
Abstract
Introduction
The open roof deformity remains a significant challenge in rhinoplasty procedures, necessitating nasal bone osteotomies to mitigate this complication. The efficacy and precision of osteotomies are pivotal factors in achieving successful postoperative outcomes. Beyond the patient’s cosmetic satisfaction, a desirable healing period entails reduced ecchymosis, minimal edema, and expedited recovery. Osteotomies are conventionally performed using traditional tools such as saws, chisels, and osteotomes or modernized with powered equipment. 1 Additionally, surgeons may opt for internal (intranasal) or percutaneous approaches, depending on their experience and preferences. 2
Despite advancements, conventional osteotomies still carry the risk of complications, including step deformity, over-resection, and asymmetry, even in the hands of seasoned surgeons. In contrast, contemporary osteotomy techniques employing electric instruments with reciprocating heads or piezoelectric-powered ultrasonic instruments allow for precise mobilization of nasal bones without the unpredictability of fractures. However, these powered instruments’ reliance on electricity may induce tissue reactions, trauma, or thermal necrosis. The setting period and instrument complexity can also extend operation time, often requiring a learning curve for optimal utilization. While existing literature presents limited studies demonstrating the superiority of modern equipment over conventional osteotomy techniques histologically, a conclusive preference for either approach still needs to be discovered.3,4
We posit that the healing process predominantly hinges on the osteotomy technique, emphasizing minimized damage and precise mobilization of the bony skeleton. A comparative histopathological and macroscopic examination of internal and external osteotomies, executed with conventional and powered instruments, is imperative. Thus, our study aimed to fill this gap by systematically evaluating and comparing these osteotomy techniques in a model, shedding light on their histopathological distinctions.
Materials and Methods
Animals
Ethics approval for this study was obtained from the Bagcilar Training and Research Hospital Experimental Animals Local Ethics Committee (2015-07). A total of 20 white New Zealand rabbits (10 male, 10 female) weighing 2.5 to 3.0 kg were included. The study adhered to all applicable institutional and national guidelines. Rabbits were individually housed in a controlled environment with a 12-hour light/12-hour dark cycle at 24℃ ± 2℃ and provided with a standard ad-lib pellet diet at the Bagcilar Research and Training Hospital Laboratory Animal Breeding and Experimental Studies Center in Istanbul.
Osteotomies
All rabbits underwent anesthesia with ketamine (35 mg/kg) and xylazine (5 mg/kg) administered intramuscularly. The frontonasal area was shaved, disinfected, and draped. Bilateral incisions superior to the nares were made, allowing the elevation of skin-subcutaneous tissues to expose the osseocartilaginous nasal pyramid fully (Figure 1). Each rabbit received 4 osteotomies: 2 20-mm-long parallel median osteotomies on the right nasal bone using a powered saw blade (external saw osteotomy [ESO]) and similar osteotomies on the left nasal bone using piezosurgery (PSO) (Piezosurgery Plus⁽R⁾; Mectron, Carasco, Italy). Internal chisel osteotomy (ICO) on the right side and external chisel osteotomy (ECO) on the left side were performed without elevating nasal mucosa, periosteum, or soft tissues. Incisions were closed, and rabbits were separated for reanimation.

Exposition of the nasal pyramid and completion of the osteotomies.
Histopathological Examination
Ten rabbits were sacrificed on the postoperative 7th day and the remaining 10 on the postoperative 15th day using intracardiac administration of a high-dose (120 mg) pentobarbital following anesthesia. Nasal bones were removed en bloc, fixed in 10% neutral buffered formalin for 72 hours, and decalcified in De Castro solution at room temperature for 4 weeks. The samples were processed (dehydrated in graded alcohols and cleared in xylene) using a vacuum tissue processor (Leica, Wetzlar, Germany) and embedded in paraffin blocks. Five micrometer thick serial sections were cut and stained with hematoxylin-eosin and Masson’s trichrome. All specimens were evaluated by 2 histologists who were blinded to the groups. Digital images were captured using a DFC7000T camera (Leica) connected to a light microscope (Leica DM6B), and digital images were used to evaluate the osteotomy gap width and bone regeneration by using an image analysis program (LAS version 3; Leica). The osteotomy gap width was assessed by measuring the length of the distance between the 2 native bone surfaces surrounding the osteotomy. The area of bone inside of the osteotomy (BA) and the total area of the osteotomy (TA) were measured. The percentage (BA/TA) was calculated to evaluate the bone regeneration in 15 day samples. 4
The defect areas in each sample were evaluated and semi-quantitatively assessed in terms of granulation tissue formation (GTF), vascularity, inflammation, and collagen fibril content. GTF was scored according to the percentage of the defect area covered by new granulation tissue as follows: Under the high-power field magnification area, less than 1% of the area was scored as 0, 1% to 30% as 1, 31% to 60% as 2, and more than 61% as 3. Vascularity was assessed by counting the number of blood vessels within a high-power field with scores as follows: 0 = none, 1 = 1 to 4 blood vessels, 2 = 5 to 10 vessels, and 3 = more than 10 vessels per high-power field. Inflammation was evaluated by the percentage of inflammatory cells within the total cell population of the defect area: 0 = 1% to 4%, 1 = 5% to 30%, 2 = 31% to 70%, and 3 = 71% to 100%. The collagen fibril content was scored as 0 = normal, 1 = slight, 2 = moderate, and 3 = severe increase in collagen fibrils. This scoring system was modified from those used by Abramov et al 5 and Tandelilin. 6
Statistical Analysis
SPSS 22 was utilized for statistical analysis (SPSS, IBM, Turkey). The Kruskal-Wallis test compared parameters between groups, while the Mann-Whitney U test identified differences in abnormal distribution. The Mann-Whitney U test compared results between the 7th and 15th days. The chi-squared and Fisher-Freeman Halton tests were employed for qualitative data comparison. Significance was determined at P < .05.
