
Abstract
Keywords
Introduction
Chronic lymphocytic leukemia (CLL) is a slowly progressive disease that typically affects older adults, with a median age of 70 at the time of diagnosis. 1 CLL is the most common leukemia in Western countries, responsible for 1.0% of all new cancer diagnoses in the United States. 1 Although CLL is typically identified incidentally on routine blood work, unique manifestations of the disease have been described both at the time of diagnosis and in the setting of indolent disease.2,3 We will present the orbital and sinonasal disease manifestations of 3 CLL patients. Although encountered infrequently, it is important for otolaryngologists to be cognizant of the orbital presentation of CLL. Any suspicion of the disease should trigger prompt referrals to hematology and oncology and clinically relevant surgical specialties.
Literature Review
Prior literature well characterizes orbital manifestations of CLL; however, sinonasal presentations are more rarely described. A systematic review of 123 cases examined ophthalmic involvement in patients with CLL. 4 Ophthalmic symptoms were the first manifestation of CLL in approximately 25% of patients, revealing a Richter’s transformation in 11%. 4 Symptoms were most commonly due to CLL-related infiltration, followed by lymphoma and infection. Prior case studies have found acute sinusitis and blindness as the first presentation of CLL, resulting in unusual presentations of a typically indolent disease process. 5 One such patient presented with bilateral ptosis that developed over a 2-month period, with biopsies of the anterior orbital fat revealing a dense infiltrate of small lymphocytes consistent with B cell CLL. 6
Sinonasal manifestations of CLL have been less commonly described in the literature. One case report described chronic rhinitis refractory to typical medical treatment as a defining symptom in CLL recurrence. 3 Another case series found CLL infiltration of the oropharynx and paranasal sinuses in less than 1% of CLL cases. 7 Retrospective analysis of 25 patients with specific head and neck involvements led to the characterization of nasal-associated lymphoid tissue (NALT) CLL. 8 These patients presented with symptoms including chronic cough, anteroposterior nasal discharge, nasal congestion, and pharyngitis. 8 This study demonstrated a worse prognosis with NALT CLL due to increased treatment requirements and more progressive disease. 8
Findings
Case 1
A 78-year-old male with a history of CLL presented to oculoplastic surgery for evaluation of binocular diplopia with right-sided restricted supraduction, 5 mm right-sided proptosis, hypoglobus, and worsening chronic epiphora. His oncologic markers had been stable for close to 17 years on routine disease monitoring. Imaging revealed a right frontal mucocele measuring 2.7 cm in contact with the medial aspect of the right globe with evidence of mass effect and mild proptosis. Heterogeneous opacification of the bilateral frontal, maxillary, and anterior ethmoid sinuses was also noted (Figure 1). Based on these imaging findings, the patient was referred to otolaryngology. Nasal endoscopy was performed which showed middle meatal polyposis bilaterally. A tissue biopsy revealed CLL. The patient underwent bilateral endoscopic sinus surgery and was started on daily steroid sinus rinses. Surgical pathology demonstrated sinonasal mucosa with small, monotonous lymphocytic infiltrate (Figure 2). Flow cytometry was CD5 positive, and immunohistochemistry testing was negative for cyclin D1, consistent with a diagnosis of small lymphocytic lymphoma or CLL.
