
Abstract
Keywords
Introduction
Chronic rhinosinusitis (CRS) is a chronic inflammatory condition of the sinus mucosa characterized by a variety of phenotypes and endotypes. Clinical manifestations involve sinus pressure, nasal congestion, rhinorrhea, and reduced olfactory function, persisting for over 12 weeks.1,2 CRS, one of the most prevalent chronic diseases, is primarily treated with the goals of suppressing infection, reducing sinus inflammation, and maintaining effective sinus drainage. CRS is usually treated medically and surgically. 3 Endoscopic sinus surgery has consistently demonstrated improvements in quality of life, olfactory function, and asthma control while reducing the need for systemic antibiotics in patients with CRS. 4 Functional endoscopic sinus surgery (FESS) has emerged as a firmly established treatment option for patients with CRS. 5 However, postoperative complications, including recurrent sinusitis, are common. 6 Therefore, macrolide antibiotics are commonly applied to prevent infection and inflammation after FESS for CRS. 7
Antibiotics perform an available part in the treatment of CRS and can be employed to weaken the infectious component of CRS. Macrolide antibiotics, such as clarithromycin (CAM), have been widely utilized for their anti-inflammatory and immunomodulatory properties in managing CRS, especially post-FESS. CAM, one of the macrolide antibiotics, is considered a suitable choice for the treatment of CRS due to its unique immunopathologic profile. Several studies have demonstrated that long-term use of CAM is effective and well-tolerated in the treatment of CRS.3,8 Current evidence indicates that intranasal glucocorticosteroids have potent local anti-inflammatory effects, minimal systemic impact, and relatively mild side effects. Glucocorticoids, such as fluticasone propionate (FP), restrain gene expression of markers that contribute to the production and support of inflammatory processes. Glucocorticoids are employed as topical agents in upper respiratory tract disorders with different inflammatory mechanisms, such as acute sinusitis and CRS with or without nasal polyps. 9 Although subsequent anti-inflammatory therapy is crucial for CRS patients after FESS, few studies have explored the combined use of CAM and FP in the cohort. Therefore, the study aims to evaluate the efficacy of CAM combined with FP in CRS patients after FESS, focusing on nasal function, nasal MCT function, and serum inflammatory markers.
Materials and Methods
Ethics Statement
The study is approved by the Ethics Committee of our hospital, and the patients have voluntarily signed the consent form.
Research Subjects
The 96 patients with CRS admitted to our hospital from August 2019 to December 2021 were considered as subjects, and the patients were randomly assigned to either the control group (FESS treatment) or the study group (FESS treatment + CAM and FP), with 48 cases in each group. Inclusion criteria included patients diagnosed with CRS 10 by computed tomography, nasal endoscopy, and clinical symptom; age >18 years; disease duration of ≥ 6 months; no previous history of nasal surgery; and good compliance. Exclusion criteria included patients with nasopharyngeal malignancies, asthma, allergic rhinitis, sleep apnea, autoimmune diseases, malignancies, organ insufficiency, systemic infections, drug allergies, pregnancy, or breastfeeding.
Methods
Patients in the control group received the treatment of FESS. Patients were placed in the supine position, administered local anesthesia, and operated on using functional endoscopy with video assistance. The Messer Klinger technique was applied to perform the surgery according to the specific conditions of the patient’s lesions. In patients with maxillary sinusitis, the surgery focused on removing the terminal portion of the uncinate process and completely exposing the maxillary sinus ostium; while in patients with frontal sinusitis or sphenoid sinusitis, the surgery focused on the removal of the head and body of the uncinate process. The maxillary, frontal, and ethmoid cells were dilated through their natural openings when the anterior and posterior ethmoid and sphenoid sinuses were affected. In patients with nasal polyps or turbinate hypertrophy that interfered with the surgical procedure, the hyperplastic tissue could be resected first with a cutting suction. Patients with structural anomalies such as deviated septum and enlarged turbinates were intervened with deviated septum correction. Normal sinus mucosa was preserved as much as possible during surgery, and the postoperative cavity was packed with a gelatin sponge or petroleum jelly gauze to stop bleeding, which was taken out 2 to 3 days postoperatively. Patients were given routine interventions such as nasal cleaning and anti-infection prophylaxis, and saline was applied to spray and clean the patient’s nose in the postoperative period, 1 spray/time, 2 times/day.
