
Abstract

Significance Statement
Pneumoparotid is a rare yet significant condition predominantly affecting individuals involved in activities that increase intraoral pressure, such as wind instrument playing. Understanding its etiology and risk factors is essential for early diagnosis and effective management, preventing chronic complications and improving patient outcomes. This report highlights the importance of recognizing occupational hazards and implementing preventative measures to mitigate the impact of this condition on at-risk populations.
A 31-year-old man without chronic diseases or a family history of illness, who works as a suona player, presented with intermittent left cheek swelling that began a year ago when playing the instrument. He came to our hospital and reported that his cheek swelled and became painful after playing suona and required manual pressure to subside (Supplemental File, Video). He had no recent dental surgeries, fever, or symptoms of upper airway infection. Physical examination of the oral cavity revealed no abnormalities. A computed tomography (CT) scan revealed air in the parotid gland and parotid duct (Figure 1) which is compatible with the diagnosis of pneumoparotid. The patient originally worked 6 to 8 hours daily, but his symptoms resolved completely after reducing his playing frequency.
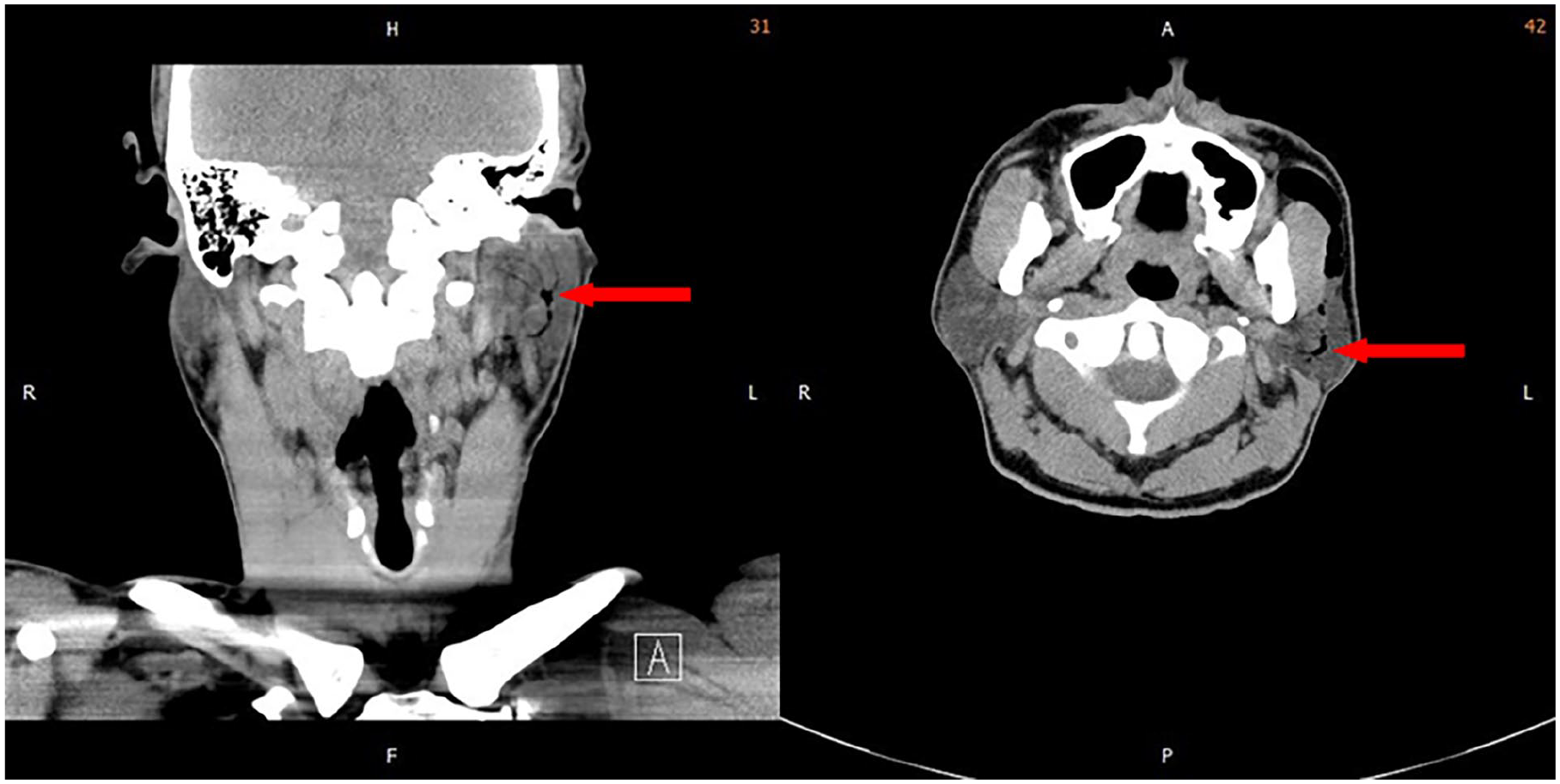
Coronal and axial sections of a CT scan of the neck, with red arrows highlighting air within the parotid gland ducts, are visible as hypodense areas in both views. CT, computed tomography.
Pneumoparotid is a rare condition characterized by the presence of air within the parotid gland and its ductal system, typically resulting from activities or behaviors that increase intraoral pressure, leading to retrograde airflow into the gland. This condition is often seen in occupational groups such as wind instrument players and glass blowers, individuals with habits like cheek puffing, and those undergoing certain medical procedures that elevate intraoral pressure. 1 Anatomical anomalies, such as a patulous Stensen’s duct, can also predispose individuals to pneumoparotid. The condition presents with symptoms like facial swelling, pain, and sometimes a crepitus sensation upon palpation. Diagnosing pneumoparotid involves clinical evaluation and imaging studies such as ultrasound 2 and CT scans, 3 which can visualize air within the gland and surrounding tissues. Over time, repeated episodes can lead to chronic