Results
Early-bone healing and regeneration using 4 different osteotomy techniques were examined in the defect sites of 7- and 15-day samples (Figure 2). The bone defects created by different techniques showed regular shapes and well-defined edges. The bone fragments and connective tissue with high cell density filled the defect areas by day 7 (Figure 3). The cell-rich areas surrounding the blood vessels and osteoid tissue islands were prominent in the defect area of PSO by day 7. The collagen fibers were thin and loosely arranged in both ICO and ECO.
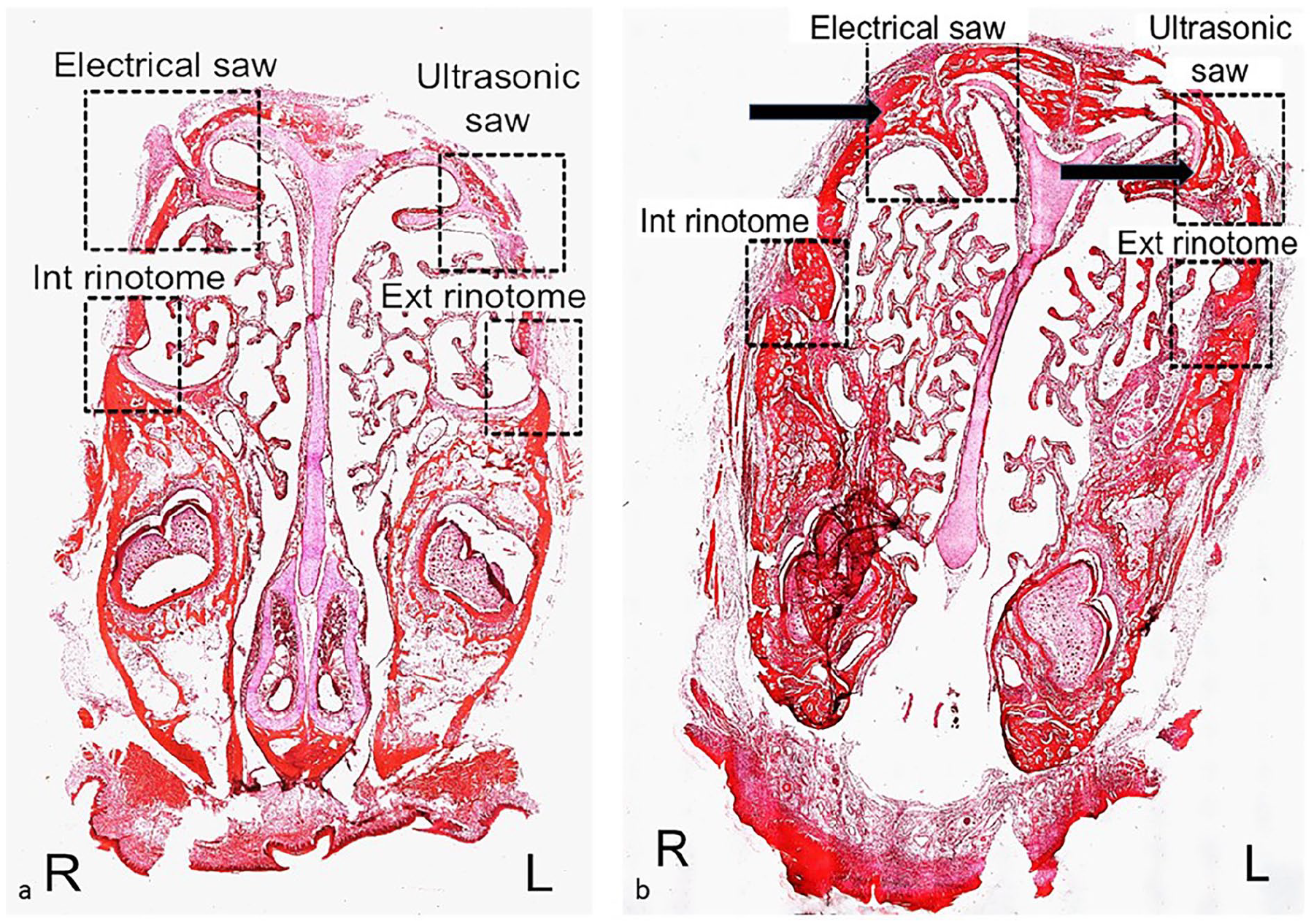
10× magnification of the 4 osteotomies on the (a) 7th and (b) 15th days.