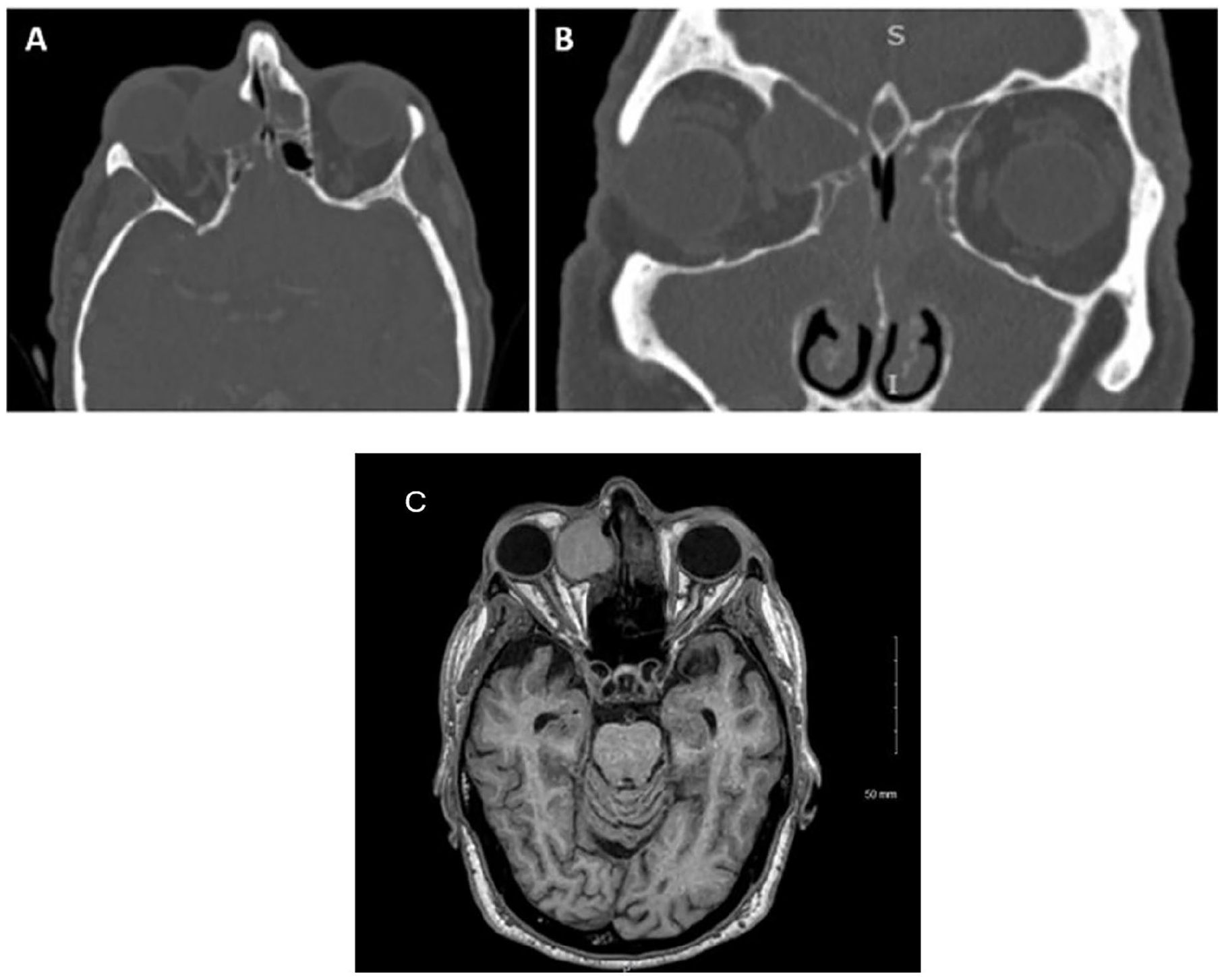
Axial (A) and coronal (B) CT showing bilateral sinusitis with right-sided mucocele with mass effect on the globe and associated proptosis. Axial T1 MRI (C) showing right-sided mucocele with mass effect on the globe and associated proptosis.
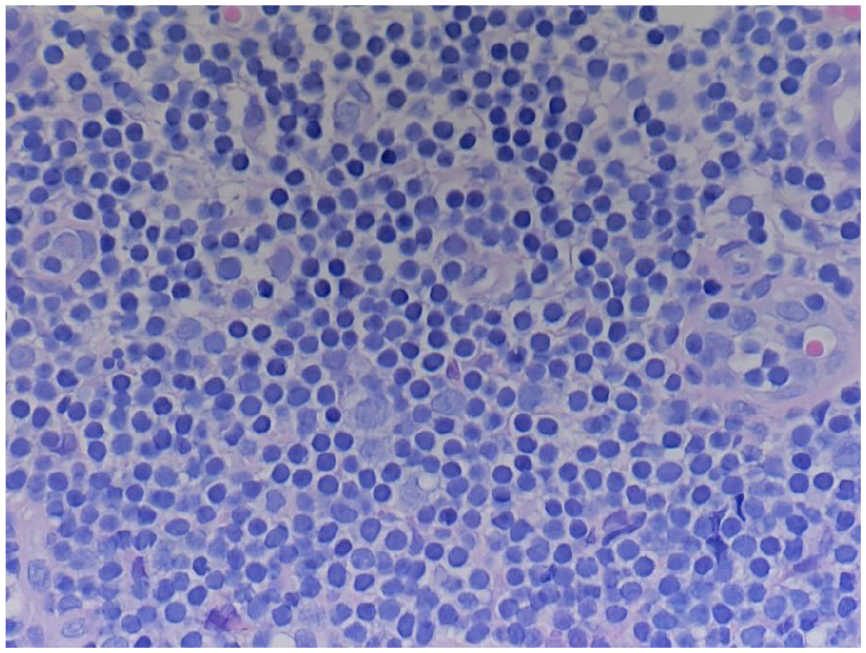
Section of sinonasal mucosa with an infiltrate consisting of small, monotonous lymphocytes.
