
Abstract
We present a novel case of acute invasive fungal rhinosinusitis (AIFRS) following a maxillary molar root canal in a 69-year-old diabetic female, who subsequently developed unilateral vision loss. The patient reported a 1-week history of progressive left facial pain, trismus, and numbness following the procedure. Initial evaluation was unremarkable, but her condition rapidly deteriorated, culminating in complete vision loss in the left eye. Imaging studies revealed opacification of the left-sided sinuses and a rim-enhancing collection in the left pterygopalatine fossa. Surgical debridement confirmed mucormycosis. The therapeutic approach included systemic and retrobulbar amphotericin B administration, along with multiple sinonasal debridements. The patient’s poorly controlled diabetes mellitus significantly contributed to the rapid progression of the infection. Retrobulbar amphotericin B injections were effective in managing orbital involvement, thus avoiding the need for exenteration. Early diagnosis and aggressive treatment are paramount in improving outcomes for patients with AIFRS.
Introduction
Acute invasive fungal rhinosinusitis (AIFRS) is a rare, life-threatening condition characterized by the invasion of fungal organisms into the mucosa, submucosa, and osseous structures of the paranasal sinuses. This invasive process can extend to the orbit and intracranial compartments, resulting in significant morbidity and mortality.1-3 The leading causative pathogens of AIFRS are Mucormycosis and Aspergillus. 2 AIFRS predominantly affects immunocompromised individuals, including those with uncontrolled diabetes mellitus, hematologic malignancies, or those receiving immunosuppressive therapy.3-5
Diabetes mellitus is a well-established risk factor for the development of AIFRS, primarily due to the associated impaired immune responses. Hyperglycemia, a defining feature of diabetes, fosters an environment conducive to fungal proliferation and impairs the function of neutrophils, macrophages, and other components of the immune system. 6 Consequently, individuals with poorly controlled diabetes are particularly susceptible to AIFRS caused by fungal pathogens such as Aspergillus and Mucormycosis species.
The diagnosis of AIFRS can be delayed due to its nonspecific initial presentation, marked with headaches, facial pain, and swelling, which can mimic chronic rhinosinusitis and other conditions. Nasal symptoms are frequently absent, but AIFRS may be accompanied by ocular manifestations in the form of monocular or binocular visual impairment.7,8 This diagnostic delay can lead to poorer outcomes, as the disease may have already progressed to involve critical anatomical structures by the time it is identified. Thus, the prompt recognition and aggressive management of AIFRS, involving a combination of surgical debridement and systemic antifungal therapy, are crucial to preventing the progression.
Dental procedures, particularly through oroantral communication, have been associated with the development of maxillary sinus mycetoma/fungal ball 9 but the association between dental work and invasive fungal sinusitis is less clear. In this article, we report the first case of acute invasive fungal sinusitis after a maxillary molar root canal that presented as sudden unilateral blindness.
Case Presentation
The patient is a 69-year-old diabetic female who underwent a root canal with crown of tooth #15 as an outpatient procedure. Postoperatively, she was prescribed clindamycin, methylprednisolone, and nonsteroidal anti-inflammatory drugs for pain and inflammation management. Within a few days of the dental procedure, she began to experience progressive left facial pain, trismus, and numbness on the left side of her face, specifically in the V2 distribution. She initially thought these were related to the procedure and delayed seeking medical attention until a week had elapsed and she was evaluated by her primary care provider. No concerning findings were found on this evaluation and the patient was discharged.
Two weeks post-procedure, the patient experienced a decrease in vision in her left eye, accompanied by ptosis and near-complete ophthalmoplegia. The following day, this progressed to complete vision loss in the affected eye which she described as “curtain falling” over her vision. The patient presented to the emergency department at the request of a nearby urgent care with concerns for temporal arteritis given unilateral headaches and vision loss.