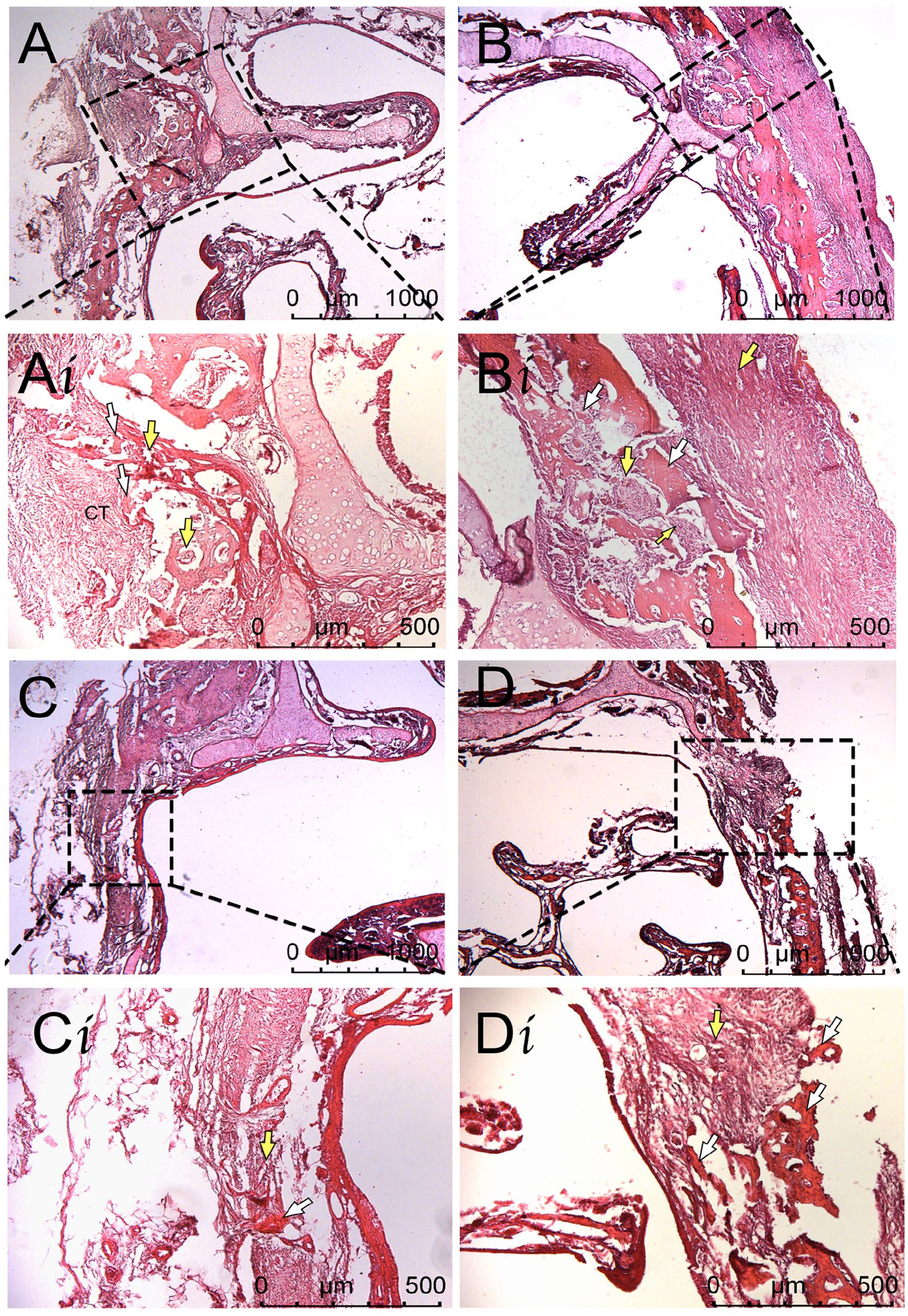
Representative micrographs showing osteotomy areas in experimental groups by 7 days. The bone fragments and fibrous connective tissue were filling the defect areas. Bone fragments (white arrow) with empty lacunas, blood vessels (yellow arrow). A, Ai: electrical saw (ESO); B, Bi: piezo (PSO); C, Ci: internal chisel osteotomy; D, Di: external chisel osteotomy (hematoxyline-eosin). CT, connective tissue.
In the samples of 15 days, the newly-formed bone and the fibrous connective tissue are observed in the defect sites. The bone debris was reduced, a single layer of osteoblasts with a cuboidal shape covered the trabecula, and the new bone lined by osteoblasts was prominent around the trabeculas. The fibrovascular stromal spaces between irregular trabecula are wider in ESO than in PSO. The perpendicularly-oriented thin long bone trabeculas were present in the osteotomy gap of PSO by day 15. In ICO and ECO, well-organized fibrous connective tissue surrounded the newly-formed bones (Figure 4). High bone remodeling activity is observed in PSO due to prominent osteoclasts (Figure 5).
