
Abstract

Significance Statement
A Bezold’s abscess is a suppurative collection in the deep tissues of the neck, occurring as an uncommon complication of acute otomastoiditis.1-3 It is non-palpable on physical examination, and diagnosis can be extremely challenging, leading to delays in treatment and possible life-threatening complications. 1 Imaging appearance on computed tomography (CT) and magnetic resonance imaging (MRI) modalities is essential in prompt diagnosis, preoperative planning, and treatment options.3-5
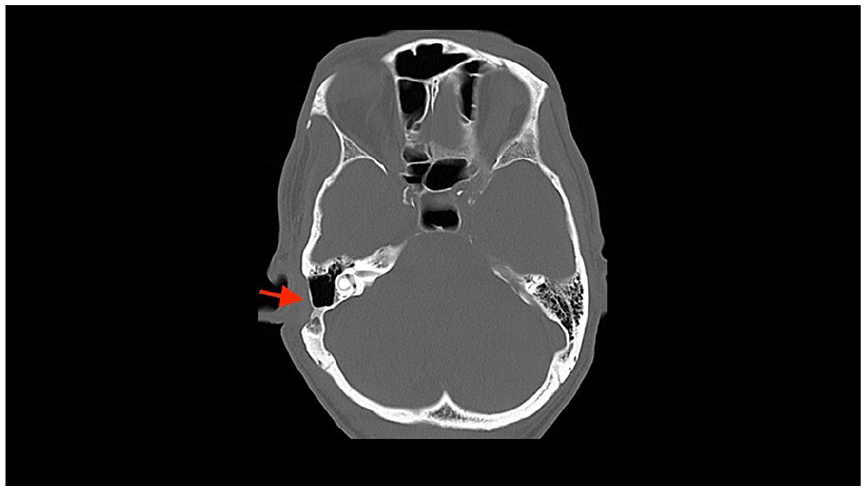
We present a case of a 68-year-old male with right otalgia, progressive hearing loss, and otorrhea for 6 weeks and acute onset of right facial paralysis 4-5 days prior to presenting to the emergency department. Physical exam was notable for right-sided facial droop, bulging right tympanic membrane, right postauricular tenderness to palpation, and mild edema. Laboratory evaluation was remarkable for ear swab cultures positive for elevated polymorphonuclear neutrophils without leukocytosis, gram-positive cocci, and gram-positive rods. CT temporal bone with contrast revealed opacification of the mastoid air cells, trabecular and cortical erosions of the right mastoid, and a cortical defect involving the inferior lateral mastoid (Figure 1). Additionally, there was a subjacent 1.4 × 0.4 cm subperiosteal rim enhancing collection with imaging findings compatible with coalescent mastoiditis and Bezold’s abscess. Contrast-enhanced MRI of the internal auditory canal confirmed findings visualized on CT and did not demonstrate any intracranial involvement (Figure 2). Management included antibiotics, incision and drainage of the abscess, and right myringotomy followed by mastoidectomy and debridement. During surgery, the intact facial nerve was decompressed and stimulated without response. A post-surgical CT showed changes of right mastoidectomy and no new areas of involvement (Figure 3).

Contrast-enhanced computed tomography of the temporal bone demonstrates trabecular and cortical erosions of the right mastoid (A) with an overlying rim-enhancing fluid collection (B) on coronal and axial reformats.
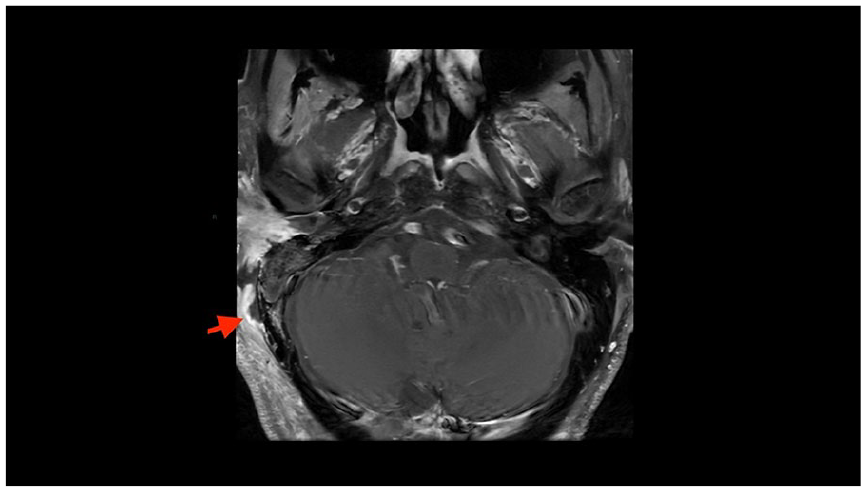
Axial contrast-enhanced magnetic resonance of the right temporal bone demonstrates a T1 hypointense rim enhancing collection adjacent to the right mastoid, compatible with abscess.
Contrast-enhanced computed tomography of the temporal bone demonstrates post-surgical changes status post right mastoidectomy and abscess drainage.
Otomastoiditis is a common complication of acute otitis media due to infection spreading to the mastoid from the middle ear. Resultant inflammation and hypertrophy of the mucosa in the aditus ad antrum can obstruct the suppurative process, leading to the development of coalescent mastoiditis. 2
First described in 1885 by Friedrich von Bezold; Bezold’s abscess occurs as a complication of coalescent otomastoiditis and erosion outside the cortex of the mastoid tip progressing into the sternocleidomastoid muscle and the attachment point of the posterior belly of the digastric muscle, extending into the infratemporal fossa.2,3 Clinically, this purulent collection remains challenging to palpate because it lies deep to the investing layer of the deep cervical fascia that cover the sternocleidomastoid and trapezius muscles.3,6 This infection can progress toward the carotid sheath, and thrombosis of the internal jugular vein can occur. 7 Other complications include intracranial involvement such as parenchymal abscess and cranial nerve involvement and extracranial involvement included retropharyngeal extension in rare cases. 7
Temporal bone CT and contrast-enhanced CT of the neck aid in diagnosis, identification of mastoid erosions, and assessment of the anatomical boundaries of the suppurative collection in the neck.3,5
MRI can provide additional anatomic details related to the suppurative collection and aid in assessing intracranial complications. CT or MR angiography are important in assessing for vessel involvement.3-5
Management of Bezold’s abscess requires a multidisciplinary approach and focus on source control, alleviating symptoms and preventing complications. Empiric broad-spectrum antibiotic initiation and prompt surgical management are required. Surgical management may include incision and drainage, mastoidectomy, and debridement of infected tissue.3,6
Footnotes
Author Contributions
J.D.G. and M.A. conceived the case topic and designed the paper methodology. M.A. conducted the data collection and performed the investigation and analysis. M.A., J.D.G., N.D.G., C.R., T.M.D., and E.P. interpreted the results and contributed to the manuscript writing. All authors reviewed and approved the final manuscript, ensuring accuracy and integrity in the reported findings.
Data Availability
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report.