The patient had full resolution of his diplopia postoperatively. Endoscopy performed 9 months after surgery demonstrated healthy mucosa and a patent right frontal sinus. The patient was evaluated by hematology and oncology in the postoperative period. Computed tomography (CT) chest, abdomen, and pelvis demonstrated disease above and below the diagram. Despite this, active monitoring with laboratory work and nasal endoscopy every 6 months was recommended. Three years after surgery, the patient had no evidence of sinonasal disease recurrence on endoscopy and did not require initiation of systemic therapy.
Case 2
A 73-year-old female with a history of chronic sinusitis and CLL was evaluated by ophthalmology for bilateral epiphora. Conjunctivochalasis with increased vascularity was noted in the left eye, prompting a biopsy that demonstrated CLL.
Regarding her CLL history, she was initially diagnosed 15 years prior to the inguinal lymph node biopsy. She was treated with fludarabine and Rituxan several years after diagnosis due to increased lymphadenopathy with clinical improvement in symptoms.
At the time of the ophthalmology consultation, she was receiving infusions of intravenous immunoglobulin (IVIG) for infection prophylaxis in the setting of hypogammaglobulinemia but was not undergoing treatment for CLL. From an otolaryngologic standpoint, the patient had undergone functional endoscopic sinus surgery (FESS) 2 years prior for chronic non-allergic pansinusitis refractory to medical management.
Three weeks after conjunctival biopsy, she developed a left dacryocystitis which was effectively treated with systemic antibiotics. At the time of subsequent oculoplastics evaluation, she was found to have nasolacrimal duct obstruction likely secondary to CLL given the patient’s prior conjunctival biopsy pathology. Endoscopic dacryocystorhinostomy (DCR) was recommended and the patient was referred to otolaryngology for surgical consultation. Upon assessment, the patient reported persistence of nasal congestion and nasal drainage status post-FESS which was refractory to daily saline