
Abstract
Introduction
According to the World Health Organization, palliative care is a multidisciplinary approach to improving the quality of life of patients by addressing physical, psychological, and emotional issues. 1 A tracheostomy is performed to expedite weaning from artificial ventilation and provide a secure airway. Tracheostomy enables patients to be discharged from the intensive care unit (ICU) sooner, allowing for the improved utilization of limited ICU resources, and it may be associated with a decreased mortality rate. The utilization of tracheostomy in the context of palliative care presents a feasible alternative for the management of airway control. By engaging in a comprehensive conversation with the patient, their family, and a diverse team of healthcare professionals, this intervention can serve as a valuable element within the broader framework of a patient’s palliative care strategy. Teaching the care and follow-up of patients with tracheostomy in the critical care unit at palliative care clinics (PCCs) may reduce the burden of care for both the patient and their family members prior to home care.2,3
There are various advantages of substituting a tracheotomy tube for an endotracheal tube. These tubes include easier weaning from mechanical ventilation, a lower probability of further direct laryngeal injury, a higher likelihood of speech and oral intake, enhanced comfort, and a reduced intensity of nursing care that is required. However, infection at the surgical site, excessive bleeding, unintentional decannulation, mucus plugging, and pneumothorax are all potential problems that can arise after a tracheostomy. It is possible for tracheal stenosis, tracheomalacia, or a tracheoesophageal fistula to develop after a successful decannulation.4,5 Considering all these complications, tracheostomy decannulation should be considered as soon as possible. 6 Several characteristics, including strength, coordination, and awareness of pharyngo-laryngeal sensation, are essential to the success of the decannulation process. Clinical stability, neurological variables, secretory management, successful swallowing, cough strength, and airway patency have been identified to be crucial in systematic reviews. 7
Patients with a tracheostomy are increasingly sent to palliative care centers, particularly following the COVID-19 pandemic. However, there are very few studies on decannulation in palliative care units. 4 Our study aimed to determine the decannulation rate and factors that influence decannulation success in the palliative care unit.
Methods
