
Abstract
Schwannomas are generally known to be benign tumors that arise from Schwann cells. The most frequently encountered tumors of this type in ENT are vestibular schwannomas or acoustic neuromas. However, head and neck localization, although rare, has been documented in the literature. We present the case of a 13-year-old girl who presented with chronic swelling of the left cheek, leading to aesthetic discomfort. Clinical examination objectified a palpable swelling on both the external and internal sides of the left cheek. No other abnormalities were detected during the clinical examination. Ultrasound of the soft tissues identified the left cheek swelling as corresponding to a subcutaneous cyst. No further investigations were indicated for this patient. The treatment consisted of surgical excision via an intraoral approach with an internal buccal incision. Histological analysis confirmed the diagnosis of schwannoma. Schwannoma, a benign neurologic tumor, is rarely located in the face, particularly in the jaw. Its diagnosis is confirmed through histopathological examination, and treatment typically involves complete surgical removal when feasible.
Introduction
Schwannoma is a common tumor generally affecting all age groups with peak incidence occurring between 40 and 60 years of age. It affects both sexes equally, with no gender predominance. 1 Schwannomas are solitary, benign, well-demarcated, painless, and slow-growing tumors of ectodermal origin, arising from Schwann cells located in the perineuronal sheath covering the axons. 2 The prognosis is generally favorable; however, schwannomas have exceptional potential for malignant transformation and typically do not recur locally after complete excision, provided the tumor’s location permits it. 1 The most frequent site of schwannoma in the head and neck region is the cervical area, with reported rates varying between 8% and 16%. 3 Other sites, in decreasing order of frequency, include the parotid glands, buccal region, scalp, tongue, and throat. Masseteric intramuscular schwannomas are exceedingly rare. 4 Schwannoma should be considered in the differential diagnosis when a tumor is present in the parotid-masseter region.
Case Report
A 13-year-old Caucasian teenager with a history of allergic asthma presented to the otorhinolaryngology clinic with a swelling of the left cheek. The onset of the symptoms dated back 4 years, marked by the appearance of a cheek painless swelling that had progressively increased in size, causing the patient aesthetic concern. The patient reported no associated functional symptoms or other complaints. There was no history of weight loss, general malaise, salivary colic, masticatory disorders, otalgia, fever, asymmetry, or facial pain. The primary reason for consultation was aesthetic discomfort.
Physical examination revealed a left cheek swelling measuring 2.5 cm along its long axis, oval in shape, soft in consistency, mobile in relation to both the deep and superficial planes, with no adjacent inflammatory signs. The swelling was also visible and palpable on the inner side of the cheek, with the same characteristics as on the outer side. The remainder of the general examination, particularly the neurological assessment, was unremarkable. Notably, the patient exhibited no facial or trigeminal nerve abnormalities, such as hypoesthesia or facial hemiparesis.
A cervical ultrasound revealed a left cheek swelling corresponding to a well-defined subcutaneous cyst, echogenic in content, with a thick appearance, measuring 22 mm along its long axis.
Management consisted of intraoral excision. Surgical exploration revealed a bilobed, soft, yellowish-white, translucent mass measuring 2 cm along its long axis, independent of adjacent tissues (Figures 1 and 2).
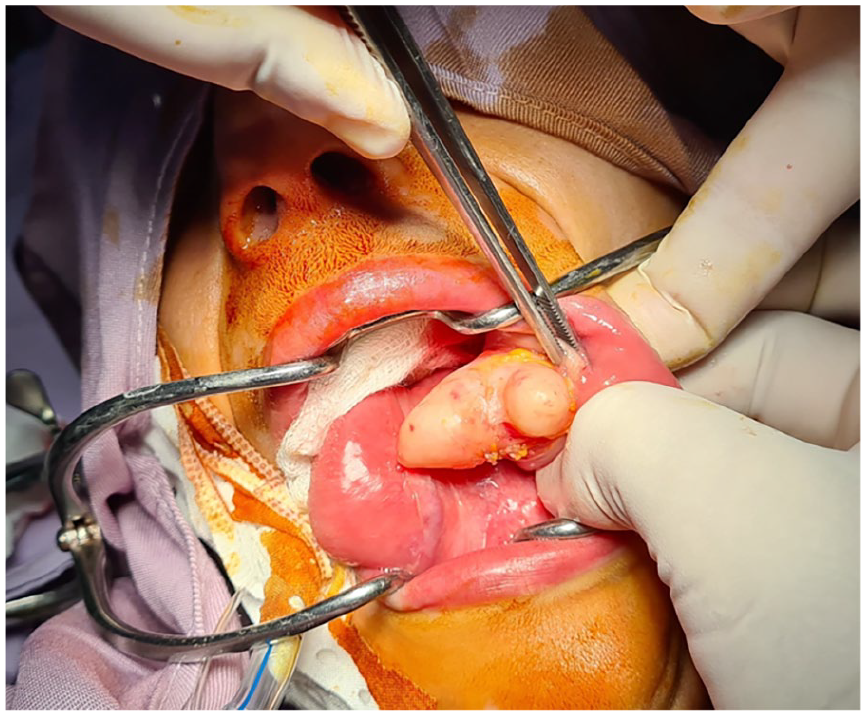
Preoperative view of endo-buccal excision of the tumor.