sinus rinses with steroid nasal spray. Her CT sinus showed severe pan-sinus mucosal thickening with near-complete opacification of the right maxillary sinus (Figure 3). It was hypothesized that the patient’s compromised immunologic status predisposed her to sinusitis. The patient underwent left endoscopic DCR and bilateral FESS with the pathology of all sinonasal specimens showing small lymphocytic lymphoma (Figure 4).
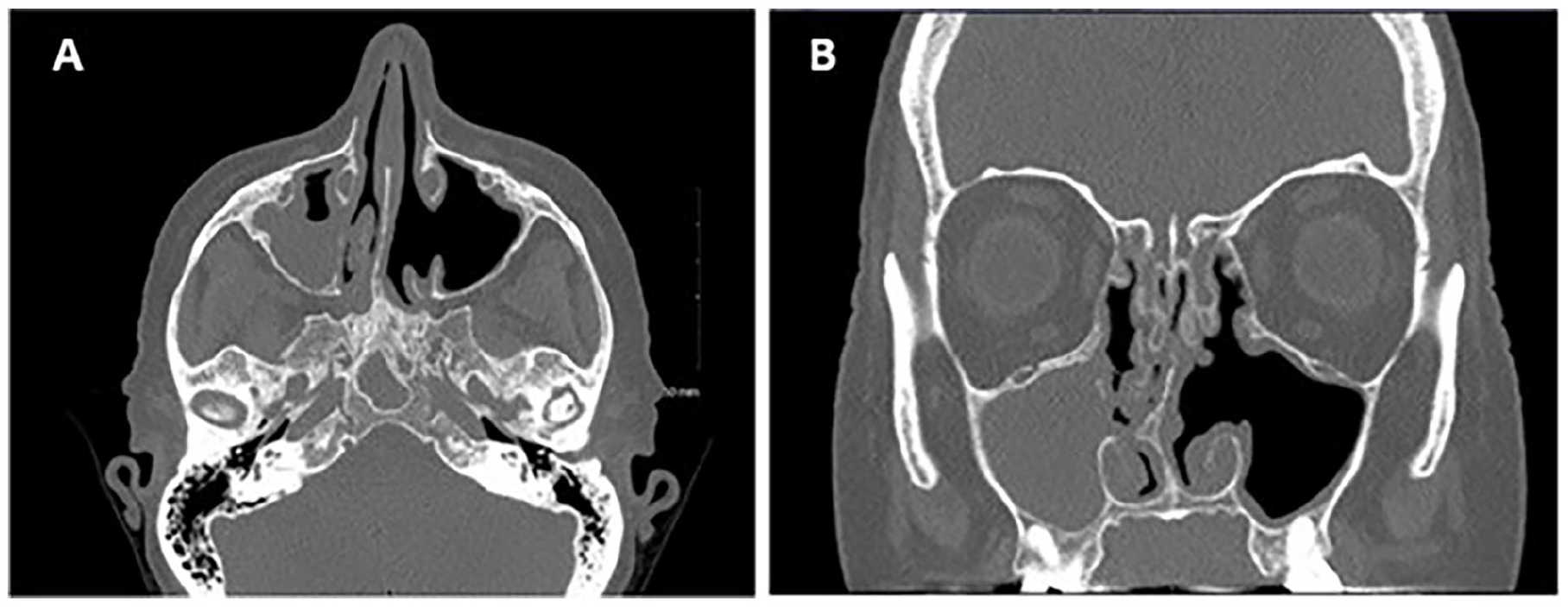
Axial (A) and coronal (B) CT showing evidence of prior ESS and opacification of the right maxillary sinus.
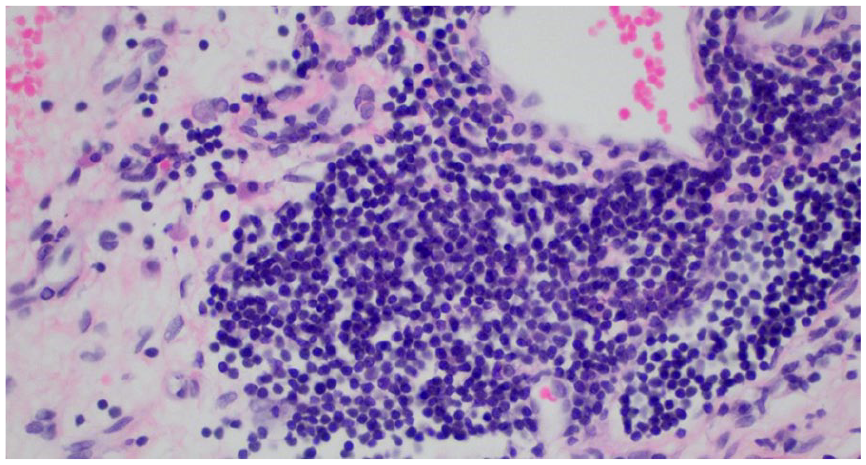
Section of sinonasal mucosa with infiltrate consisting of small lymphocytes consistent with small lymphocytic lymphoma.
Following surgery, she was started on daily steroid rinses. At the 3-week follow-up appointment, her lacrimal and nasal symptoms had nearly resolved. The patient had no further episodes of dacryocystitis. She was started on bendamustine and obinutuzumab by her hematologist for progressive disease as full body imaging revealed diffuse adenopathy. A post-treatment CT showed a resolution of adenopathy. She continues to be treated medically for chronic sinonasal symptoms with daily steroid topical rinses and intermittent antibiotic use as needed for recurrent infections. She is also being treated with regular IVIG infusions to address her hypogammaglobulinemia.
Case 3
A 59-year-old male with a history of CLL presented to the oculoplastic surgery clinic with left-sided epiphora and new-onset anosmia. He had undergone a left-sided DCR for treatment of epiphora secondary to nasolacrimal obstruction 1 year prior which provided symptomatic relief for several months. Regarding his history of CLL, the patient was diagnosed 7 years earlier on laboratory work which revealed a leukocytosis. Imaging showed splenomegaly without adenopathy; thus, no treatment was recommended. The ophthalmologic evaluation confirmed recurrent left-sided nasolacrimal duct obstruction. The patient was referred to otolaryngology for consideration of endoscopic DCR and evaluation of anosmia.