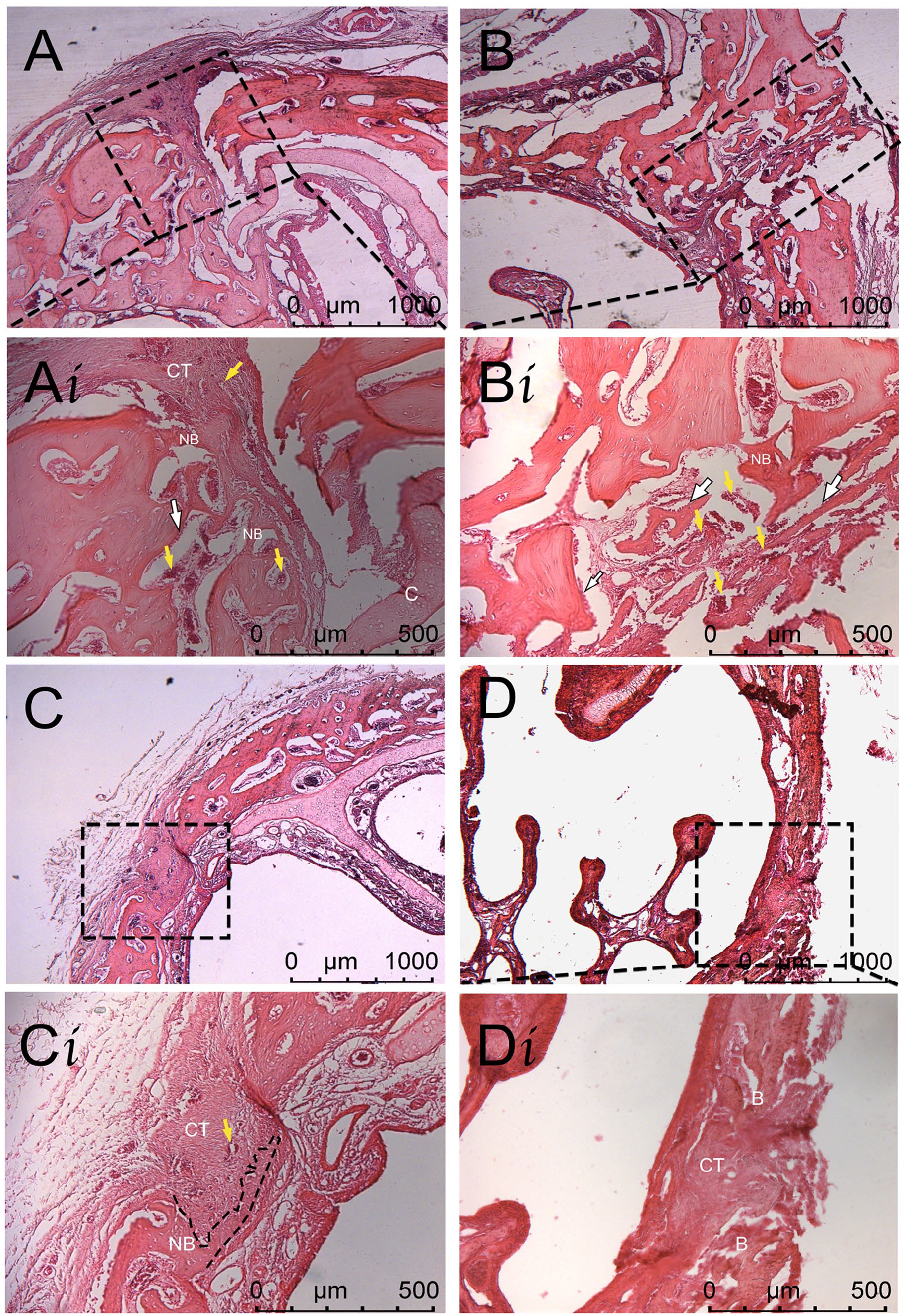
Representative micrographs showing defect areas in experimental groups by 15 days. The new bone formation is seen in the defect areas. CT: connective tissue, blood vessels (yellow arrow), osteoblasts (white arrow); A, Ai: electrical saw (ESO); B, Bi: piezo (PSO); C, Ci: internal chisel osteotomy; D, Di: external chisel osteotomy (hematoxylin-eosin). B, bone; NB, new bone.
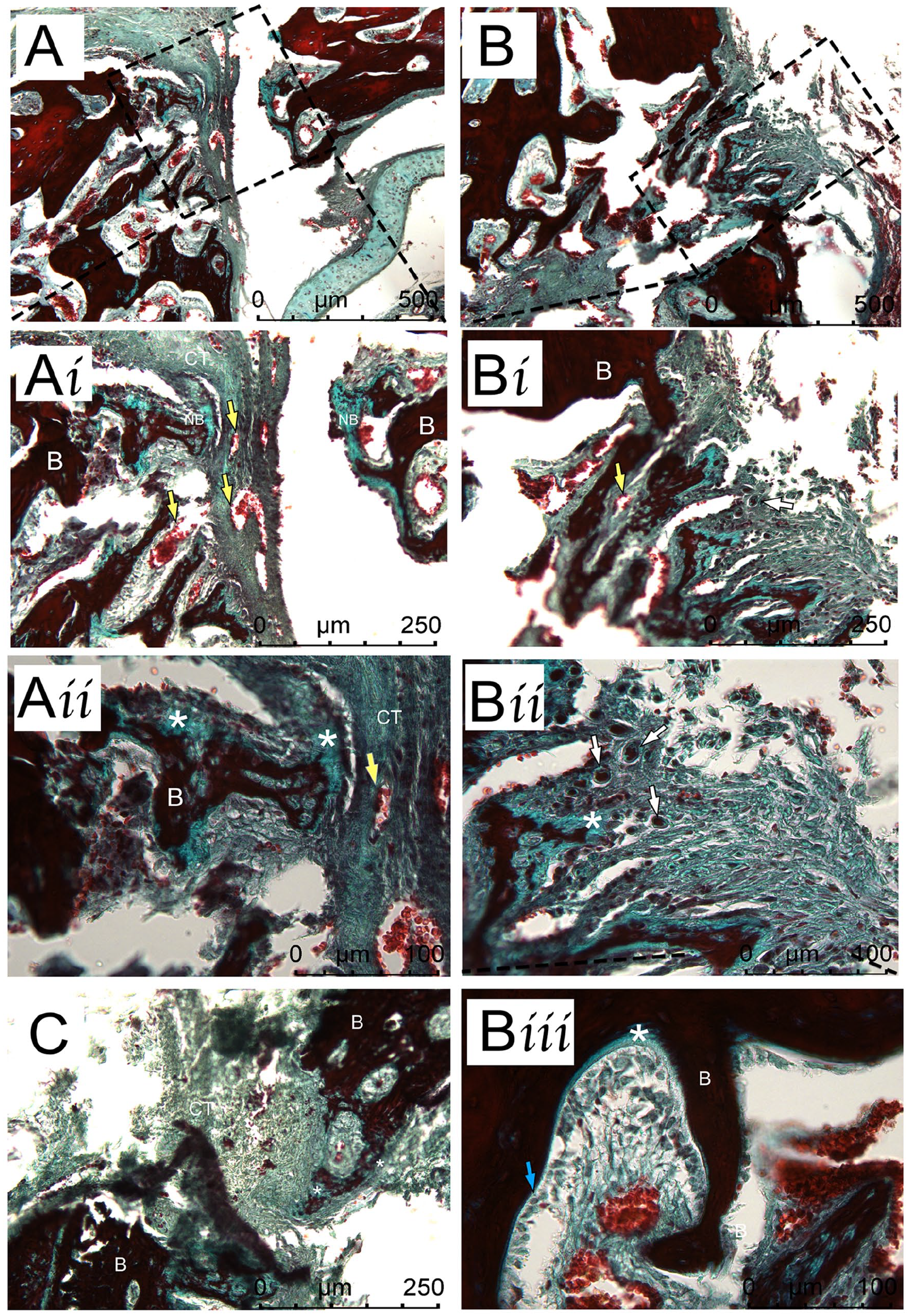
Representative micrographs showing new bone formation in the defect areas in experimental groups by 15 days. The new bone lined by osteoblasts in green, and the relatively-mature remodeled bone in red. CT, connective tissue, blood vessels (yellow arrow); asterisks, new bone, osteoclasts (white arrow), osteoblasts (blue arrow); A, Ai, Aii: electrical saw (ESO); B, Bi, Bii, Biii: piezo (PSO); C: internal chisel osteotomy (Masson’s trichrome). B, bone.
Granulation Tissue Formation
On the 7th day, the GTF for ICO was significantly lower than ESO or piezosurgery osteotomy (PSO) (P1 = .013*, P2 = .036*). Similarly, GTF on the 7th day in external chisel osteotomy (ECO) was significantly lower than ESO or PSO (P1 = .011*, P2 = .017*). No significant difference existed between GTF on the 7th day for ESO and PSO (P = .076), and ICO and ECO were comparable (P = .085) (Table 1). Intergroup comparisons showed no significant difference in GTF on the 15th day among the osteotomies (P = .084). ICO GTF remained statistically consistent between the 7th and 15th days (P = .549), as did ECO GTF (P = .429). Conversely, PSO GTF was higher on the 7th day and gradually decreased on the 15th day (P = .036*) (Table 1).
Evaluation of Granulation, Vascularization, Inflammation, Collagen Fibril Content Among Groups.