The study group was treated with CAM combined with FP on top of the control group. FESS measures were consistent with the control group. CAM capsule (Specification: 0.25 g/capsule; Manufacturer: Jiangsu Xiangrui Pharmaceutical Co, Ltd, Jiangsu, China; State Drug Administration: H20065091) was taken orally, 1 capsule/day. Based on the patient’s symptoms, the dosage could be increased to 2 capsules/day, 1 capsule every 12 hours. FP inhalation aerosol (Specification: 125 μg × 60 sprays; Manufacturer: Glaxo Wellcome SA, England; State Drug Administration: H20130190) was administered with the following precaution: the nasal septum was not sprayed directly. The right nostril was sprayed using the left hand, and the left nostril was sprayed using the right hand to ensure proper application. Two sprays were needed for each side of the nasal cavity, 1 time/day, 200 μg/day, and the dose may be changed to 2 times/day, once in the morning and once in the evening, based on the patient’s symptoms.
Both groups underwent continuous spray treatment for 1 month, and the therapeutic effects were assessed at the conclusion of the treatment.
Observation Indicators
Clinical data
The study gathered the clinical data of all patients, such as age, gender, disease duration, and lesion location.
Clinical efficacy
The clinical effectiveness of the patients was assessed after 1 month of treatment.
Completely effective
The patients’ sinus opening was fully open with no cysts, edema, or purulent secretion seen in nasal endoscopy, and all the clinical symptoms completely resolved.
Partially effective
The patient’s sinus opening was good, but there was some growth of cysts, mild edema, and a small amount of purulent secretion in nasal endoscopy, with partial improvement in clinical symptoms.
Ineffective
The patients’ nasal endoscopy showed severe edema, a large amount of purulent secretion, and no significant improvement in clinical symptoms.
Total effective rate = (number of completely effective cases + number of partially effective cases)/total number of cases × 100%.
Symptom scores
Before cure and after a month of cure, patients’ symptom improvement was analyzed by adopting a visual analog scale, containing nasal congestion, runny nose, sneezing, dizziness, and headache. Patients were rated on a scale from 0 to 10, where 0 indicated no discomfort and 10 indicated severe discomfort; higher scores reflected more severe symptoms.
Nasal function
Before treatment and after 1 month of treatment, the nasal ventilation function indices of patients were determined through an anterior nasal pressure gauge (Master PF-10 model, Master Electronics lnc. , California, USA), involving nasal airway resistance (NAR), nasal cavity volume (NCV), nasal minimal cross-sectional area (NMCA), and distance of the minimal cross-sectional area to the nostril (DCAN). T&T olfactory test method 11 was applied to examine the patients’ olfactory function, which was performed in a well-ventilated environment free of background odors. Floral, fruity, rotten, fecal, and burnt odors were each separated into 8 concentrations, and the concentrations were scored on a scale from −2 to 5, with values increasing from low to high; those who still could not be tested or confirmed at the highest concentration were scored as 6. The average score of the 5 olfactory elements was used as the final score, with higher scores indicating poorer olfactory function.
Nasal MCT function
Before therapy and after a month of therapy, the patient’s nasal MCT function was measured by the saccharin test. The patients fasted from sweet food 2 hours before the measurement, took an upright sitting position, kept their head level, breathed calmly, and blew out the excess secretions in the nasal cavity. A saccharin pellet of approximately 0.8 mm in diameter was placed on the inner edge of the patient’s inferior turbinate, and a stopwatch timer was started after placement. Every 30 seconds, the patient was extended to swallow once. The time from placing the saccharin granules until the patient first detected sweetness was recorded as the mucociliary transport time (MTT). The time from the detection of sweetness, until the sensation disappeared, was recorded as the mucociliary clearance (MCC) time. A soft sterile cotton swab was inserted into the posterior pharyngeal wall through the nostril, and the distance from the setting of saccharin to the posterior pharyngeal wall was recorded as the distance of saccharin transported by the nasal cilia. Nasal MCC = MCT time/nasal cilia transport distance of saccharin × 100%. Nasal mucociliary transport rate (MTR) = nasal cilia transport distance of saccharin/MTT.