During otolaryngologic assessment, the patient reported a several-year history of nasal obstruction which responded well to nasal decongestant spray. In-office nasal endoscopy demonstrated bilateral turbinate hypertrophy and mild rightward septal deviation. There was bilateral middle turbinate head edema, but no polyps or drainage were identified. He was diagnosed with allergic rhinitis and rhinitis medicamentosa and advised to discontinue nasal decongestant use and to begin steroid saline sinus rinses. A sinus CT showed no evidence of sinus disease; therefore, FESS was not pursued (Figure 5A). A left DCR with bilateral inferior turbinate reduction was recommended to address his symptoms of nasal obstruction and epiphora. Intraoperatively, friable nasal mucosa and a polypoid appearance of the left lacrimal sac were observed. Surgical pathology of the nasal mucosa and tissue from the left lacrimal sac revealed a sheet-like proliferation of small lymphocytes consistent with CLL (Figure 5B). Flow cytometry stained positive for PAX-8, CD5, and CD43 (Figure 5C).
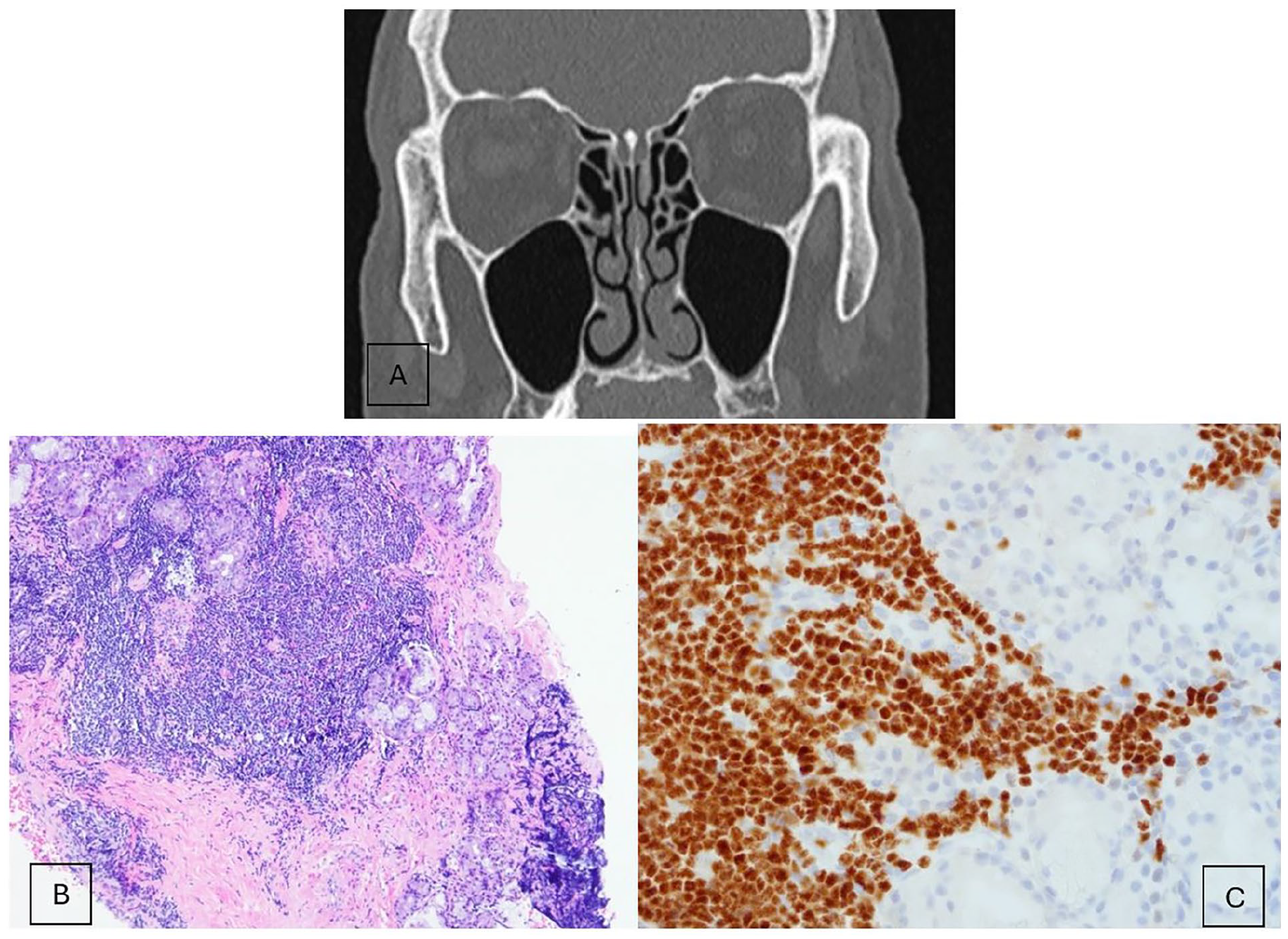
Coronal CT sinus (A) demonstrating clear paranasal sinuses with a narrow nasal airway. Section of left nasal cavity mucosa (B) demonstrating sheet-like proliferation of small lymphocytes that have round to slightly irregular nuclear contours, clumped chromatin, and scant cytoplasm. Slide demonstrating PAX-5+ staining (C).