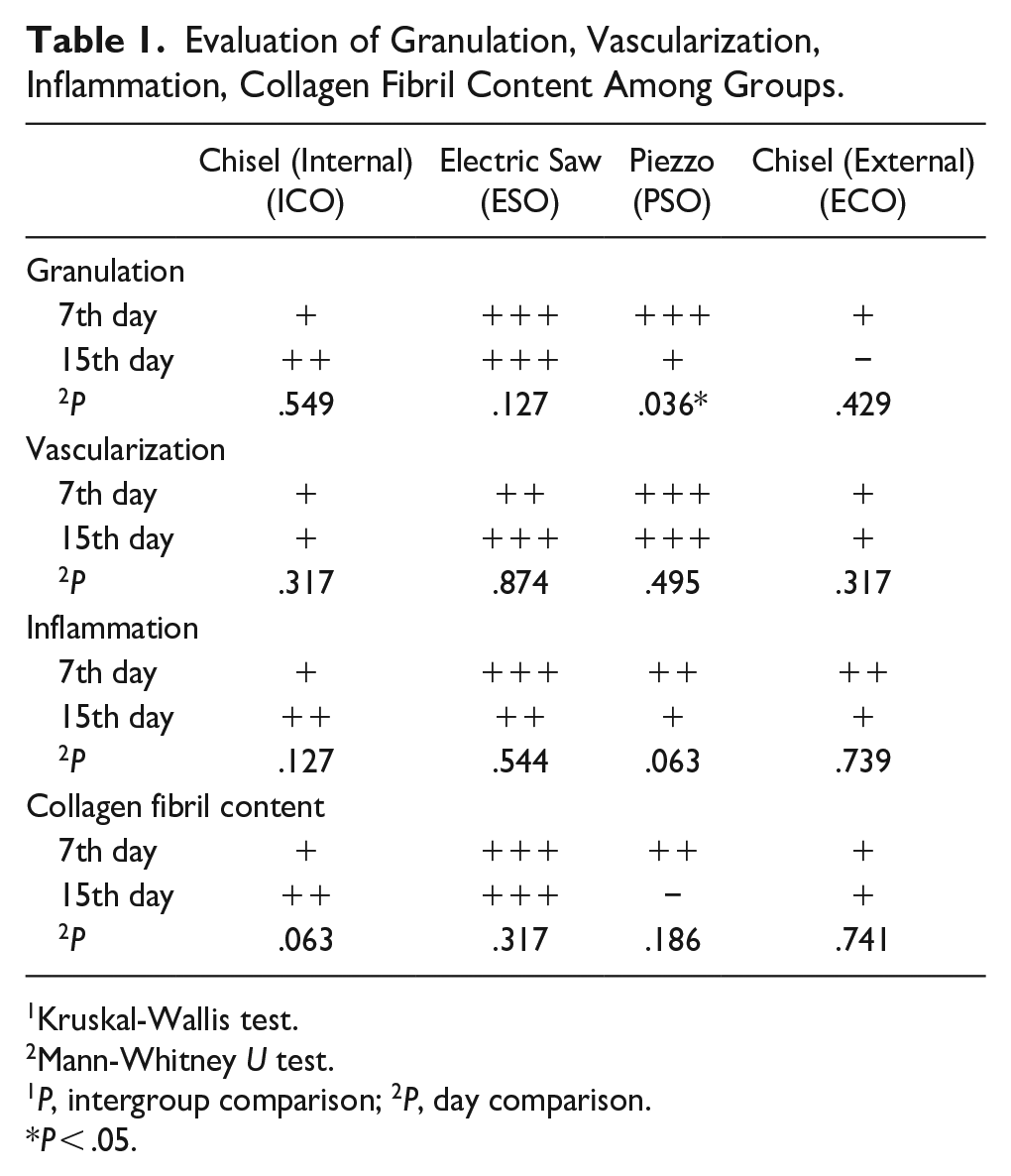
Kruskal-Wallis test.
Mann-Whitney U test.
1P, intergroup comparison; 2P, day comparison.
P < .05.
Vascularization
Vascularization (VSC) was prominent in PSO and ESO, while slight blood vessels were observed in ECO and ICO on the 7th day. The intergroup comparisons of VSC were statistically significant (P = .004*). VSC in ICO and ECO were significantly lower than in ESO or PSO (P = .011 and P = .013, respectively). The 7th day VSC between ESO and PSO was not significant (P = .128), and similarly, the 7th day VSC between ECO and ICO was not significant (P = .246). All osteotomy types exhibited nonsignificant VSC between the 7th and 15th days (all P > .05, Table 1).
Inflammation
On the 7th and 15th days, no statistically-significant difference emerged between the 4 osteotomy types (all P > .05).
Collagen Fibril Content
On the 7th day, collagen fiber content (CFC) was significantly higher in ESO than in the other 3 osteotomies (ICO P = .013, PSO P = .011, ECO P = .011). No significant CFC difference existed between ICO and ECO on the 7th day (P = .244).
CFC on the 15th day was insignificant between the osteotomies (all P > .05). CFC between the 7th and 15th days was also not significant (all P > .05).
The Osteotomy Gap and BA/TA %
The osteotomy gap width and the percentage of BA/TA were evaluated in 15 day samples (Figure 6), and the osteotomy gap width was highest in ECO (755.075 ± 89.656 µm) and lowest in the PSO (454.943 ± 21.895 µm). The percentage of BA/TA was high in PSO (35.75 ± 11.870) and was lower in ESO, ICO, and ECO (27.5 ± 5.259; 19.25 ± 4.645; 20.5 ± 5.802, respectively; Table 2).