Serum inflammatory marker levels
Before treatment and after 1 month of treatment, 5 mL of fasting venous blood was drawn from patients, centrifuged at 3000 rpm for 10 minutes, and the supernatant was separated and put in a low-temperature refrigerator for assessment. Enzyme-linked immunosorbent assay was employed to determine patients’ serum inflammatory marker levels, containing interleukin (IL)-6, IL-8, tumor necrosis factor-α (TNF-α), and procalcitonin (PCT).
Occurrence of adverse reactions
The occurrence of adverse reactions such as nosebleeds, nasal adhesion, nasal dryness, nausea, and vomiting in patients was kept a record after surgery.
Statistics
SPSS 26.0 software (IBM Corp, Armonk, NY, USA) and GraphPad Prism 8.01 software (Graph Pad Inc, La Jolla, CA, USA) were used for data analysis. Measurement data were indicated as mean ± standard deviation ± s), and paired-samples t-test was used before and after treatment between groups, and independent-samples t-test was employed for separate comparisons between groups. Numeration data were presented as case numbers and percentages (%), and comparisons were made utilizing the χ2 test or Fisher’s exact test. P values below .05 were considered significant.
Results
Clinical Data
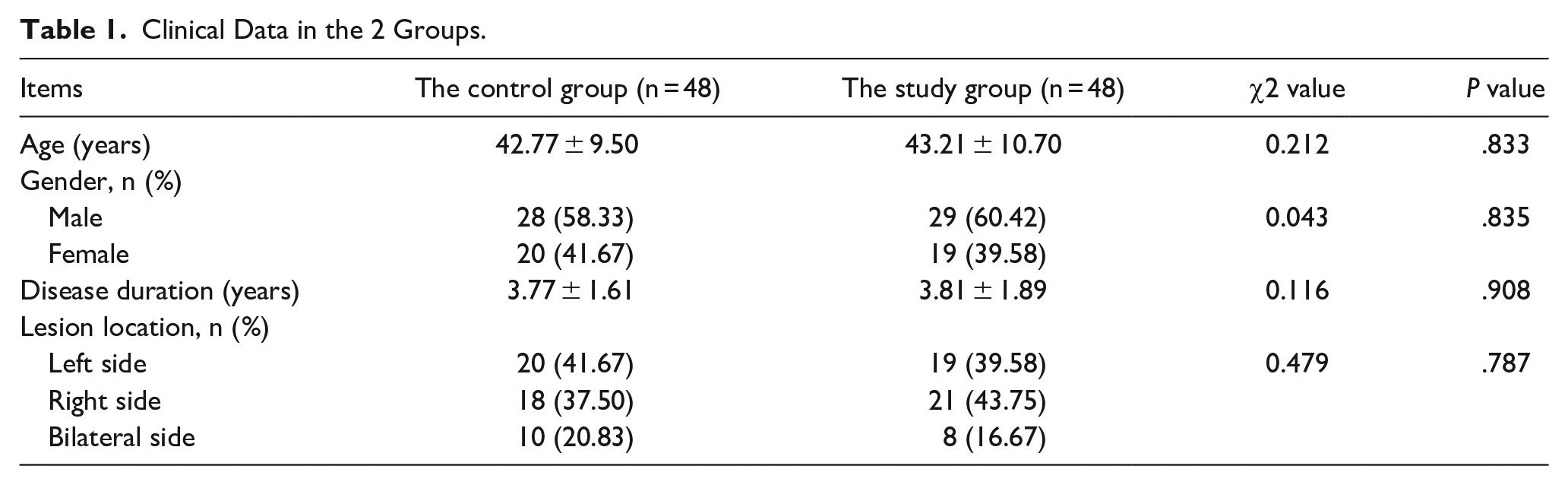
Differences in age, gender, disease duration, and lesion location in the 2 groups were considered to be insignificant at P > .05 (Table 1).
Clinical Data in the 2 Groups.
Clinical Efficacy
The total effective rate of the study group (95.83%) was significantly higher than that of the control group (83.33%) (P < .05). Thus, the impact of CAM combined with FP in patients with CRS after FESS was good (Table 2).
Clinical Efficacy Between the 2 Groups.

Symptom Scores
After therapy, the symptom scores of nasal congestions, runny nose, sneezing and dizziness, and headache of the study group were lower compared to those of the control group (P < .05). CAM combined with FP effectively alleviated symptoms and enhanced the postoperative experience of patients after FESS for CRS (Table 3).
