
Abstract
Introduction
Laryngeal stenosis, a condition that narrows the laryngeal cavity, leads to breathing difficulties. Various surgical techniques, including laryngeal reconstruction, laryngoplasty, local injection, and carbon dioxide (CO2) laser surgeries, are available for treatment. CO2 laser incision has become popular due to its minimally invasive nature and high success rates. However, the restenosis rate remains a concern. 1 Our experience indicates that severe circumferential scars respond poorly to CO2 laser incision, resulting in a high rate of restenosis. Cricohyoidoepiglottopexy (CHEP) has shown promise for treating laryngeal stenosis, with a low restenosis rate and a high success rate in decannulation. 2 However, postoperative radiation therapy can complicate open surgery for some patients due to radiation-induced cellular and tissue damage, leading to inflammation, necrosis, and delayed wound healing. 3 Consequently, achieving sufficient exposure or mobilization of the larynx becomes challenging.
Case Report
A 71-year-old male presented to our department seeking surgical intervention for laryngeal stenosis and failed decannulation. Three years prior, he had undergone an anterolateral-vertical partial laryngectomy followed by 70 Gy fractionated radiotherapy for stage IV transglottic squamous cell carcinoma (T4N0M0). After 35 rounds of 70 Gy radiotherapy, he experienced shortness of breath when the tracheostomy tube was plugged. Laryngoscopy revealed significant