The information of patients with tracheostomy hospitalized in the PCC of a research and training hospital between 2017 and 2022 was analyzed retrospectively after ethical approval was obtained from the Ethics Committee (date/number April 28, 2021/1). Patients who were younger than 18 years old and patients with day hospitalization were excluded from the study. The demographic data of the patients, their diagnoses, comorbidities, nutritional status, number of days of hospitalization, pressure ulcer status, pressure ulcer risk scores, and discharge status were recorded. It was checked whether there was a difference between these values between patients who had cannula removed and those who did not. Families and caregivers were trained in tracheostomy care, cuff exercise, and respiratory and swallowing therapy.
The Norton and Braden scales were used to assess the risk of bedsores in the patients. The Norton score uses 5 factors, for each of which the patient is assessed on a rating scheme varying from 1 (low risk) to 4 (high risk): physical condition, mental condition, activity, mobility, and incontinence. On each of the 5 risk variables, the patient receives a score between 1 and 4. The patient is considered at risk for pressure sores or decubitus ulcers if they have a score of 11. The Braden Scale is derived from 6 prevalent risk factors, including sensory function, moisture, activity, mobility, nutrition, and shearing force and friction. The total score represents an indication of the degree of risk, with lower scores suggesting a higher level of risk. Patients with a score of 18 or lower are in the risk group.8,9
All patients were evaluated and treated by a multidisciplinary team of doctors, nurses, physiotherapists, and dietitians. The airway patency of each patient was checked by an otolaryngologist by entering through the nasal and tracheal ostium. Additionally, cannula replacement was performed by the otolaryngologist in patients with granulation tissue around the cannula. An un-cuffed cannula was used in the patients with good swallowing functions, while a cuffed cannula was used in the patients with swallowing problems. The clinical nurse instructed all tracheostomy patients and their family members about tracheostomy care. By teaching cuff exercises to the families of the patient, the patient’s tracheal blood flow was ensured, and the patients who were able to speak had the ability to communicate with their relatives.10,11