The patient’s initial labs were notable for a markedly elevated erythrocyte sedimentation rate of 130 mm/hour (normal <20 mm/hour) and C-reactive protein of 122.5 mg/L (normal <7.4 mg/L), indicative of a significant inflammatory response. Additionally, her HbA1c was significantly elevated at 13%, reflecting poorly controlled diabetes, which had been previously diet managed. Computed tomography (CT) and magnetic resonance imaging (MRI) studies were performed to elucidate the etiology of her symptoms.
Despite the patient having minimal to no sinus complaints, her CT was notable for opacification of the left-sided sinuses (Figure 1A). She was started on IV antibiotics and an MRI of the orbits was obtained that revealed a 1.7 × 2.1 × 2.8 cm rim-enhancing collection in the left pterygopalatine fossa and infratemporal fossa (Figure 1B and C). She underwent endoscopic sinus surgery (ESS) to treat the opacified sinuses and she was noted intraoperatively to have copious purulence in the nasal cavity, but overall healthy appearing mucosa aside from areas of necrosis immediately adjacent to the location of the sphenopalatine foramen and within the maxillary sinus (Figure 2). Biopsies were consistent with AIFRS secondary to mucormycosis and the patient was subsequently started on intravenous amphotericin and transferred for definitive management.
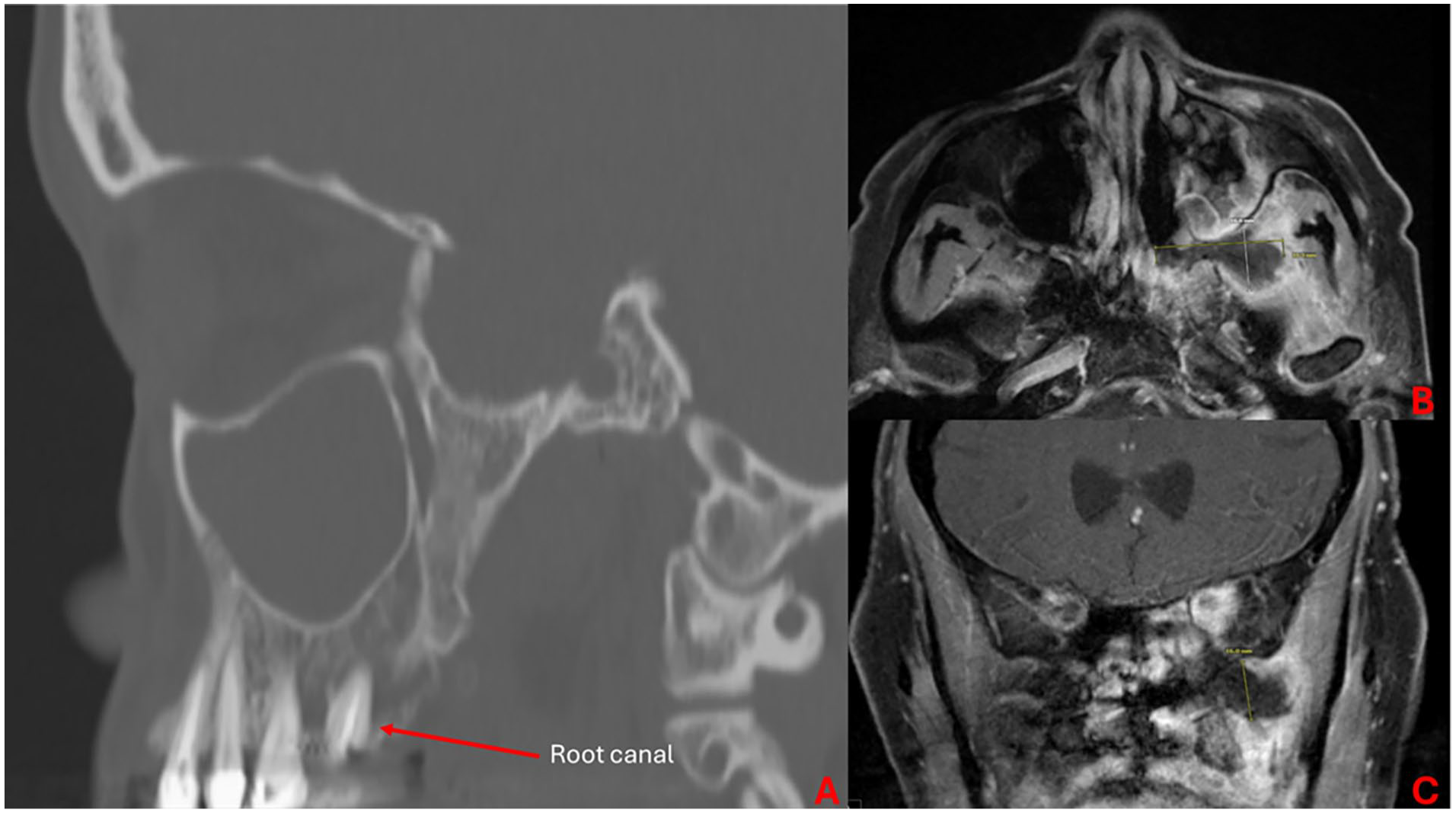
