
Abstract

Significance Statement
Fibrous dysplasia is a rare, expansile, benign bone lesion in the paranasal sinuses. It is recognized by its typical ground-glass appearance on computed tomography (CT) but may sometimes have a cystic appearance. This should be considered in the differential diagnosis of lesions in radiological evaluation. Surgery is recommended in symptomatic patients and follow-up is recommended in asymptomatic patients.
A 27-year-old woman presented to our clinic with swelling and pain on the left side of her forehead. Her complaints had increased over the past year. She had no history of surgery, trauma, or known chronic illness. Clinical examination revealed a hard, immobile lesion of approximately 1 cm in the left midline frontal region. A non-contrast CT scan of the paranasal sinuses was performed without significant laboratory findings. The images obtained showed a uniformly circumscribed hypodense mass lesion measuring 16 × 19 × 21 mm in the left part of the frontal sinus, causing bone expansion (Figure 1A and B). Hounsfield unit values varied between 20 and 154. Contrast-enhanced magnetic resonance (MR) imaging was performed with a presumptive diagnosis of a mucocele. On MR imaging, the lesion had hypo-intensity on T1- and heterogeneous intensity on T2-weighted images. There was no diffusion restriction and post-contrast series showed peripheral contrast enhancement (Figure 2A-C). With these imaging features, endoscopic frontal sinus surgery was planned with a diagnosis of mucocele. During surgery, no mucus was aspirated from the hard mass, and biopsies were taken. Histopathological examination