
Abstract

Significance Statement
Hamartoma is derived from a Greek word called Hamartia meaning defect or error. It is a benign malformation representing focal proliferation of normal cells. Hamartomas are common in the lungs, liver, and spleen but in regions of the head and neck, it is rarely seen. We here report a case of lipomatous hamartoma of buccal mucosa in a 4-year-old male child.
A 4-year-old boy presented to ENT out patient department (OPD) with a complaint of growth buccal mucosa from 4 years. According to the mother, it was progressively increasing in size with a child having difficulty in chewing due to the bulk of the lesion. Occasional history of bleeding from lesions due to trauma (Figure 1).
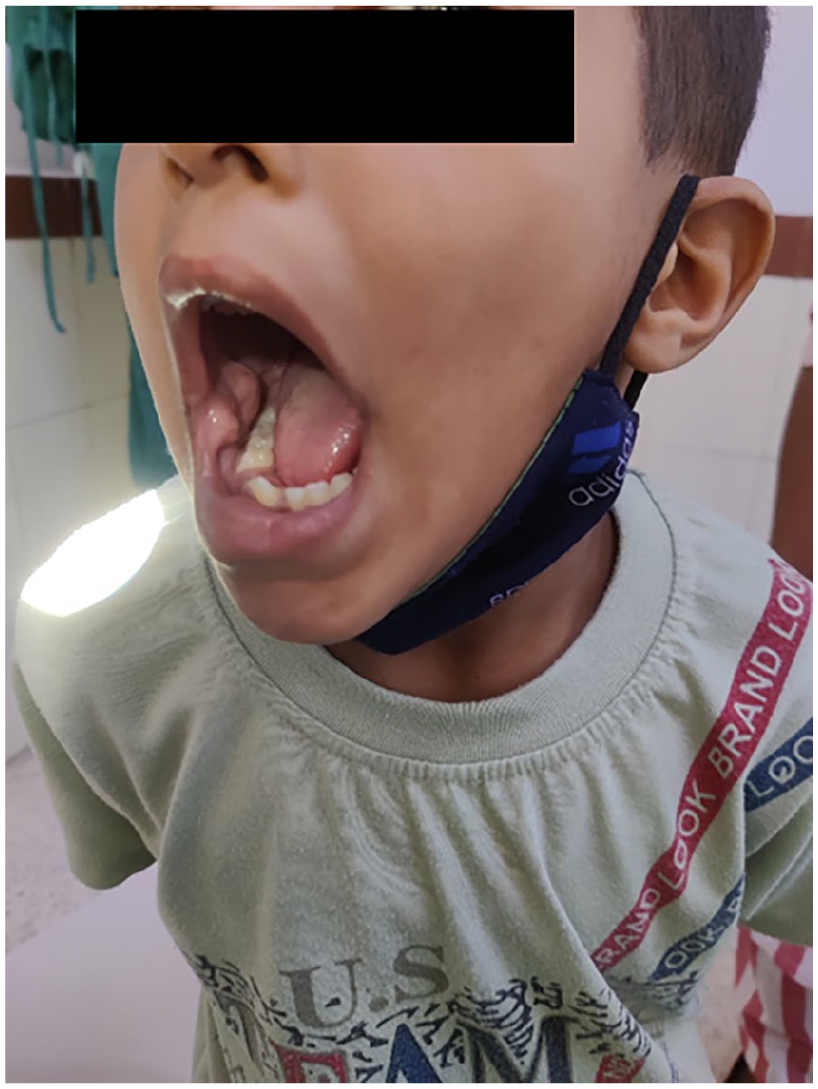
Pre-op picture of the mass right buccal mucosa.
On local examination, fullness was seen in the right cheek, and growth was seen in the right buccal mucosa which was exophytic, pinkish colored, 3 × 3 cm sized, irregular in shape with a smooth surface. On palpation, it was soft, non-tender, and did not bleed on touch. A dental opinion was taken for any misaligned tooth.
The child was advised fine-needle aspiration which was inconclusive and an ultrasound cheek which suggested a heterogeneous hyperechoic lesion of size 24 × 4 mm seen in the right oral cavity near the angle of mouth with minimal vascularity on color Doppler. The child was further advised contrast-enhanced MRI face which suggested a mild asymmetric non-enhancing soft tissue thickening of buccal mucosa on the right side with no areas of fat signals, T2 flow voids, or calcifications within likely benign lesion.
After the pre-anesthetic checkup, the patient’s attendant were informed about the surgical procedure, and the risks involved, and after informed consent, he was taken up for an excisional biopsy under general anesthesia because a diagnosis was not achieved. The lesion was excised in toto and suturing was done for the remaining defect using absorbable sutures. The child made a good recovery and no recurrence was seen in the 1-year follow-up period (Figure 2).

Showing postoperative images. (a) After 7 days. (b) After 1 year.
The sample was sent for histopathology which revealed a well-circumscribed unencapsulated lesion composed of lobules of mature adipocytes with interspersed skeletal muscles suggestive of lipomatous hamartoma (Figure 3).
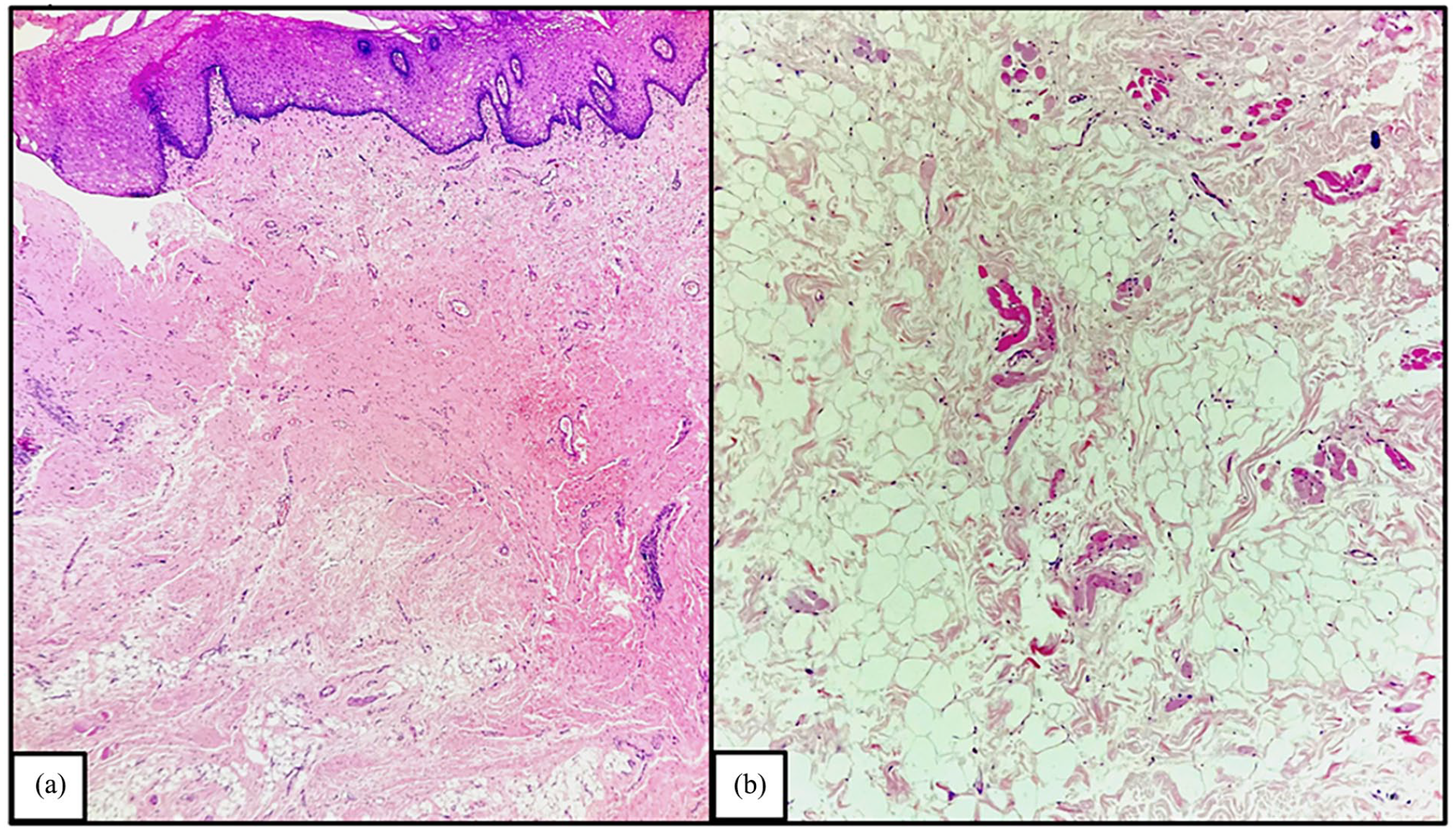
(a) The histopathological section shows a tissue bit lined by hyperplastic stratified squamous epithelium with underlying fibrous tissue and adipose tissue (H&E, 10×). (b) The high-power view shows abundant disorganized adipose, fibrous tissue, and a few scattered skeletal muscle bundles (H&E, 40×).
Hamartoma was described by German pathologist Eugen Albrecht in 1904. 1 Commonly seen in other parts of the body, but the incidence in the head and neck region is low. Within the oral cavity, they can be seen arising from odontogenic and non-odontogenic derivatives, muscles, nerves, bones, and fat.
The pathogenesis of hamartoma is unknown. Initially, it was thought to be developmental, but it is now considered to arise out of chromosomal aberrations. 2 It is also commonly seen in association with other conditions like tuberous sclerosis, Cowden syndrome, and Peutz-Jeghers syndrome. However, in our patient, no systemic features were seen. 3
Although the oral cavity is a common site for head and neck hamartomas, but very few cases of pediatric lipomatous hamartoma in the region of buccal mucosa have been reported. The clinical presentation in our case was not specific and after preliminary assessment, our differential diagnosis included choristoma, fibroma, pyogenic granuloma, hamartoma, lipoma, arterio-venous malformation, and malignancy.
However, granuloma and fibroma were ruled out based on clinical examination as granuloma is usually bluish in color and fibroma is firm on palpation. Imaging tools like CT and MRI were utilized to check for the nature and extent of swelling, but the final diagnosis was reached on histopathology. The lack of mitotic cells or nuclear atypia ruled out malignancy, lack of thick-walled vessels with phleboliths excluded arterio-venous malformations. 4 However, it is difficult to differentiate between lipoma, lipomatous hamartoma, and choristoma. Kaplan et al in a study concluded that both lipomas and lipomatous hamartoma are unencapsulated and well-circumscribed but lipoma contains only mature adipocytes, whereas hamartoma will have an admixture of adipocytes, skeletal muscles, and resident tissue. Between hamartoma and choristoma, histopathology is similar except for the fact that choristoma is composed of tissues not normally found at the anatomical site in which the lesion is arising. 5
Treatment of choice is complete surgical resection which was done in our case. Our patient has been under follow-up for the last 1 year and no recurrence has been reported. Due to the high recurrence rate of head and neck hamartomas, this case warranted the need for long-term follow-up.
We report a unique case of a lipomatous hamartoma in the buccal mucosa which presented as a slow-growing lesion. Although rare, hamartomas should be included in the differential diagnosis of buccal mucosa lesions.
Footnotes
Acknowledgements
None.
Authors Contribution
EN and ST prepared the manuscript and collection of materials. AK, NJ, and AG reviewed the manuscript before submission.
Data Availability Statement
The clinical data for this patient are available with the authors and can be reproduced on demand.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The clinical and surgical principles adopted for their management complied with the ethical standards of relevant national and institutional guidelines on human experimentation, as laid down in the Declaration of Helsinki, 1975, as revised in 2008.
Written Informed Consent
Written informed consent has been obtained from the patient’s legal guardian for the publication of this clinic document.