Macroscopic aspect of the tumor after excision.
Preoperatively, the neural origin of the tumor was suspected based on its clinical features, namely translucent appearance, yellowish coloration, and soft consistency.
Histological examination revealed a well-encapsulated benign tumor proliferation, with fasciculated architecture and variable cellular density, alternating between hypercellular and hypocellular areas. The fascicles occasionally exhibited a palisading pattern. The nuclei were regular, with no evidence of atypia or mitotic figures (Figures 3a and b).
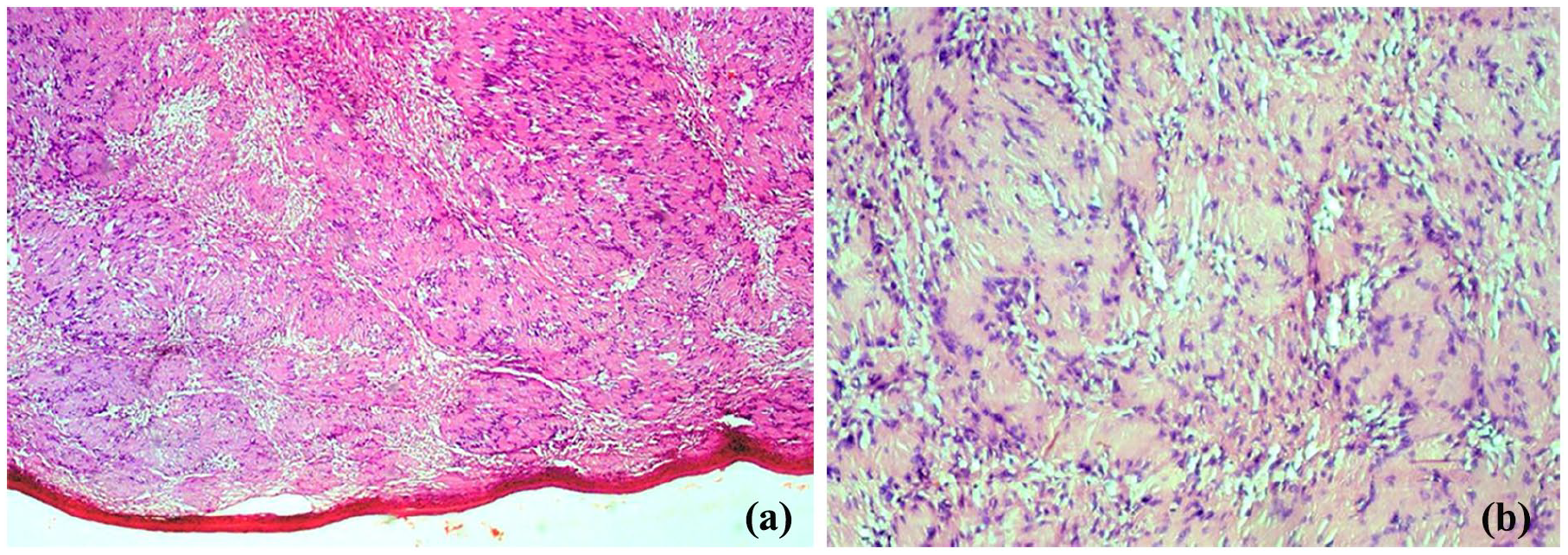
(a) Histological image of the tumor with hematoxylin–eosin staining (40× magnification) shows a well-encapsulated tumor proliferation. (b) A histological image of the tumor with hematoxylin–eosin staining (400× magnification) highlights the fasciculated architecture and palisading pattern of the tumor.