sialadenitis, fibrosis, and in severe cases, emphysema in the mediastinum. In addition, if left untreated, the condition may cause persistent ductal damage and potentially necessitate surgical intervention. Treatment focuses on addressing the underlying cause, relieving symptoms, and preventing recurrence. Conservative management includes behavioral modification and occupational adjustments, while medical treatments involve anti-inflammatory medications and antibiotics if a secondary infection is suspected. Interventional procedures, such as ductal irrigation 4 and in rare cases, surgical interventions like duct ligation or parotidectomy 5 may be necessary for recurrent cases. Patient education plays a crucial role in the prevention and management of pneumoparotid. Individuals in high-risk occupations should be informed about the potential for this condition and advised on techniques to minimize intraoral pressure during their activities. For instance, wind instrument players might benefit from breathing techniques that reduce strain on the parotid glands. Regular check-ups and early intervention strategies, such as reducing playtime or modifying playing techniques, can prevent the condition from progressing to a chronic state.
While the current understanding of pneumoparotid’s etiology and management has advanced, several gaps in knowledge remain. Future research should focus on longitudinal studies that track the long-term outcomes of patients diagnosed with pneumoparotid, particularly those in high-risk occupations. In addition, the development of more effective preventive measures, such as specialized equipment or techniques to minimize intraoral pressure, may significantly reduce the incidence of this condition. Investigating the genetic predispositions or anatomical variations that may contribute to a higher susceptibility could also provide valuable insights into tailored prevention strategies.
Footnotes
Author Contributions
Conceptualization: P.-H.J. and S.-Y.C. Data curation: S.-Y.C. Project administration: P.-H.J. Supervision: T.-R.H. and S.-Y.C. Validation: T.-R.H. and S.-Y.C. Visualization: T.-R.H. Writing – original draft: P.-H.J. Writing – review & editing: T.-R.H.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
We confirm that written informed consent has been obtained from the patient for the publication of this case report. In addition, this study has received approval from the Institutional Review Board (IRB).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.