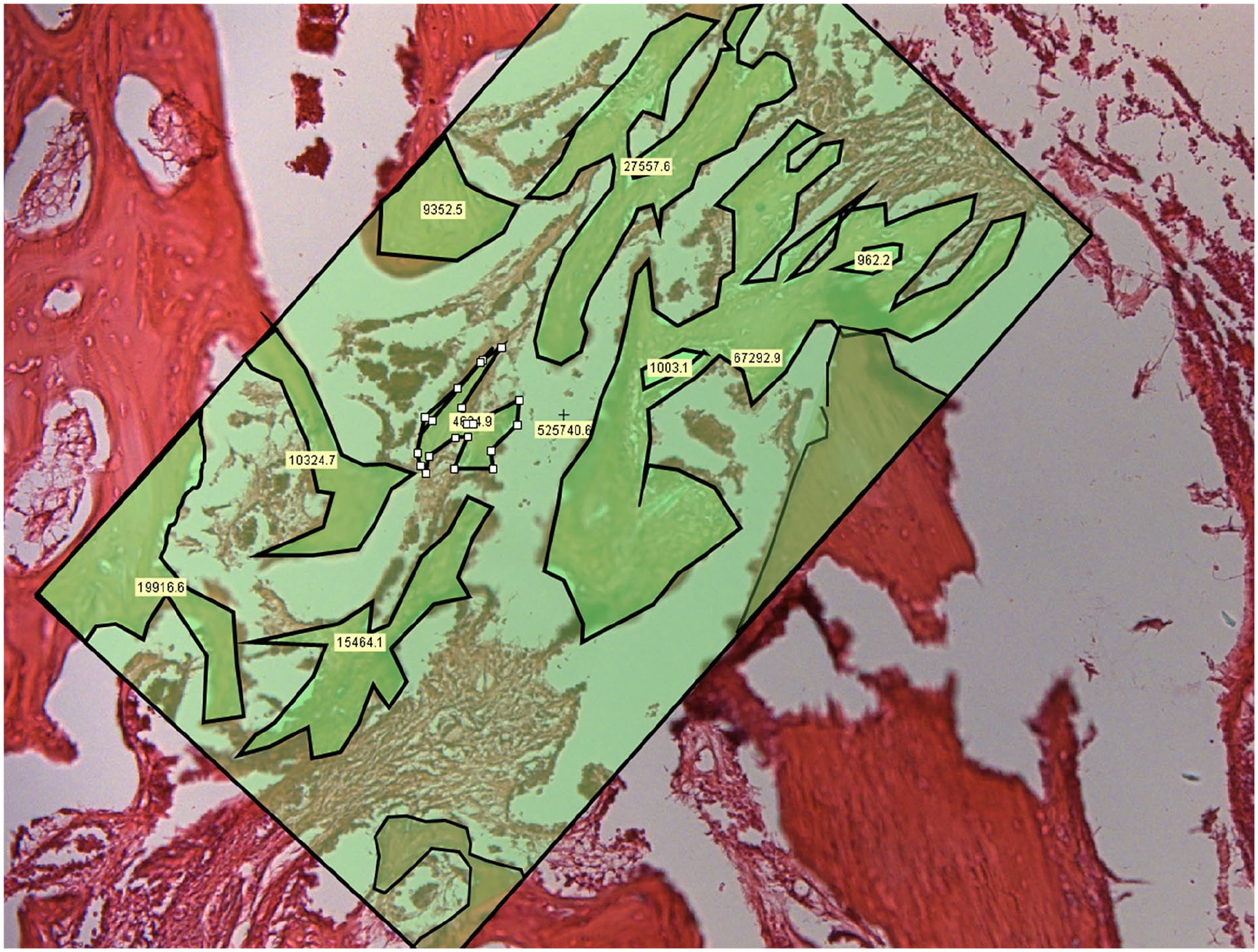
A representative micrograph was used for histomorphometric evaluations of BA/TA %. The rectangle marks the total area of osteotomy (TA); the regenerated bone areas (BA) are outlined in black.
Histomorphometric Analysis for Different Osteotomies.
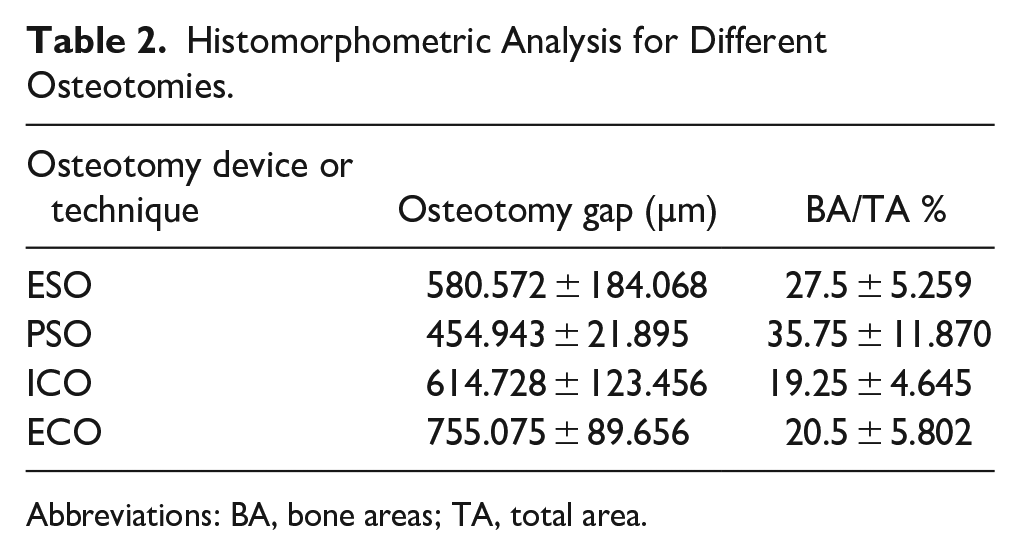
Abbreviations: BA, bone areas; TA, total area.