Symptom Scores in the 2 Groups.
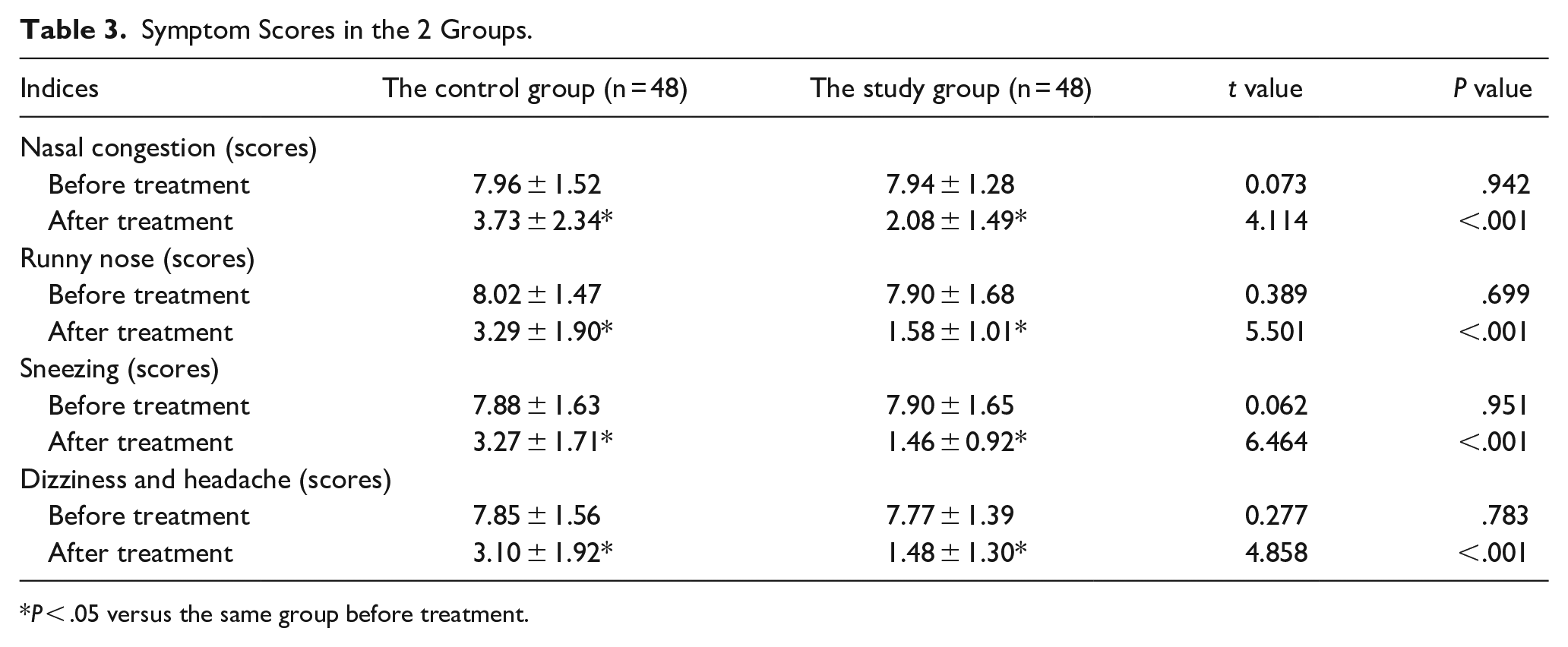
P < .05 versus the same group before treatment.
Nasal Function
Before treatment, the differences in symptom scores between the 2 groups were not statistically significant (P > .05). After treatment, NAR, DCAN, and T&T olfactory scores of the study group were lower, and NCV and NMCA were higher compared to those of the control group (P < .05). CAM combined with FP could improve the nasal function of patients after FESS for CRS (Table 4).
Nasal Function Between the 2 Groups.