(A) Sagittal CT of the left maxillary sinus demonstrating complete sinus opacification and maxillary second molar that had recently undergone root canal. (B, C) Axial (B) and coronal (C) T1 post-contrast MRI demonstrating a 1.7 × 2.1 × 2.8 cm rim-enhancing collection in the left pterygopalatine fossa with extension into the infratemporal fossa. CT, computed tomography; MRI, magnetic resonance imaging.
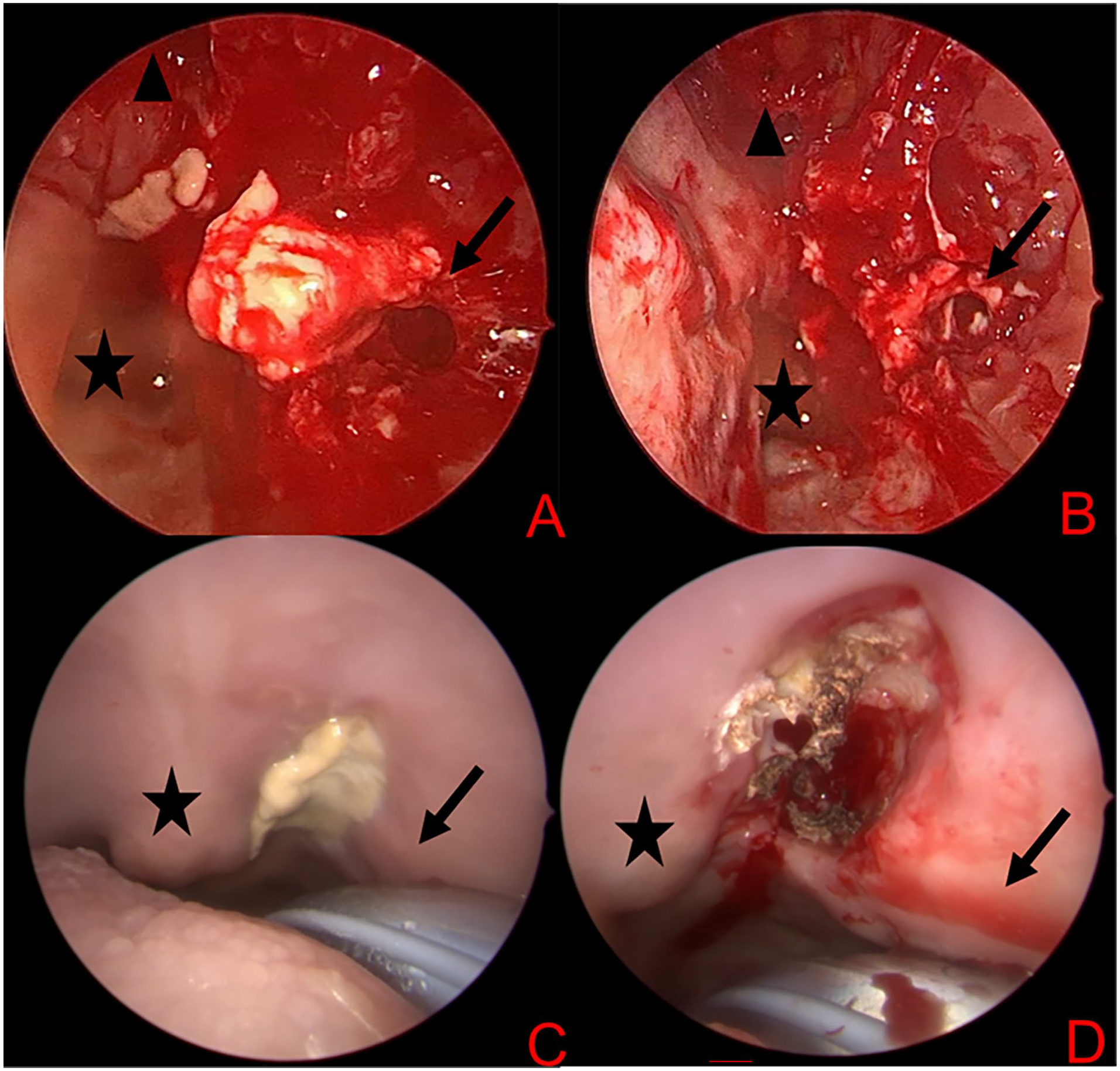
Intraoperative photos of first debridement. (A, B) Figure depicts a zero-degree endoscopic view of the nasal cavity during (A) and post-debridement (B) of necrotic tissue. The black star marks the nasopharynx, the black triangle denotes the left sphenoid os, and the black arrow denotes the pterygopalatine fossa. (C, D) Figure depicts a zero-degree endoscopic view of the oral cavity pre- (C) and post-debridement (D) of necrotic tissue at the location of the greater palatine foramen. The black star marks a tori palatini and the black arrow marks the approximate location of the alveolus of the second molar. All areas were positive for invasive fungal disease on final pathology.
On arrival, the patient underwent revision ESS for debridement of necrotic tissue, drainage of infratemporal abscess, and mapping biopsies to determine the extent of the disease. Biopsies were taken throughout the left paranasal sinuses to include the lamina, periorbita, and orbital fat. Interestingly, an examination of the oral cavity was notable for an additional area of necrosis at the location of the greater palatine foramen in the hard palate, near her operated tooth. Biopsies of the pterygopalatine fossa, infratemporal fossa, periorbita, orbital fat, and the oral hard palate were positive for invasive fungal elements. All other paranasal sinus and nasal cavity biopsies were negative for fungus with viable tissue throughout.
The patient was treated with a total of 7 injections of retrobulbar amphotericin B, systemic liposomal amphotericin B, and caspofungin, and an additional 2 operative sinonasal debridements. The patient was subsequently discharged on oral isavuconazole for long-term management and has been followed serially in the rhinology clinic since that time. At her last evaluation, 6 months post-discharge, she had only slight limitations to orbital abduction and had recovered light and shadow perception in her affected eye.
Discussion
We present the first documented case of AIFRS after a root canal in a poorly controlled diabetic patient. The patient presented with a complex clinical picture with the unusual presentation of rapid ophthalmoplegia and findings of an infratemporal abscess. The patient was successfully managed with a combination of systemic and orbital antifungal therapies with aggressive sinonasal debridement. Unfortunately, she had sustained loss of vision without anticipation of additional meaningful visual recovery.