revealed fibrous dysplasia with fibro-osseous proliferation. The patient, who refused surgical excision due to aesthetic concerns, was followed up. One year later, there was no significant change in the lesion bytes on the follow-up CT scan. However, internal hyperdense areas had developed (Figure 1C and D). On MR imaging, heterogeneous appearance persisted on T1- and T2-weighted images, and contrast enhancement was observed in the lesion on post-contrast series (Figure 2D). The patient is being followed up.
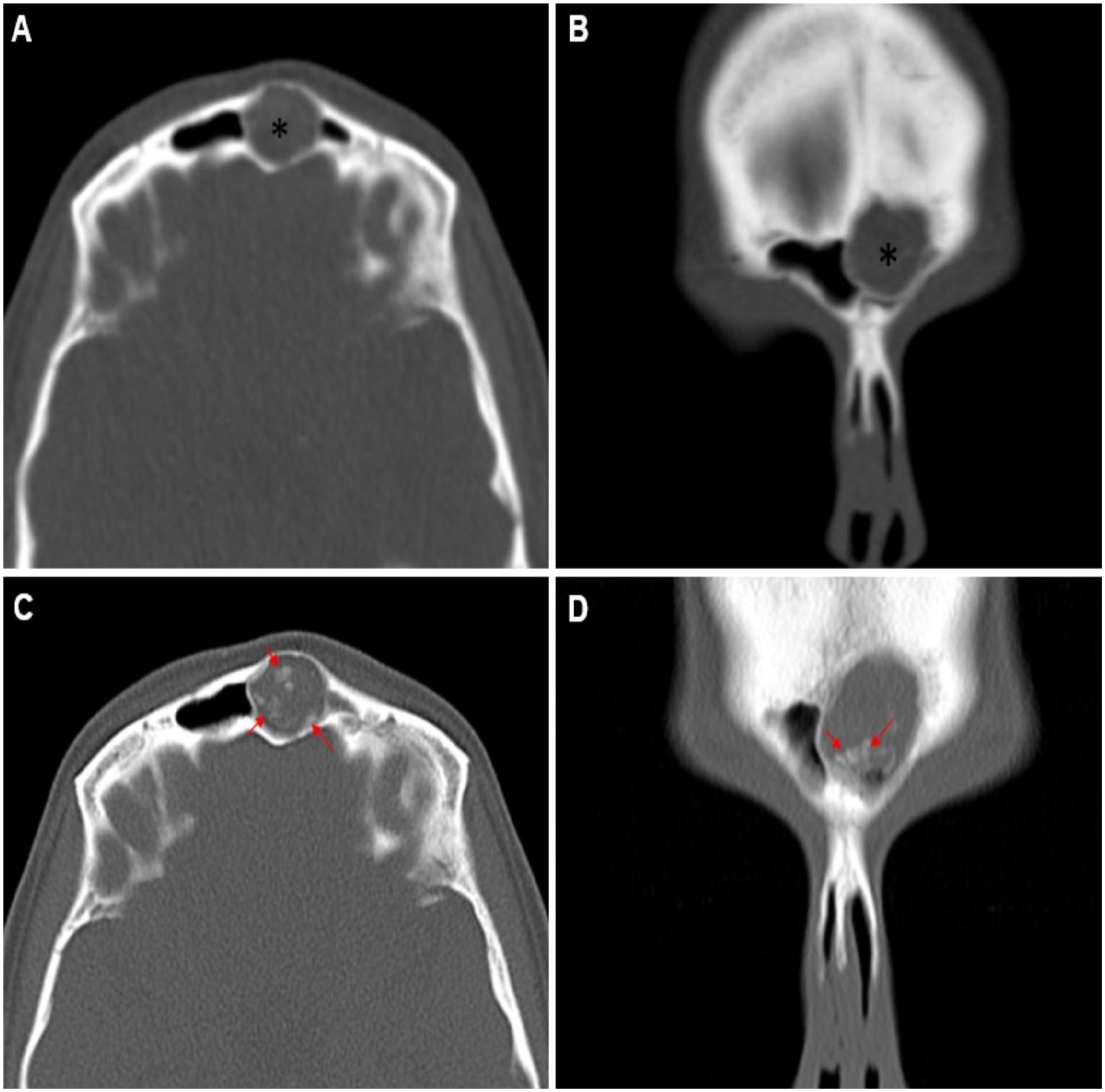
Non-contrast axial (A) and coronal (B) section paranasal sinus CT images demonstrate an expansile hypodense lesion with smooth margins (asterix). Axial (C) and coronal (D) non-contrast CT images acquired 1 year later illustrate the development of hyperdense regions within the lesion (arrows).
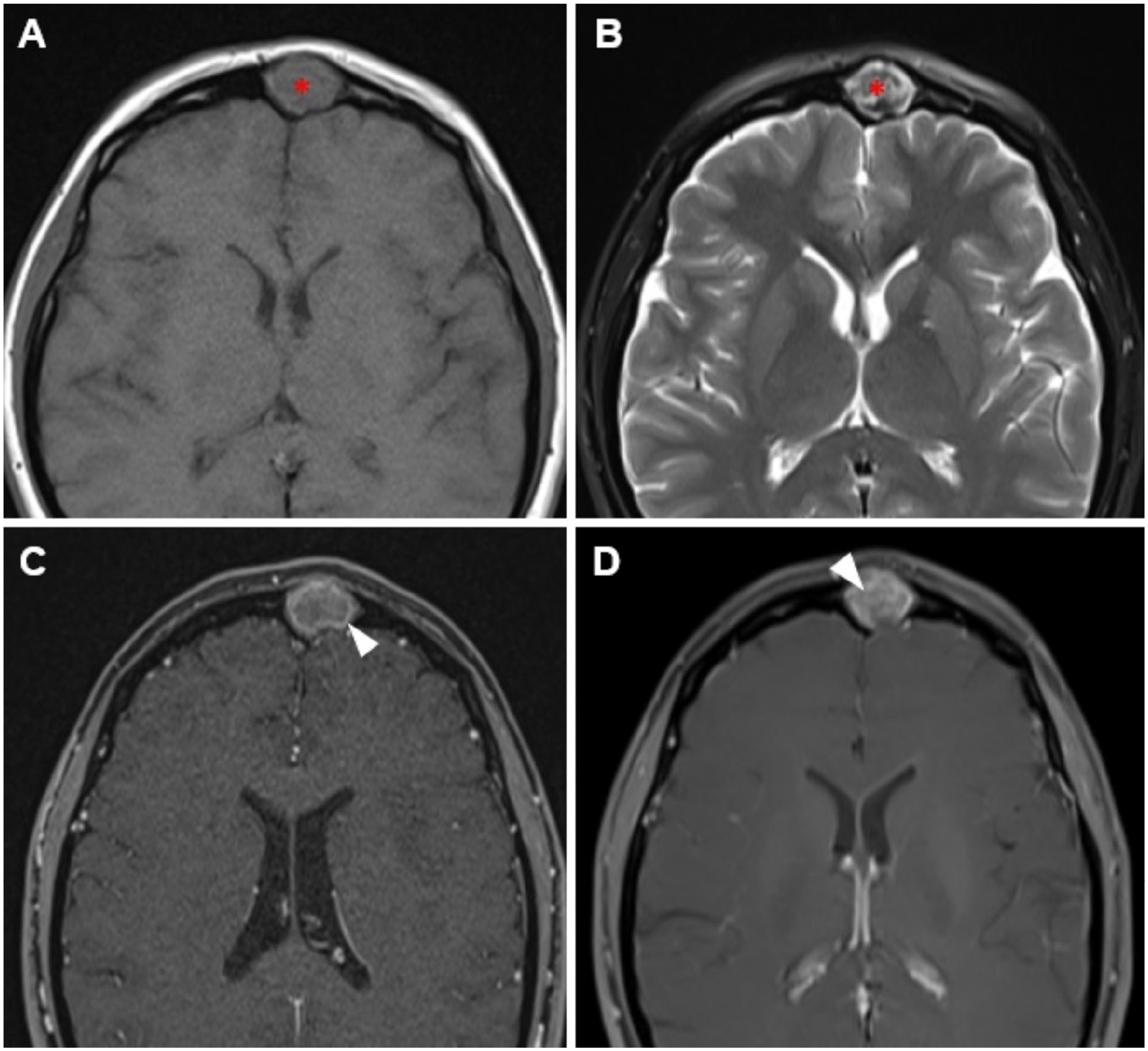
The frontal sinus lesion (asterix) is iso-hypointense on axial section T1-weighted image (A), heterogeneous intensity on T2-weighted image (B) and peripherally contrasted on post-contrast T1-weighted series (C) (arrowhead). One year later, post-contrast T1-weighted axial section image (D) shows internal contrast enhancement in the lesion (arrowhead).
Fibrous dysplasia is a common, congenital, but non-hereditary, benign bone lesion. Normal bone structure is replaced by fibrous stroma and immature bone islands as a result of impaired osteoblastic activity of skeletal stem cells. This condition can manifest in any bone in the body, with approximately one-third of cases involving the craniofacial region. While the maxilla and the mandible are the most