circumferential laryngeal stenosis (Figure 1A and B), and computed tomography (CT) scans indicated marked narrowing of the laryngeal lumen without signs of tumor recurrence (Figure 1C and D). The initial surgical plan included scar resection followed by CHEP, after ruling out contraindications. However, during surgery, the surrounding tissue was found to be excessively stiff and adhesive, complicating the fixation of the cricoid cartilage to the hyoid bone and epiglottis.
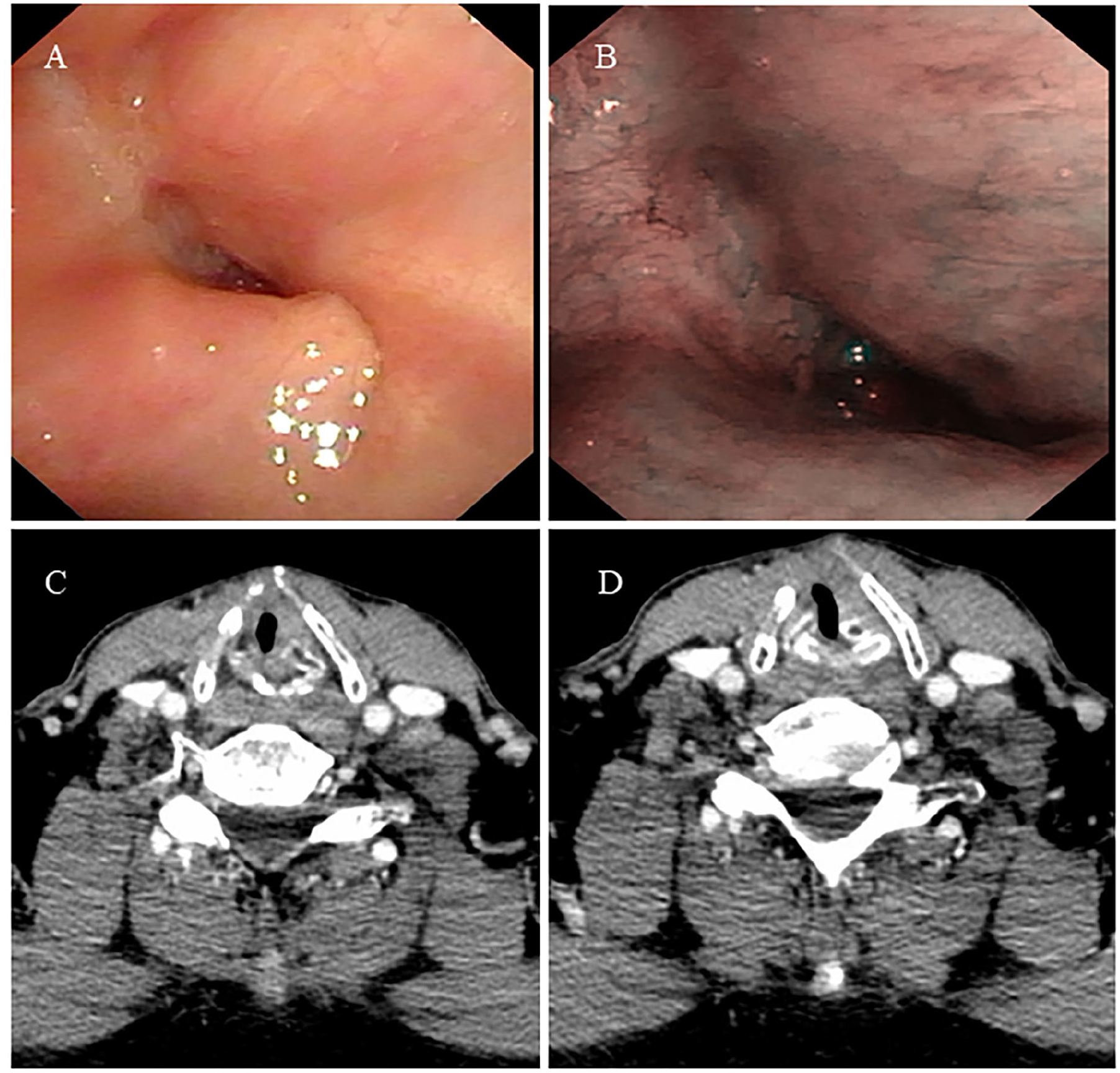
Preoperative laryngoscopy (A, B) and CT scan (C, D).
To avoid high-tension anastomoses and potential complications or discomfort, we conceived and performed an epiglottis-tongue root flap reconstruction. A 15 cm arc-shaped transverse neck incision was made along the cervical strip at the level of the tracheostomy, sparing the tracheostomy itself (Figure 2A). The linea alba cervicalis and part of the strap muscles were dissected to expose the larynx (Figure 2B).
Following exposure, the remaining lamina of the thyroid cartilage was mobilized and resected, and the scar tissue on the anterior portion of the laryngeal cavity was removed (Figure 2C). The epiglottis-tongue root flap was created by mobilizing the structure between the tongue root and the hyoid bone (Figure 2D and E). The inferior portion of the flap was anastomosed to the cricoid cartilage using 2-0 Vicryl sutures (Figure 2F and G). The strap muscles were then sutured together with 2-0 Vicryl to reinforce the reconstruction site (Figure 2H).