Prior to tracheostomy decannulation, the patients were enrolled in a physical therapy program. First, deep breathing exercises were performed while the cuff was inflated. Then, the incentive spirometer was attached to the cannula. After deflating the tracheostomy cuff and obstructing the cannula with a sponge, upper respiratory tract breathing exercises were performed. With the mouthpiece, incentive spirometer exercises began. The patient completed these exercises while sitting up in bed or on a chair during the hours they were awake. For the patients with sputum, bronchial hygiene and forced expiration treatments were employed. The patients received effective coughing training, allowing them to expel secretion orally. All patients participated in a mobilization program that progressively increased in intensity. The swallowing functions of the patients were examined by an otolaryngologist and a physical therapist. A physiotherapist who specialized in swallowing rehabilitation had patients with inadequate swallowing functions perform swallowing exercises.12,13
In patients with normal physical examination results, lung radiology findings, biochemistry results, and hemogram results, tracheostomy closure was attempted before decannulation. The patients who required oxygen were given oxygen via a nasal cannula or an oxygen mask. The patients were monitored for indications of discomfort and increased breathing effort. The patient’s oxygen saturation, ability to swallow sputum status, coughing status, and respiratory rate were constantly monitored while the ostium was closed. After tracheostomy closure, blood gas analyses were performed. Additionally, the expected PaO2 values according to age were determined with the formula PaO2 = 104.2 − (0.27 × age) or 100 − (age/3). 14 It was considered safe to remove the tracheotomy tube if the blood gas measurements were normal, and the patient was comfortable and able to manage secretions through the oropharynx for 12 to 24 hours. Because the ostium closes swiftly after cannula removal, it may not be possible to re-cannulate a patient who has desaturated. Patients with exacerbated comorbidities, such as advanced heart failure, advanced cancer, and advanced Alzheimer’s disease, did not undergo decannulation due to the possibility of desaturation.
Statistical Analysis
The descriptive statistics that were used in the statistical analyses included mean ± standard deviation values for the continuous data and frequency and percentage values for the categorical data. The normality of the distribution of the continuous data was checked by the Kolmogorov-Smirnov test. Groups of variables that did not show normal distribution were compared by the Mann-Whitney U test. The distributions of the categorical variables in groups were evaluated using the Pearson chi-squared test. The analyses were carried out using the IBM SPSS 21 (IBM SPSS, Inc., Chicago, IL, USA) package program. The threshold for statistically significant differences was determined to be .05.
Results
Between 2017 and 2019, 41 of 102 tracheostomy patients were decannulated. It was found that there was a statistically significant difference between the mean ages of the decannulated and non-cannulated groups, and the mean age of the decannulated group (52.10 ± 20.54, median: 53) was significantly lower than the mean age of the non-decannulated group (61.48 ± 18.07) (z = −2.516, P = .012). Twelve of the 41 patients in the decannulated group (29.3%) and 19 of the 61 in the non-decannulated group (31.1%) were female (Table 1). In both the decannulated and non-decannulated groups, almost all patients had malnutrition and restricted movement. In both groups, again, the rates of patients requiring oxygen support at the time of admission were over 80%. The decannulation statuses of the patients were not significantly associated with any other parameters except for age (Table 1).
Demographic and Clinical Characteristics of Patients.
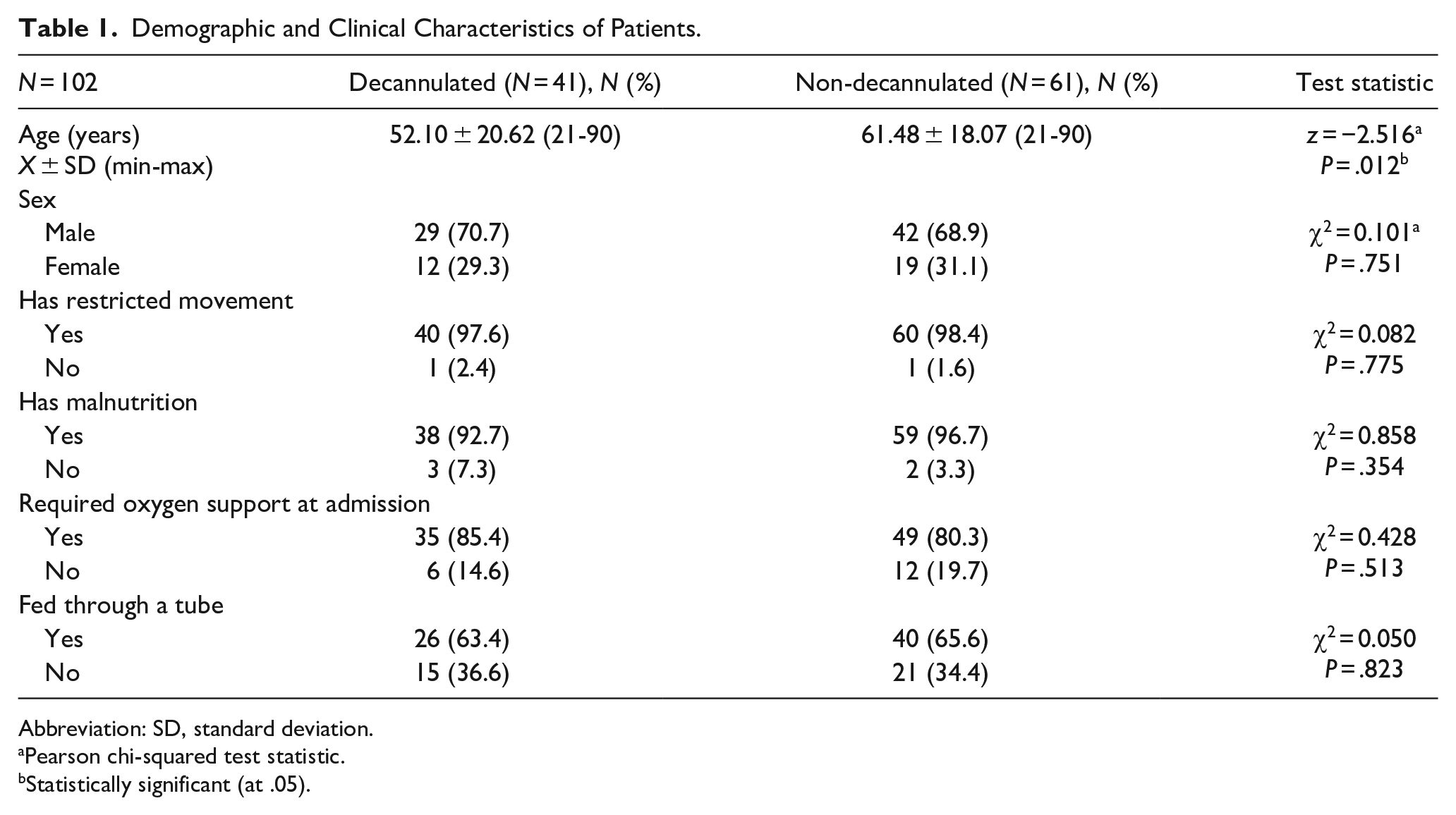
Abbreviation: SD, standard deviation.
Pearson chi-squared test statistic.
Statistically significant (at .05).
There were several different comorbidities in the patients. The mean number of comorbidities was 2.595 ± 1.6. There was no significant difference between the decannulated and non-decannulated groups regarding their number of comorbidities and comorbidities (Table 2).
Comorbidities of Patients.
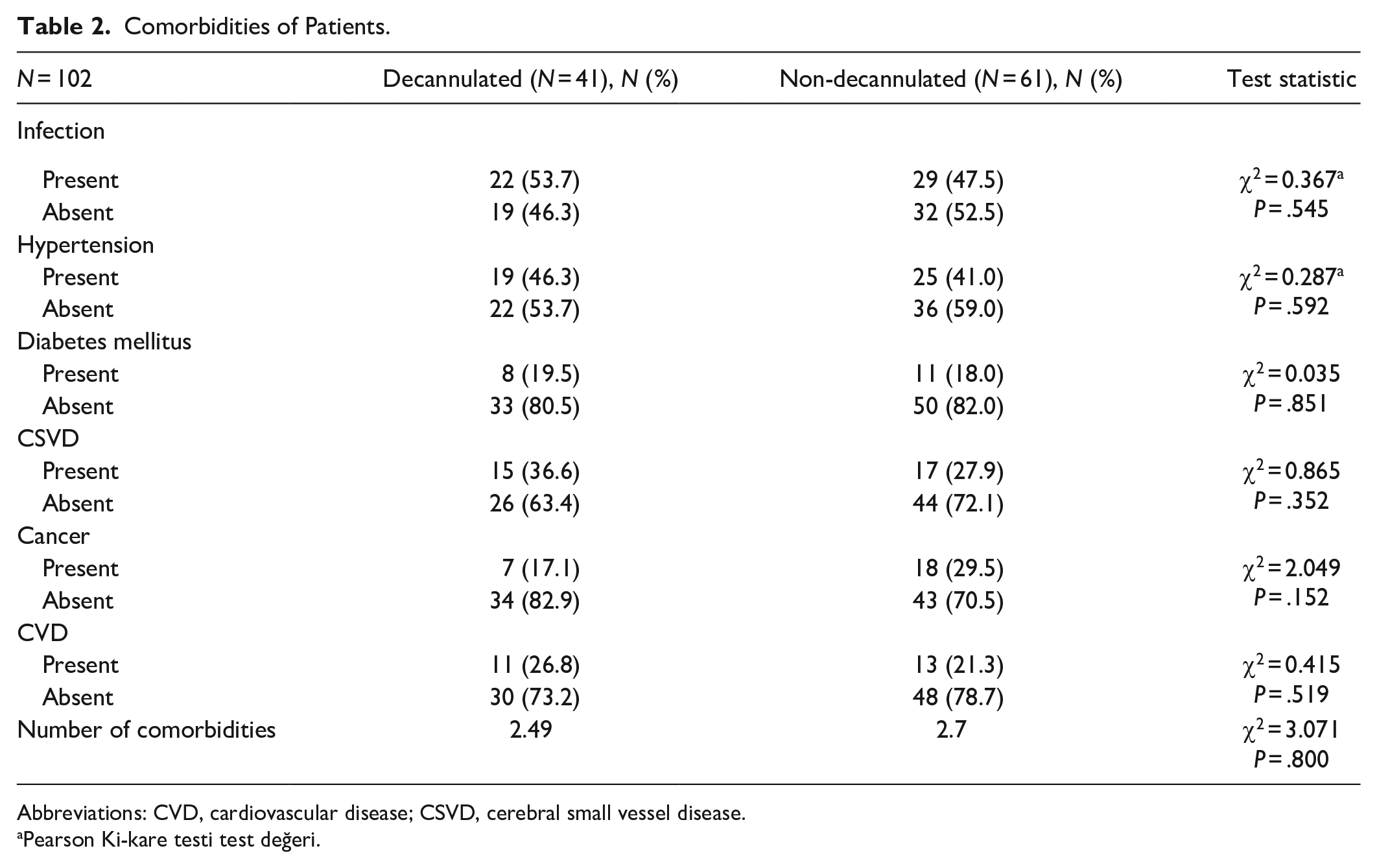
Abbreviations: CVD, cardiovascular disease; CSVD, cerebral small vessel disease.
Pearson Ki-kare testi test değeri.
Thirty-two decannulated patients (78%) and 39 non-decannulated patients (63.9%) had been referred from ICUs. While 26 of the patients had been referred from inpatient clinics, 5 had arrived from their homes. Thirty-one decannulated and 45 non-decannulated patients were discharged to their homes. The number of patients referred to ICUs was 2 in the decannulated group and 7 in the non-decannulated group. Six patients in the non-decannulated group died. Eleven patients were readmitted to the hospital for cannula replacement, 2 were readmitted for connection to a household-type mechanical ventilation device, and 6 were readmitted due to infections. Only 1 decanulated patient was hospitalized for infection (urinary system). None of the decanulated patients had any problems due to the withdrawal of the cannula (Table 3).
Referral Clinics and Discharge Statuses of Patients.