Discussion
Previously known as a neuroma, benign schwannoma is the most common nerve tumor. As a primary tumor of the peripheral nerves, it accounts for 1% to 2% of all soft tissue tumors. It is crucial to distinguish benign schwannomas and neurofibromas from malignant nerve tumors, which frequently occur in Recklinghausen’s disease. 5 Schwannomas must be also differentiated from neurofibromas and or other tumors that originate from nerve tissue, including intermediate-grade malignant nerve tumors or malignant tumors of the nervous system. 1
Schwannomas are generally solitary, sporadic, and idiopathic in over 90% of cases, although they may be associated with neurofibromatosis type 2 or schwannomatosis. 1 These are slow-growing tumors and are palpable when large or superficial. The onset of symptoms generally occurs over a prolonged period, often extending over several years. 5
Schwannomas are found in 25% to 45% of cases in the cervical region, with the majority originating from the vagus nerve (the 10th cranial nerve). 6 Although schwannomas are generally benign, rare cases of malignant schwannomas have been reported in the literature. 3
An exceptional location for schwannomas is the larynx, with laryngeal schwannomas being part of the various otorhinolaryngological localizations. 7 They rarely affect the mouth, particularly the tongue. Oral schwannomas typically arise from small nerves, which makes identifying the affected nerves challenging. 8
These tumors can occur subcutaneously, with a predilection for the head, neck, and flexural surfaces of the limbs. In deeper locations, they may involve the mediastinum or retroperitoneal region, developing from various plexuses. Schwannomas can also be found in the intradural region, affecting extra-medullary spinal nerves, and are referred to as “hourglass tumors.” 1
Other potential locations of these tumors include the cranial nerves: all can be affected except the first and the second cranial pair (I and II), with the eighth cranial nerve (VIII) being involved in more than 85% of cases, leading to the clinical presentation of acoustic neuroma. 1 Olfactory schwannomas are very rare since olfactory nerves lack Schwann cells, and the origin of these tumors remains unclear. 9
These tumors typically evolve very slowly, with progressive, painless growth over several years, which can delay diagnosis. 4
Schwannomas are often asymptomatic due to their slow progression and typically present with nonspecific clinical signs depending on the affected nerve. Symptoms may be sensory or motor. Schwannoma of the eighth cranial nerve (VIII) may present with vertigo and hearing loss.
Subcutaneous and deep lesions occur without specific clinical manifestations. Conversely, Schwannomas located in the spinal cord can cause radicular pain, movement disorders, dizziness, and numbness. 1
Schwannomas most commonly occur in individuals aged 20 to 40, with no gender predominance. 1
Objective sensory and motor deficits are rare due to the noninvasive nature of the tumor, which often results in normal electromyography. Computed tomography typically shows a dense, firm, homogeneous mass. 8 Magnetic resonance imaging (MRI) provides a more detailed view of the nerve tumor and can assist in diagnosis by revealing tumors with similar signals as muscle tissue on T1-weighted sequences and a markedly stronger signal on T2-weighted sequences. However, MRI cannot differentiate between neurofibromas and schwannomas. A histological examination is necessary to confirm the diagnosis. 5
Curative treatment involves the complete surgical removal of the tumor, which is almost always achievable. The surgical approach depends on the tumor’s location. For facial tumors, the intraoral (endo-buccal) approach is often preferred, as it minimizes the risk of facial nerve damage and avoids visible scars. 4
Unlike neurofibromas, schwannomas are not precursors to other tumors, and malignant transformation is rare. 10
Conclusion
Schwannomas are challenging to diagnose, due to their nonspecific clinical manifestations, which vary depending on the tumor’s location. They often present with a symptomatology that evolves gradually over several years. Treatment is exclusively surgical, focusing on the complete removal of the tumor. Cervicofacial schwannomas are very rare and have been reported in the literature only on rare occasions.
Footnotes
Acknowledgements
The authors would like to thank Dr Emna Nsiri for his kind assistance in the elaboration of this article.
Author Contributions
All the authors participated in the design, performance, analysis, and drafting of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.