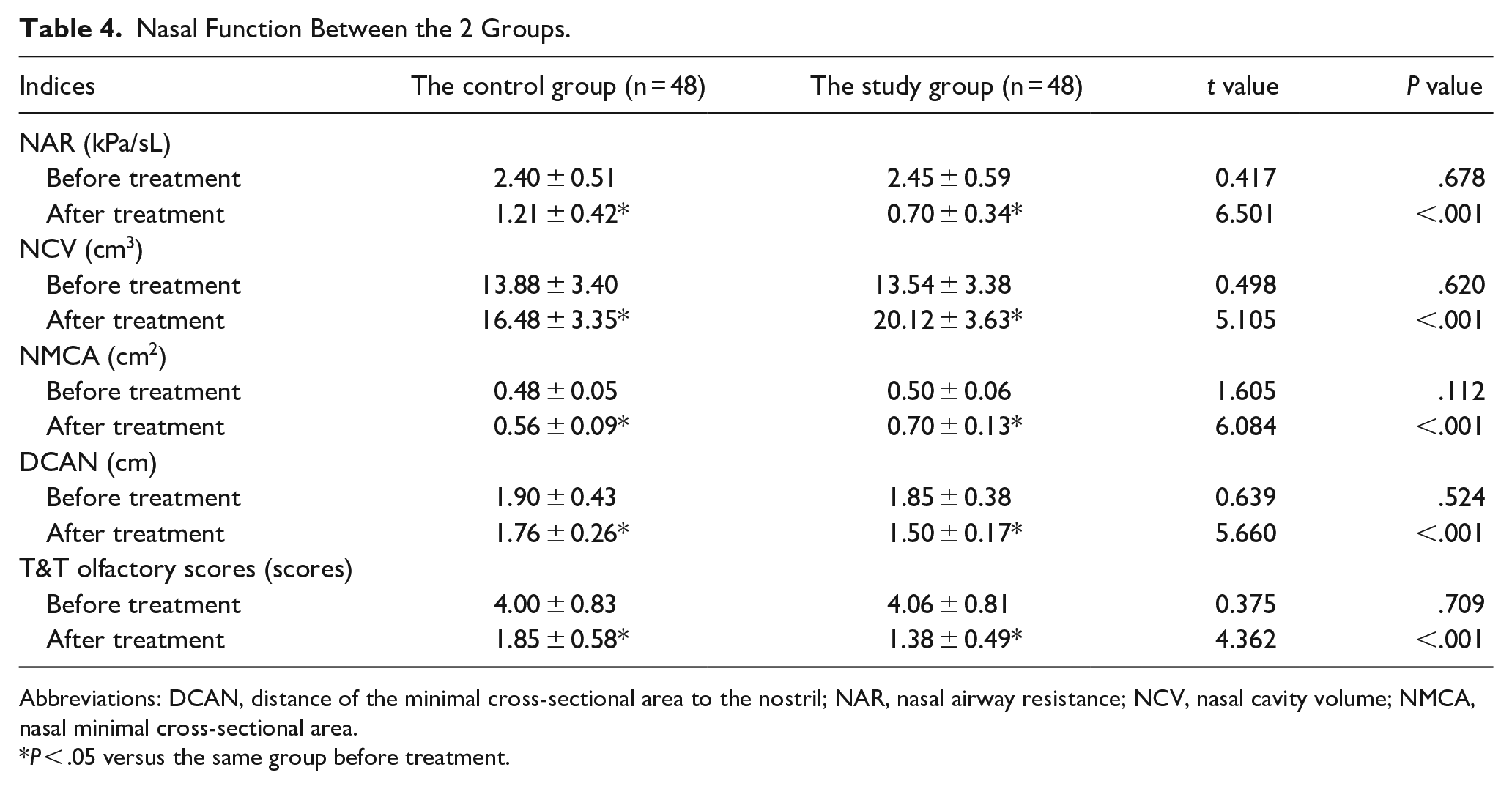
Abbreviations: DCAN, distance of the minimal cross-sectional area to the nostril; NAR, nasal airway resistance; NCV, nasal cavity volume; NMCA, nasal minimal cross-sectional area.
P < .05 versus the same group before treatment.
Nasal MCT Function
Before treatment, the differences of MCC and MTR in the 2 groups were not statistically significant (P > .05). After treatment, the MCC and MTR of the study group were higher compared to those of the control group (P < .05). CAM combined with FP could enhance the nasal MCT function in patients after FESS for CRS (Table 5).
Nasal Mucociliary Transport Function Between the 2 Groups.