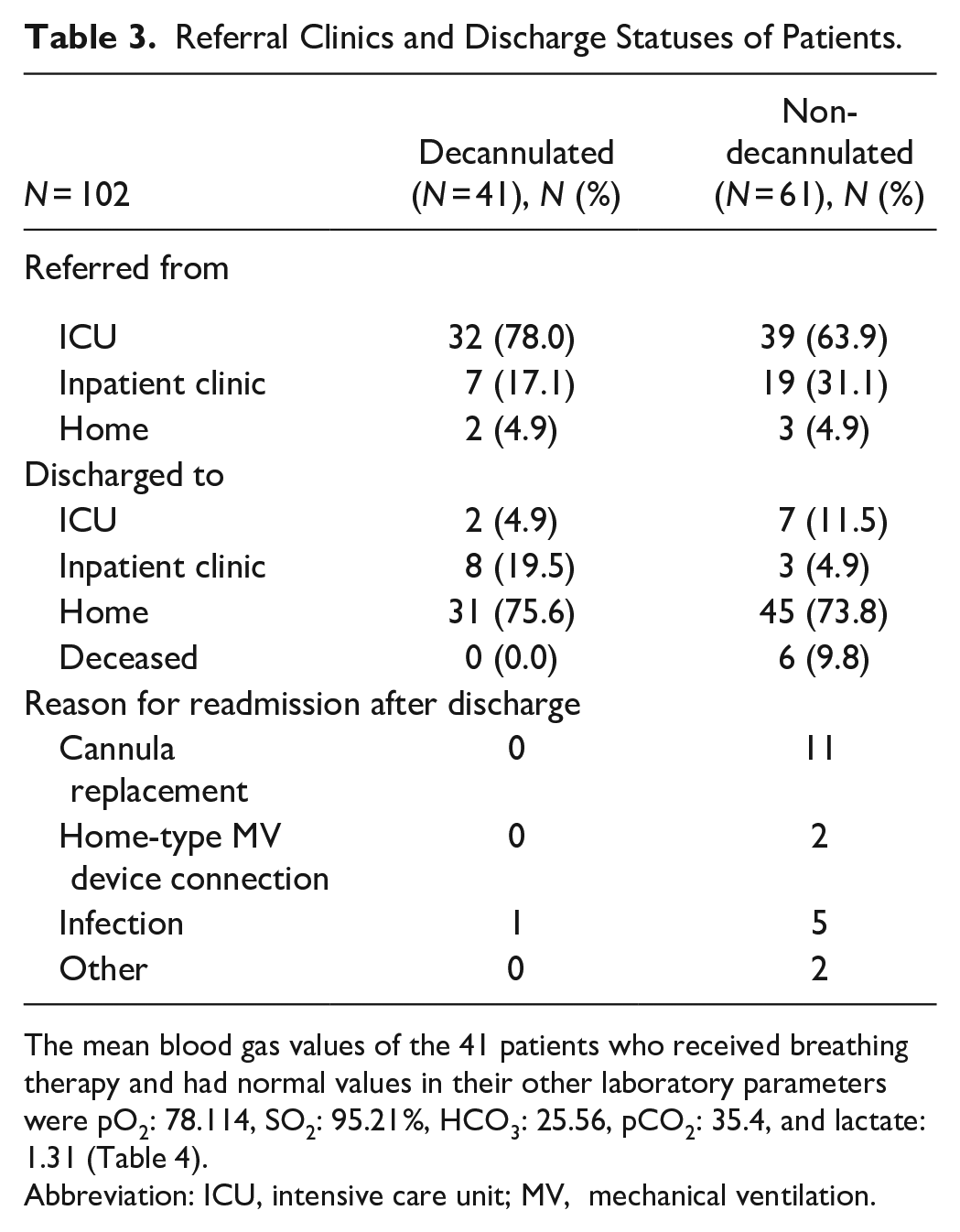
The mean blood gas values of the 41 patients who received breathing therapy and had normal values in their other laboratory parameters were pO2: 78.114, SO2: 95.21%, HCO3: 25.56, pCO2: 35.4, and lactate: 1.31 (Table 4).
Abbreviation: ICU, intensive care unit; MV, mechanical ventilation.
The mean blood gas values of the 41 patients who received breathing therapy and had normal values in their other laboratory parameters were pO2: 78.114, SO2: 95.21%, HCO3: 25.56, pCO2: 35.4, and lactate: 1.31 (Table 4).
Blood Gas Values of Decannulated Patients during Closure.