Discussion
In rhinoplasty, nasal bone osteotomies play a pivotal role in shaping the nose and directly influencing surgical outcomes. Choosing between internal and external techniques and selecting conventional or powered instruments significantly impacts both cosmetic results and functional aspects. Inadequate narrowing of the bony vault can lead to functional deformities that compromise the overall aesthetic outcome. Thus, carefully selecting the surgical technique and instrumentation becomes paramount, ensuring optimal results while preserving the integrity of the nasal mucosa and periosteum. 7
Over the past decade, advancements in surgical instruments have aimed to minimize soft tissue damage and enhance the precision of nasal bone cutting.8-10 The introduction of powered saws, as reported by Giampapa and DiBernardo in 1993, demonstrated efficacy in achieving well-defined and precise lateral osteotomies, improving patient comfort, and reducing complications. 8 Conversely, Piezoelectric surgery, championed by Robiony et al, 9 offered a minimally-invasive approach with ultrasonic vibrations, preserving soft tissues during osteotomies. 6 In a previous Ma et al 11 study, piezosurgery and conventional osteotomy healing patterns were compared in an animal model. The results showed no significant difference between these techniques. In a Kocak et al 12 study, piezosurgery and internal osteotomy conventional techniques were compared regarding patients’ clinical outcomes such as postoperative ecchymosis, edema, pain, and mucosal integrity. Piezosurgery was safe, effective, and precise, with less pain, ecchymosis, and edema than conventional osteotomy. However, histopathological features were not evaluated. More studies that compare piezosurgery and conventional osteotomies stated the common advantage of piezosurgery was less postoperative ecchymosis and edema.13-15 Nevertheless, every technique has its advantages and disadvantages. Therefore, there is still a significant controversy over the optimal instrument and method for osteotomies.
To the best of our knowledge, there was no published data to support the bone healing process microscopically. Our results showed that GTF and VSC in PSO and ESO were higher than the classical chisel technique, which implied a better healing process overall.
Many studies have also compared internal and external lateral osteotomy; however, there is no consensus regarding the best choice. Sinha et al 2 compared external and internal osteotomies in 45 patients and found that nasal mucosal injury, postoperative, and edema were less in the external osteotomy group. Ogden et al 16 compared bone healing of endonasal and percutaneous lateral osteotomy histopathologically in rabbits. They found that percutaneous lateral osteotomy results in less period and bone trauma and better bone healing than endonasal osteotomy. 16 Mottura 17 elevated the external period and internal mucoperiosteum before osteotomy and then used a double-guarded osteotome for internal lateral osteotomy. He claimed that this method offered less mucosal trauma as well as reduced postoperative ecchymosis and edema.
Our study adds valuable microscopic insights into the bone healing process, a facet largely unexplored in existing literature. Results demonstrated higher GTF and VSC in PSO and ESO compared with the classical chisel technique, indicative of an overall superior healing process. The advantages of piezosurgery, including reduced postoperative ecchymosis and edema, align with previous studies, emphasizing its safety, effectiveness, and precision.
While debates persist over internal and external lateral osteotomy techniques, our study found no histological difference between the approaches.18,19 Further clinical studies are warranted to evaluate postoperative factors such as bruising, edema, and swelling. Additionally, the choice between open and closed techniques should be tailored to the surgeon’s experience, as Kilic et al 20 reported. Our histopathological examination did not assess these postoperative factors, underscoring the need for complementary clinical studies to determine the optimal osteotomy technique.
Animal models, such as sheep and rabbits, have been extensively employed to study bone healing. In our study, the bone healing process was more distinctly delineated in powered instruments than in conventional techniques. The sample size was adequate for conclusive comments on histopathological findings. However, further clinical investigations, including patient satisfaction and quality of life assessments, are essential to comprehensively understand the ideal osteotomy technique in rhinoplasty.
Conclusion
Our histopathological study comparing various nasal osteotomy techniques in a rabbit model provides valuable insights into the bone healing process. PSO and ESO demonstrated superior GTF and VSC compared with the classical chisel technique on the 7th day, suggesting a more favorable healing trajectory. We chose the 2 week mark for the sacrifice of the animals and analysis. We have indicated that the most apparent difference may be seen at this period. This idea was supported by the results showing less traumatic procedure with PSO than with ESO regarding demonstrated superior GTF and VSC.
The ongoing debate regarding internal versus external osteotomy techniques did not reveal histological differences in our study. However, it is essential to note that our investigation focused solely on microscopic aspects, and further clinical studies are warranted to evaluate postoperative factors such as bruising, edema, and swelling.
The advantages of piezosurgery, including reduced postoperative ecchymosis and edema, align with existing literature, supporting its safety, effectiveness, and precision. While each technique has its own advantages and disadvantages, our study contributes to microscopically understanding the bone healing process.
Future research endeavors should encompass larger clinical studies, incorporating patient satisfaction and quality of life assessments, to provide a comprehensive evaluation of the optimal nasal osteotomy technique in rhinoplasty. The findings from this study offer a foundation for further exploration, paving the way for advancements in surgical techniques that prioritize both aesthetic outcomes and patient well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
All procedures performed in studies involving animals were following the ethical standards of the institution or practice at Bagcilar Training and Research Hospital Experimental Research and Skills Development Center (2015, n◦ 2015-07). All applicable international, national, and/or institutional guidelines for the care and use of animals were followed.
Informed Consent
For this study, informed consent is not required.