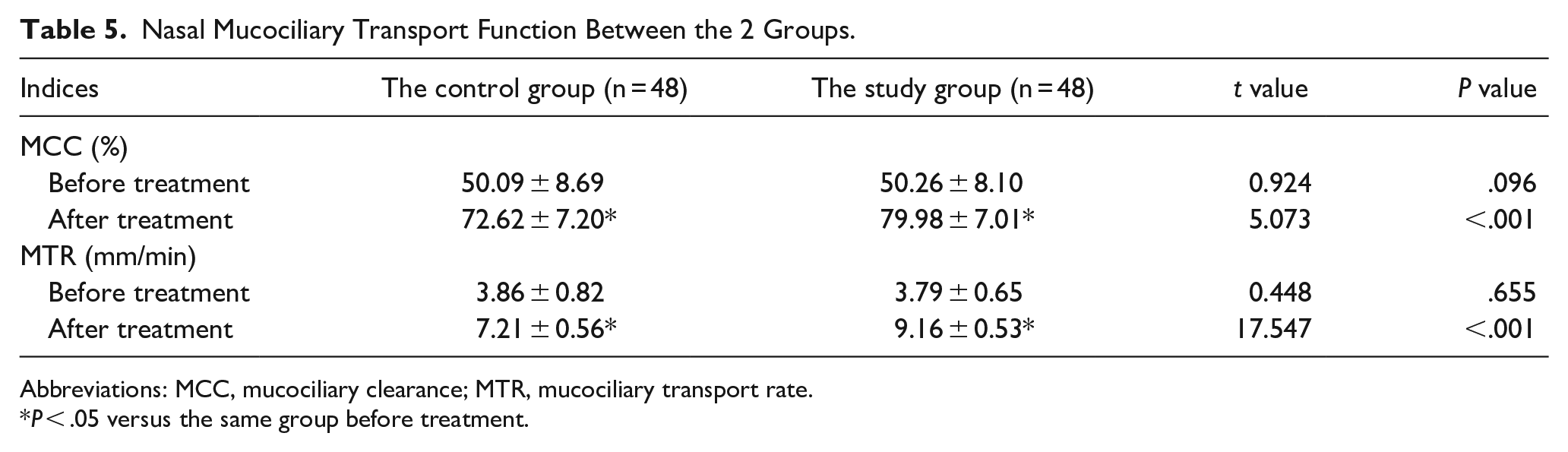
Abbreviations: MCC, mucociliary clearance; MTR, mucociliary transport rate.
P < .05 versus the same group before treatment.
Serum Inflammatory Marker Levels
Before treatment, there was no insignificant difference in serum inflammatory marker levels between the 2 groups (P > .05). After treatment, serum IL-6, IL-8, TNF-α, and PCT levels of the study group were lower compared to those of the control group (P < .05). CAM combined with FP was effective in reducing the inflammatory response in patients after FESS for CRS (Table 6).
Serum Inflammatory Factor Levels in the 2 Groups.
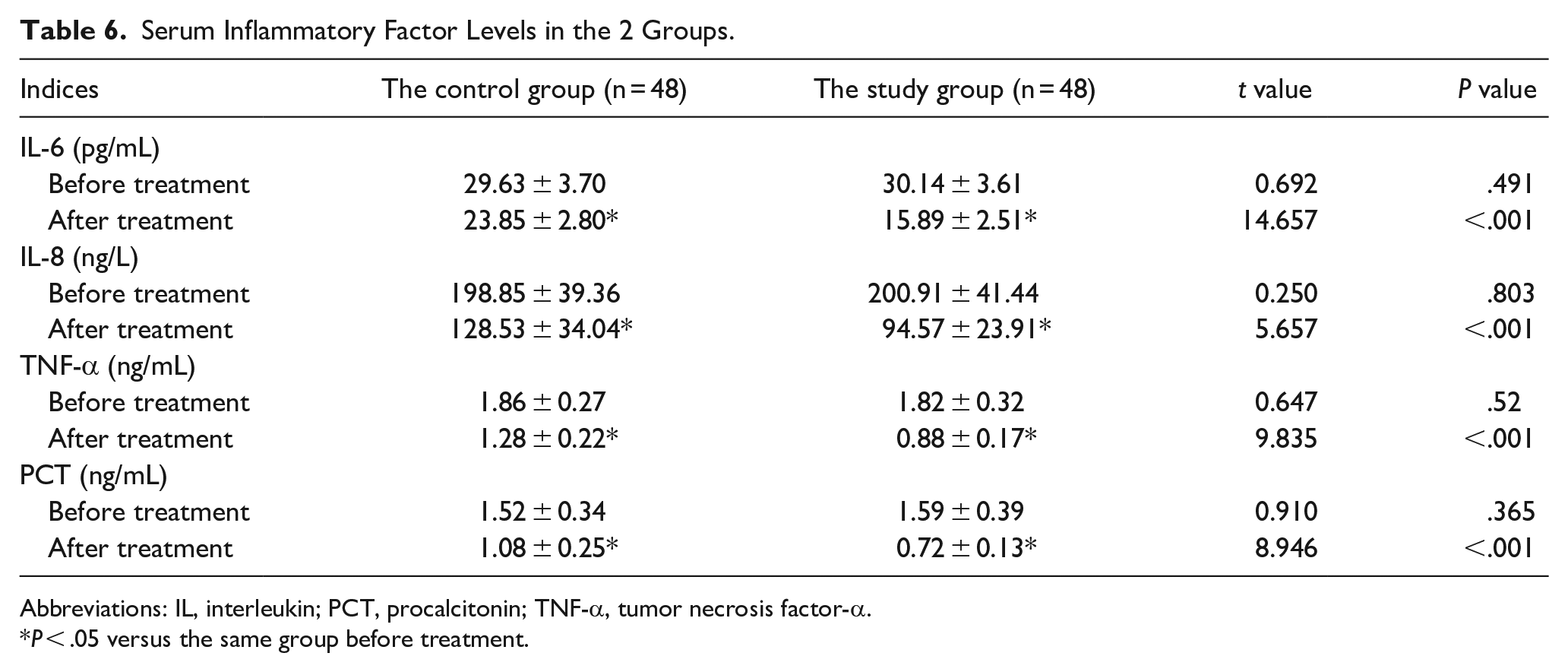
Abbreviations: IL, interleukin; PCT, procalcitonin; TNF-α, tumor necrosis factor-α.
P < .05 versus the same group before treatment.
Occurrence of Adverse Reactions
Differences in the total incidence of adverse reactions between the 2 groups were not considered significant (P > .05). The adoption of CAM combined with FP contributed to no increase in the occurrence of adverse reactions in patients after FESS for CRS (Table 7).
Occurrence of Adverse Reactions in the 2 Groups.
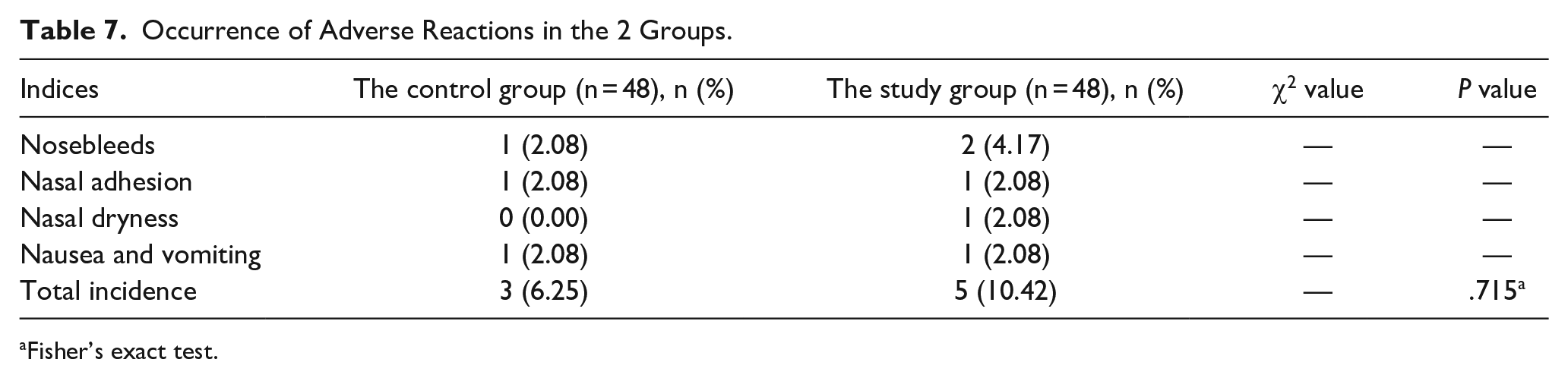
Fisher’s exact test.