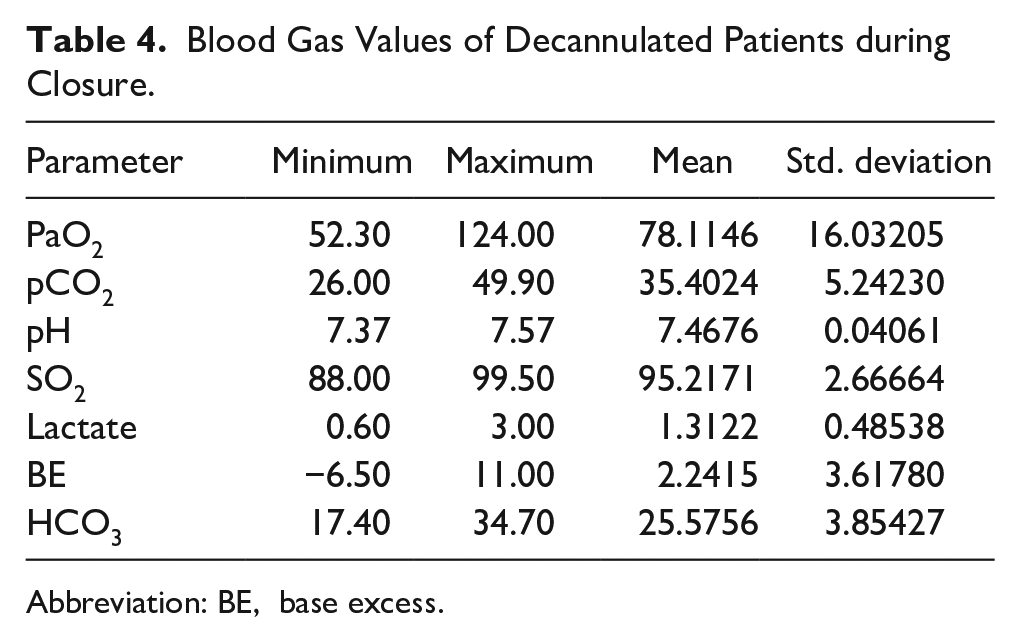
Abbreviation: BE, base excess.
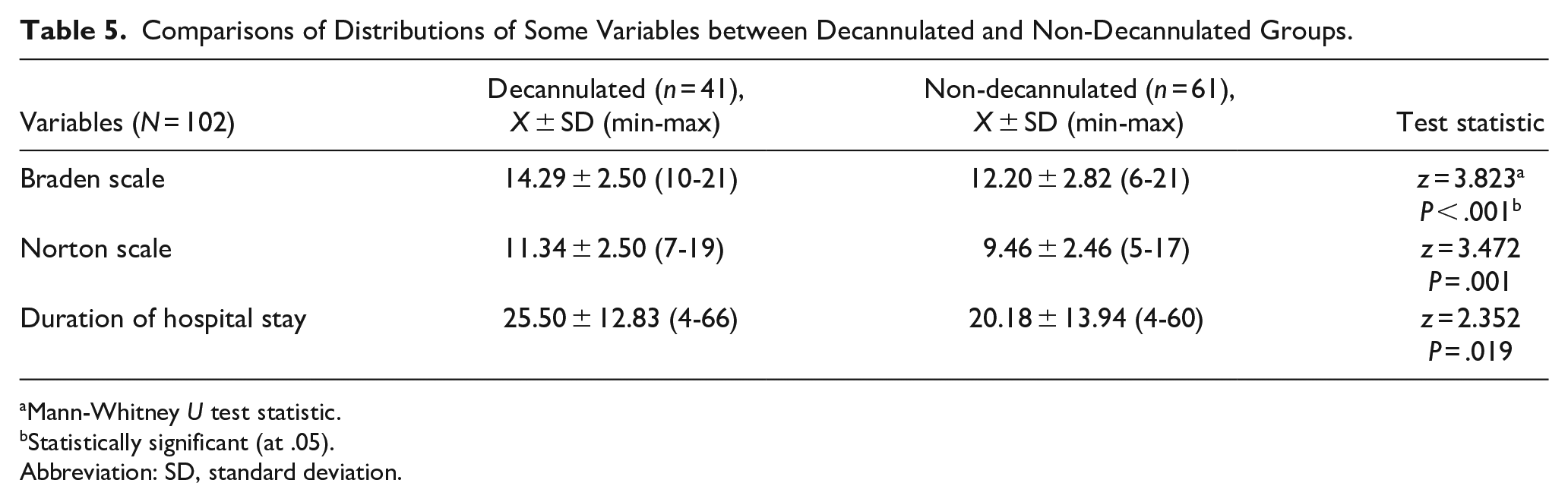
The mean Braden Scale score of the decannulated group (14.29 ± 2.50) was significantly higher than that of the non-decannulated group (12.20 ± 2.82) (z = 3.823, P < .001), and the mean Norton Scale score of the decannulated group (11.34 ± 2.50) was significantly higher than that of the non-decannulated group (9.46 ± 2.46) (z = 3.472, P = .001) (Table 5).
Comparisons of Distributions of Some Variables between Decannulated and Non-Decannulated Groups.