commonly affected bones, isolated paranasal sinus fibrous dysplasia is a rare occurrence.1,2 Craniofacial fibrous dysplasia may be asymptomatic and the most common symptoms are swelling and facial asymmetry.1-3 CT is the gold standard in radiological imaging, and a ground-glass appearance is a typical finding. In a smaller number of cases, a homogeneous hyperdense and cystic appearance is observed. It is hypothesized that the lesions, which are more radiolucent in the early stages of the disease, become radiopaque as the disease progresses. MR imaging is primarily employed to ascertain the relationship between the lesion and the surrounding neurological structures. The lesion displays an iso-hypointense appearance in T1-weighted images, exhibiting variable intensity in T2-weighted images, and displays modest contrast enhancement in post-contrast series.2-4 Mucoceles are expansile lesions such as fibrous dysplasia with variable attenuation on CT imaging. Contrast enhancement on MR imaging is peripheral and not inside the lesion. 5 As fibrous dysplasia is thought not to progress after puberty, clinical observation and follow-up is recommended in asymptomatic cases. Surgical treatment is performed in cases of visual changes, nerve compression, and facial asymmetry.1-3
Footnotes
Author Contributions
EG: idea, design, literature review, writing the article, references, and fundings. AS: design, control/supervision, critical review, materials.
Consent
We declare that written informed consent for patient information and images to be published was provided by the patient.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases.