease recurrence by several authors. Thus, avoidance of dust can be an important measure to prevent disease progression and recurrence after treatment. 23 Our results evidence a positive occupational dust exposure in 23.2%, with most patients being exposed to organic dust. Despite a high rate of recurrence, occupational exposure was not a predictive factor of recurrence.
According to many studies, history of previous ESS and higher preoperative nasal polyposis endoscopy scores were found to associate with polyp recurrence.12,24 This is in contrast to our study that has not identified these factors as risk factors for recurrence.
Regarding polyposis histology, it has been shown that eosinophilic type of CRSwNP is an independent prognostic significance in relation to recurrent polyposis.4,11 On the contrary, other authors stated that the degree of eosinophilia in CRSwNP did not differ significantly between patients showing recurrence and those not showing recurrence. 25 By our data, there was no role for elevated tissue eosinophilia as predictive factor for recurrence.
A more extensive surgical approach, including extended sinusotomy, may be an important tool to combat polyp recurrence. Jankowski et al 26 found that nasalization of the ethmoids was associated with lesser polyp recurrence compared to functional ethmoidectomy. Moreover, there is evidence that partial resection of middle turbinate decreased the opportunity of recurrence of disease and resulted in significantly better symptomatic improvements. 27 In our series, all patients had a bilateral radical ethmoidectomy and middle turbinate resection.
Data from randomized trials indicate that postoperative use of intranasal glucocorticoids improves symptom control and endoscopic scores and reduces the need for rescue therapy with systemic corticosteroids.28,29 This ongoing medical therapy is therefore considered to be an essential part of surgical management, and patients must be counseled appropriately before and after surgery. A meta-analysis showed that risk of recurrence is reduced by postoperative corticosteroids in CRSwNP (P = .01). 28
In our center, CRSwNP postoperative protocol treatment includes systematically daily and long-term administration of topical corticoid spray. Finally, we found that no compliance with postoperative topical corticosteroid use was the most significative factor related to recurrence. The multivariate model showed that only this factor retained an independent prognostic significance in relation to recurrent polyposis (P < .001). This group of patients had 16 times the odds of recurrence compared to other patients.
In last years, many attempts were made to recognize CRSwNP phenotypes focusing on identifying relevant key pathogenic molecules. In fact, even if different subtypes of CRSwNP present with a similar clinical picture, they probably include variable histopathologic mechanisms of polyps formation. But basing on present knowledge about CRSwNP, the list of particular endotypes has not been proposed yet. Some of the endotypes proposed are, for example, IL-5 and IgE endotypes.4,30 From results of Davide et al, 4 high IL-5 expression in CRSwNP correlate with higher rate of polyps recurrence, whereas neutrophilic and lymphocytic infiltration, as well as IL-8 expression do not correlate with polyps recurrence.
This is a retrospective study based on medical charts with a potential information bias. The main strengths of the present study lie in the high number of cases examined and the homogeneous series of patients considered: their surgical treatments were performed consecutively by the same surgeon, with the same surgical experience; their histological diagnosis was established by the same laboratory; and postoperative medical treatment was standardized. The main weakness of the study, on the other hand, concerns significative missing data. More clinical investigations and future prospective studies are needed to support our findings. Risk factors for polyp recurrence were examined in all our patients. Our patients had at least 1 anterior and posterior ethmoidectomy and 1 maxillary antrotomy, as well as 1 mid-turbinectomy. Regarding the influence of the surgical procedure on disease recurrence, this factor was not studied, which constitutes a second limitation for our study. However, most authors analyze the impact of a functional or radical ethmoidectomy on disease recurrence and not the extent of the procedure performed. 26
Conclusion
From our results, we can conclude that Surgery plus continued postoperative medical management significantly improved surgical outcome. The findings of this study provide the opportunity to improve our ability to predict the prognosis of the surgical intervention, although it is still needed to explore the optimal predictor of outcome in CRSwNP.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This retrospective study does not pose any ethical problem.