Mann-Whitney U test statistic.
Statistically significant (at .05).
Abbreviation: SD, standard deviation.
It was observed that the mean length of hospital stay of the decannulated group (25.50 ± 12.83) was significantly higher than the mean length of stay of the non-decannulated group (20.18 ± 13.94) (z = 2.352, P = .019) (Table 5).
The mean length of stay of the patients in the PCC was 22.19 ± 13.67 days (median: 21, min: 4, max: 66).
Discussion
Most of the patients with tracheostomy who were admitted to the PCC (68.9%) had been referred from ICUs. The increased demand for intensive care following the onset of the COVID-19 pandemic led to an acceleration in admissions to the PCC. While the care requirements of such patients are intensive, the rate of discharge to home in this study was also high (74.8%, n = 77). In addition to breathing therapies, the education of family members about tracheostomy care may also be thought to contribute to the discharge of patients to their homes.10,11 Tracheostomy care, deep tracheal aspiration, humidification, coughing exercises, speech valve usage, breathing exercises, and ambulation are subjects that are taught to the caregivers of patients by palliative care doctors, educator nurses, and physiotherapists.12,13 In addition to the 41 decannulated patients, 36 patients who were not decannulated could also be discharged to their homes by teaching the aforementioned subjects to their families. It was reported that improving the knowledge and skills of caregivers regarding tracheostomy care increases their belief in their ability to provide care to these patients. 10
A similar study, which argued that the care of such patients will be more effective when provided with a multidisciplinary approach, emphasized the importance of the roles of respiratory therapists, physiotherapists, swallowing and speech therapists, nurses, and psychologists.15-17 In the context of our study, it may be stated that the PCC, which is a multidisciplinary care environment, has an important place in the care of such patients.
In the PCC, by teaching coughing exercises to the relatives of tracheostomy patients, the tracheal blood flow of the patient is ensured, and patients who are able to speak gain the ability to communicate with their relatives. Patients who are monitored in a conscious state in ICUs for months have increased levels of morale and motivation when they can communicate and speak with their relatives. Providing this opportunity to patients who have not lost their ability to speak affects the quality of life of these patients positively. 18
The presence of a tracheostomy tube disrupts normal tracheal elevation during swallowing.16,19 In this study, when the ostium of the patient was closed, their ability to swallow their sputum, cough, breathe in and out, and their respiratory rate were closely monitored. The arterial blood gases of the patients who did not experience a decrease in their saturation were analyzed. The patients were decannulated based on these blood gas values. The mean pO2 value of the patients was 76.19 (Table 5). Assuming that the pO2 values of the patients could have been reduced by the difficulty of swallowing their secretions in room air and when the cannula was blocked, as well as the presence of the cannula in the respiratory tract, the researchers did not wait for pO2 values to reach the ideal level of 83. 14 None of the decannulated patients were desaturated in their follow-ups. In a similar study, closure was considered successful when there was no oxygen desaturation, and oxygen requirements did not reach or exceed 40% FiO2. 20 Because the ostium will rapidly close after the removal of a cannula, the re-cannulation of a desaturated patient may not be possible. Decannulation procedures were not studied in patients with comorbidities such as old age, heart failure, advanced-stage cancer, or advanced-stage Alzheimer’s assuming that these conditions could raise the risk of desaturation.20-22
In our study, the distributions of the Braden and Norton Scale scores of the patients differed significantly between the decannulated and non-decannulated groups. With the recommendation of the Braden and Norton Scale Ministry of Health, every inpatient is cared for. The mean Braden Scale score of the decannulated group (14.29 ± 2.50) was significantly greater than that of the non-decannulated group (12.20 ± 2.82) (z = 3.823, P < .001) Similarly, the mean Norton Scale score of the decannulated group (11.34 ± 2.50) was significantly greater than that of the non-decannulated group (9.46 ± 2.46) (z = 3.472, P = .001). In both scales, consciousness levels are important. In similar studies carried out by Heidler et al and Alhashemi et al, decannulation was more successful in patients who were conscious.19,21 Physical activity and the ability to move are covered in both scales. The positive effects of physical activity and peripheral muscle strength on respiratory functions were reported.23,24 This shows us that to be able to decannulate them, patients should be mobilized as soon as possible, and physical capacity should be increased.