Early management and treatment of AIFRS is the mainstay of treatment. This patient’s unique presentation likely contributed to her delayed presentation and treatment. Interestingly, she had a focal area of necrosis along the greater palatine foramen, which may be an extension of disease from the infratemporal fossa into the oral cavity and remains of uncertain significance. The patient also presented with a large infratemporal abscess, which further confounded her clinical picture as this was an atypical presentation.
Infratemporal abscesses are most commonly directly related to dental pathology. Young et al examined 67 patients across 43 studies and found that 44.8% of infratemporal abscesses were related to dental extractions with another 25.4% related to odontogenic infections. 10 In this review, there were no reported fungal pathogens in any of these infections with most demonstrating a polymicrobial bacterial etiology. In our patient, all bacterial cultures were negative, but at the time of her definitive drainage, she had been on intravenous antimicrobials for multiple days. A single case review from Prepageran et al documented an infiltrative aspergilloma of the infratemporal fossa but this was also without frank abscess and although the aspergilloma was infiltrative it was not causing an apparent AIFRS. 11
The other unique feature of this patient’s case is her close association with a root canal in the setting of poorly managed diabetes. Diabetes mellitus is a known immunocompromising condition that is a common contributing factor in the diagnosis of AIFRS and rapid reversal of immunocompromising state portends improved outcomes.12,13 Fortunately for this patient, her elevated inflammatory markers and hemoglobin A1C prompted additional consideration of infectious etiologies that may be contributing to her symptomatology and prompted her initial surgical evaluation that discovered her invasive fungal disease. This highlights the diagnostic challenges associated with AIFRS and the potential for delays in recognition and subsequent care.
To our knowledge, this is the first case of AIFRS associated with a root canal. Dental surgery is an extremely rare cause of invasive rhino-orbital fungal disease but has been documented in the literature, albeit only in case reports. Chopra et al noted 2 cases of AIFRS following dental manipulation for caries by reportedly unqualified personnel with unsterile instrumentation, which led to blindness, interestingly in immunocompetent patients. The exact nature of these procedures is not known and was presumed to be related to the treatment of caries/dental hygiene. 14 Additional case reports have shown similarly rare episodes of AIFRS in patients with multiple maxillary caries leading to odontogenic infection 15 and in 2 patients with dental extractions. 16 While rare, recent dental procedures, particularly in patients with severe immunocompromising processes should raise concern for the possibility of AIFRS in this patient population.
AIFRS management requires a multi-pronged approach combining surgical and pharmacologic treatments. In this case, the patient underwent ESS to debride the infected tissue, followed by systemic antifungal therapy with intravenous amphotericin B. In the case of AIFRS spreading from the pterygopalatine fossa to the orbit causing blindness and ophthalmoplegia treatment remains controversial. 8 Exenteration, being the most aggressive treatment modality, lacks data to support any survival benefit.13,17 A multicenter study by Dallalzadeh, et al. showed that transcutaneous retrobulbar amphotericin B injections significantly lowered the exenteration rate in patients with local orbital involvement without negatively affecting mortality. 18 In our case, we opted to employ retrobulbar amphotericin injections in lieu of orbital exenteration successfully.
Conclusion
AIFRS is a fulminant infectious process with high morbidity and mortality. The nonspecific presentation of AIFRS often delays diagnosis, highlighting the importance of imaging studies and a thorough medical history. This case further highlights the importance of heightened clinical vigilance when treating diabetic patients who present with nonspecific facial pain and ocular symptoms following dental procedures. Additionally, this case emphasizes the importance of recognizing atypical clinical presentations in these patient populations. Ultimately, prompt diagnosis and intervention employing a multidisciplinary approach are pivotal in managing AIFRS for the best possible outcome.
Footnotes
Submission Statement
This article is original and has not been submitted elsewhere in part or in whole.
Author Contribution
All authors reviewed the case, contributed to writing and editing the manuscript, and approved the final version of the manuscript.
Consent Statement
Written informed consent was obtained from the patient for the publication of this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.