Discussion
CRS is a complex inflammatory disease of the upper airways with a wide variety of clinical manifestations. 12 FESS is a minimally invasive surgical procedure commonly employed as an available intervention for the treatment of CRS. 13 Nevertheless, the postoperative situation is prone to complications, 6 and olfactory changes may be unpredictable. 1 The study demonstrates that CAM combined with FP exhibits good efficacy, leading to relief of clinical symptoms, improvement in nasal function, enhancement of MCT function, and reduction of inflammatory reactions without increasing adverse reactions.
Previous research supports the efficacy and safety of long-term, low-dose oral CAM in patients with refractory CRS after surgery, showing it improves clinical symptoms, facilitates mucosal epithelialization, and is well-tolerated in these patients. 14
It has been demonstrated that fluticasone expiratory delivery systems can enhance the therapeutic outcome of CRS by elevating the amount administered to the target superior/posterior anatomical site. 15 The FP-containing exhaled breath delivery system provides broader intranasal delivery, particularly to the upper and posterior nasal regions, compared to conventional nasal sprays, and reduces off-target losses caused by drop-out and swallowing. 16 Moreover, the study finds that the use of CAM combined with FP in post-FESS patients with CRS produces favorable results. It further shows that symptom scores of nasal congestion, runny nose, sneezing dizziness, and headache are alleviated in patients after the combination treatment. This indicates that CAM combined with FP is beneficial in relieving symptoms and enhancing the postoperative experience of patients after FESS for CRS.
In the study evaluating the efficacy and safety of long-term, low-dose CAM treatment in patients with CRS and nasal polyps after ESS, the findings reveal that 1 month of low-dose CAM reduces the patients’ need to blow their noses, frequency of sneezing, diminished sense of smell, and mucous secretion. 17 The study indicates that CAM, as a postoperative treatment, displays excellent efficacy. Consequently, the study focuses on analyzing the impacts of CAM combined with FP on nasal function and nasal MCT function in postoperative patients. The results show that CAM combined with FP could effectually enhance the nasal function and MCT function in postoperative patients. Through the literature review, the study finds that CAM and FP have anti-inflammatory and immunomodulatory influences.9,18 FP, when used with other drugs, inhibits the production of IL-6 and IL-8 in inflammatory cells. 19 CAM, as part of combination antibiotic therapy, significantly reduced PCT levels and a similar dynamic change in IL-6 during treatment. 20 The study confirms the anti-inflammatory properties of CAM, as evidenced by reduced serum levels of IL-6, IL-8, TNF-α, and PCT in treated patients, suggesting that CAM combined with FP helps reduce the inflammatory response in patients after FESS for CRS. Finally, the study compares the occurrence of adverse reactions with and without the use of CAM combined with FP after FESS. The results show that the treatment does not increase the incidence of adverse reactions in patients with CRS after FESS.
Salicaceae pollen is regarded as a moderate source of pollen sensitization. However, in large and compacted areas covered by Salicaceae, besides some particular situations such as air pollution, weather conditions, and urban ornamental vegetation, poplar, and willow pollen might be of local significance in producing seasonal allergic rhinitis. Thus, when various unfavorable markers converge, a minor issue like Salicaceae sensitization can escalate into a public health concern, such as seasonal allergic rhinitis. 21 Thus, the study inevitably has certain limitations. One is the undefined allergic status of patients. For example, some patients test negative for common allergens but may still have hidden allergens. In addition, the study is based on limited clinical data, and therefore the results are only representative of a small group of CRS patients. Future studies with larger sample sizes are needed to further validate the findings.
Conclusion
CAM combined with FP demonstrates excellent efficacy in improving nasal function, enhancing MCT, and reducing inflammation in CRS patients after FESS, with a low incidence of adverse reactions. The study supports the use of CAM and FP in the postoperative pharmacologic management of CRS. As our understanding of the pathophysiology of CRS continues to advance, treatment approaches and management strategies are evolving. However, given the limited data in the study, the therapeutic potential of CAM combined with FP warrants further investigation.
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.