The mean duration of hospitalization among the patients who were included in this study was 22.19 ± 13.67 days. The patient with the shortest stay at the hospital had a hospitalization duration of 4 days, while the patient with the longest stay had a hospitalization duration of 66 days. The potential reasons for prolonged hospitalization could be listed as a high number of comorbidities, feeding through a tube, mobilization problems, the presence of pressure sores, and the resistance of caregivers. 21 The hospitalization durations of the groups in this study differed significantly, where the mean hospitalization duration of the decannulated group (25.50 ± 12.83 days) was significantly longer than that of the non-decannulated group (20.18 ± 13.94) (z = 2.352, P = .019). The monitoring of the respiratory parameters of the patients after their decannulation procedures led to the prolongation of their hospitalization.
The patients in the decannulated group included 15 trauma patients (traffic accidents, firearm injuries), 11 had cerebrovascular events, 5 had oncological diagnoses, 6 had Chronic obstructive pulmonary disease or aspiration pneumonia, and 4 had cardiovascular diseases. There was no significant difference between the decannulated and non-decannulated groups in terms of hypertension, cardiovascular diseases, cerebrovascular diseases, or diabetes mellitus. In contrast, in the study where they developed the DEKAN scoring system to measure the success of decannulation in the ICU, Chul Park et al reported that the presence of cancer or neurological diseases affected decannulation procedures negatively. 20
In this study, the mean age of the decannulated group (51.71 ± 20.62) was significantly younger than the mean age of the non-decannulated group (61.48 ± 18.07) (z = −2.516, P = .012). Similar studies also found that older age affected decannulation procedures negatively.19-21 Structural abnormalities seen in old age include chest wall and thoracic spine deformities, which compromise the compliance of the overall respiratory system and result in an increase in breathing effort, which may explain the negative impact of advanced age on decannulation. 25
The patients whose swallowing functions were considered inadequate despite the removal of their cannulas were sent home with PEG Percutaneous endoscopic gastrostoma. Even though they have respiratory capacity, patients who are unable to swallow should be subjected to intensive examinations by swallowing assessments. 26 When the cannula is in place, the inflated cuff of the cannula is protective against aspiration. This is why patients for whom oral feeding will be allowed should be identified very carefully. Oral feeding was not allowed in patients with Alzheimer’s or severe neurological deficits with permanent brain injury, and these patients were sent home with feeding tubes. 26 The feeding tubes of the 11 decannulated patients who passed the swallowing test were also removed. This is a rehabilitation process that requires interdisciplinary management by a multidisciplinary team.27,28
Most of the patients we followed in our study were tracheostomized after prolonged mechanical ventilation in the ICU. Prolonged mechanical ventilation and immobility lead to impaired respiratory mechanics, decreased lung volumes, and respiratory muscle weakness. These complications can be avoided by enrolling these patients in a respiratory physiotherapy program and mobilizing them as soon as feasible. Therefore, physiotherapists play a crucial function in palliative care units. Navarro-Meléndez et al reported that palliative care including physiotherapy improved the functionality of PCU patients, their independence, and their skills for activities of daily living. 29
Previous studies have defined the indicators of successful decannulation as the age of the patient, their consciousness status, their time of spontaneous respiration before decannulation, their coughing capacity, secretions, and oxygenation parameters. 30 A limitation of our study was that the secretions of the patients were not measured quantitatively.
Conclusion
This study demonstrated that the monitoring and evaluation of individuals undergoing tracheostomy procedures can be carried out effectively in PCCs. The importance of a multidisciplinary team and care plan for the treatment of these patients was emphasized by the results of this study. In terms of Norton and Braden scales, it was observed that the rate of cannula removal was significantly higher in patients with low risk of pressure ulcers. It may be recommended to repeat both scales in more centers in the follow-up of patients with tracheostomy. It was also shown that aging, immobility, and impaired consciousness are parameters that negatively affect decannulation success.
Footnotes
Acknowledgements
We would like to thank the doctors, nurses, physiotherapists psychologists, social workers, and data processing personnel working in the Palliative Care department.
Data Availability Statement
All data produced or analyzed during this study are included in the published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Ethics Committee (date/number April 28, 2021/1). All methods were carried out in accordance with relevant guidelines and regulations of Gulhane Training and Research Hospital, University of Health Science and Turkey guidelines for ethical conduct of research. Informed consent was obtained from all subjects and/or their legal guardian to participate in the study.