Following surgery, he was started on daily steroid rinses. At his 6-week follow-up appointment, he noted improvement of epiphora and nasal congestion. His sense of smell remained diminished, although the degree of inflammation within his nasal cavities significantly improved. At his 6-month follow-up, his sense of smell remained blunted, but his presenting symptoms of epiphora and nasal obstruction had resolved completely. He was started on ibrutinib by hematology and oncology after a bone marrow biopsy showed 80% CLL and the patient had developed significant B symptoms such as severe night sweats and fatigue.
Discussion
CLL is the most common leukemia in western countries and typically affects older adults. 1 As discussed, although CLL is most often identified incidentally on routine blood work, unique manifestations of the disease are possible both at the time of diagnosis and in the setting of stable disease.2,3 In this case series, we present 3 CLL patients with previously indolent disease who were found to have disease progression within the orbit, nose, and paranasal sinuses after initially presenting with common ophthalmologic complaints such as diplopia, proptosis, epiphora, and recurrent dacryocystitis. Given the propensity for CLL to infiltrate the orbit and cause symptoms, awareness of risk factors and prompt recognition of disease by otolaryngologists with referral to ophthalmology is crucial for facilitating appropriate intervention. 4
Autopsy studies have shown ocular and periocular involvement of chronic leukemia in up to 75% of patients.9,10 Diplopia and proptosis are among the most common reported orbital manifestations of CLL. 9 Another common ophthalmologic condition associated with CLL orbital involvement is dacryocystitis. Workup for obstructive causes should be performed in all patients presenting with dacryocystitis and epiphora, especially patients with a diagnosis of CLL, as disease infiltration of the lacrimal sac is a known ophthalmologic manifestation. 9 Rarely, chronic rhinitis has been a presenting symptom of sinonasal CLL. 10 The constellation of symptoms including epiphora, dacryocystitis, and rhinitis in a patient with a history of CLL should prompt further evaluation and work-up for the progression of the disease. Although rare, orbital and sinus manifestations of CLL may have clinically significant consequences such as permanent vision loss, orbital cellulitis, and brain abscess formation.4,9
Conclusions
The 3 cases described involved CLL patients with no active treatment for many years who presented with isolated orbital and nasal complaints and no concerns for systemic symptoms. All patients were evaluated by hematology and oncology after diagnosis and 2 were found to have progressive disease with bone marrow involvement, lymphadenopathy, and blood work derangements which required further systemic treatment. Without proper diagnosis of their ophthalmologic symptoms, identification of global disease progression and initiation of systemic treatments would have likely been delayed. These 3 cases underscore the importance for otolaryngologists to be suspicious of local disease metastasis in CLL patients who present with new onset ophthalmologic symptoms.
Footnotes
Author Contributions
D.B.: Conceptualization, Methodology, Writing—Original draft. A.S.: Writing—Original draft. K.M.: Conceptualization, Methodology, Writing—Original draft. A.R.: Conceptualization, Methodology, Writing—Original draft. C.R.: Methodology, Data curation. P.A.: Methodology, Data curation. E.H.: Writing—Review and editing. C.O.: Conceptualization, Methodology, Writing—Review and editing.
Data Availability Statement
The data used to support the findings of this case series are included in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Our institution does not require ethical approval for reporting individual cases or case series.
Patient Consent
Verbal and written informed consent was obtained from the 3 patients included for their anonymized information to be published in this article.
Method of Literature Search Statement
The literature search was conducted through a thorough examination of case series and research studies related to ocular involvements and manifestations of chronic lymphocytic leukemia on PubMed and Google Scholar databases.