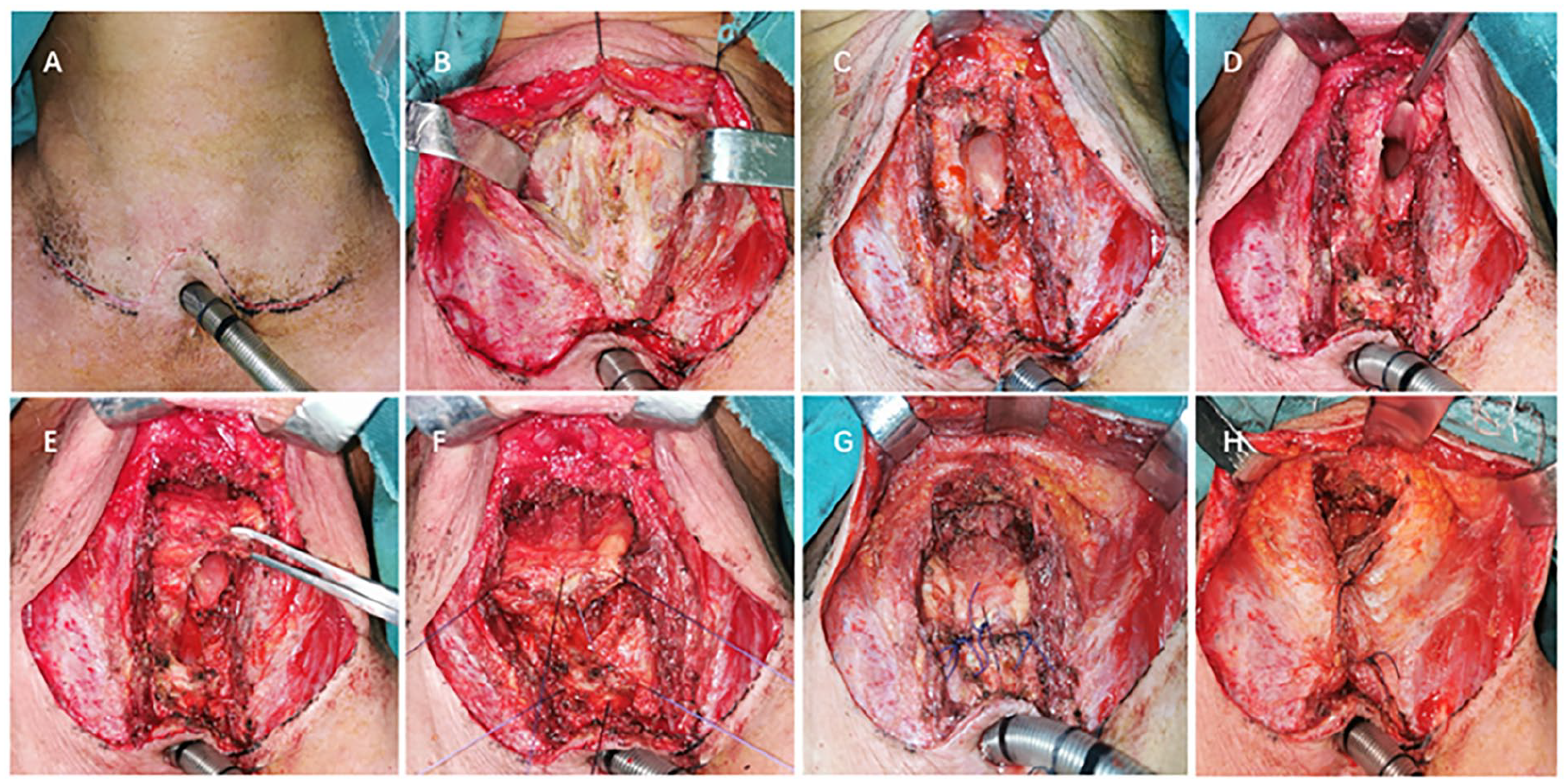
Surgical procedure of the modified CHEP surgery. CHEP, cricohyoidoepiglottopexy.
Antibiotics (cefoxitin sodium 2000 mg) were administered postoperatively until the third day, and enteral feeding via a nasogastric tube began on the first postoperative day. No complications related to the operation were observed, and the patient was discharged on the sixth postoperative day. The plastic tracheostomy tube was replaced with a metallic one on the discharge day, and the patient was encouraged to plug the orifice and practice speaking. Once the patient tolerated a liquid diet, the nasogastric tube was removed on the twenty-first postoperative day.
The patient’s recovery after the modified CHEP surgery was uneventful, with satisfactory swallowing function and minimal food aspiration. Follow-up laryngoscopies conducted at 1 month, 6 months, and 1 year postoperatively showed no structural stenosis (Figure 3). At the 1-month follow-up, laryngoscopy revealed moderate edema of the aryepiglottic fold but no structural stenosis. Unfortunately, the patient’s decannulation was significantly delayed due to intermittent COVID-19 lockdowns. Six months postsurgery, laryngoscopy demonstrated a patent larynx without any indications of stenosis. The decannulation was ultimately delayed for a year postsurgery due to quarantine policies. After decannulation, laryngoscopy showed no signs of stenosis, and the patient exhibited unobstructed breathing.
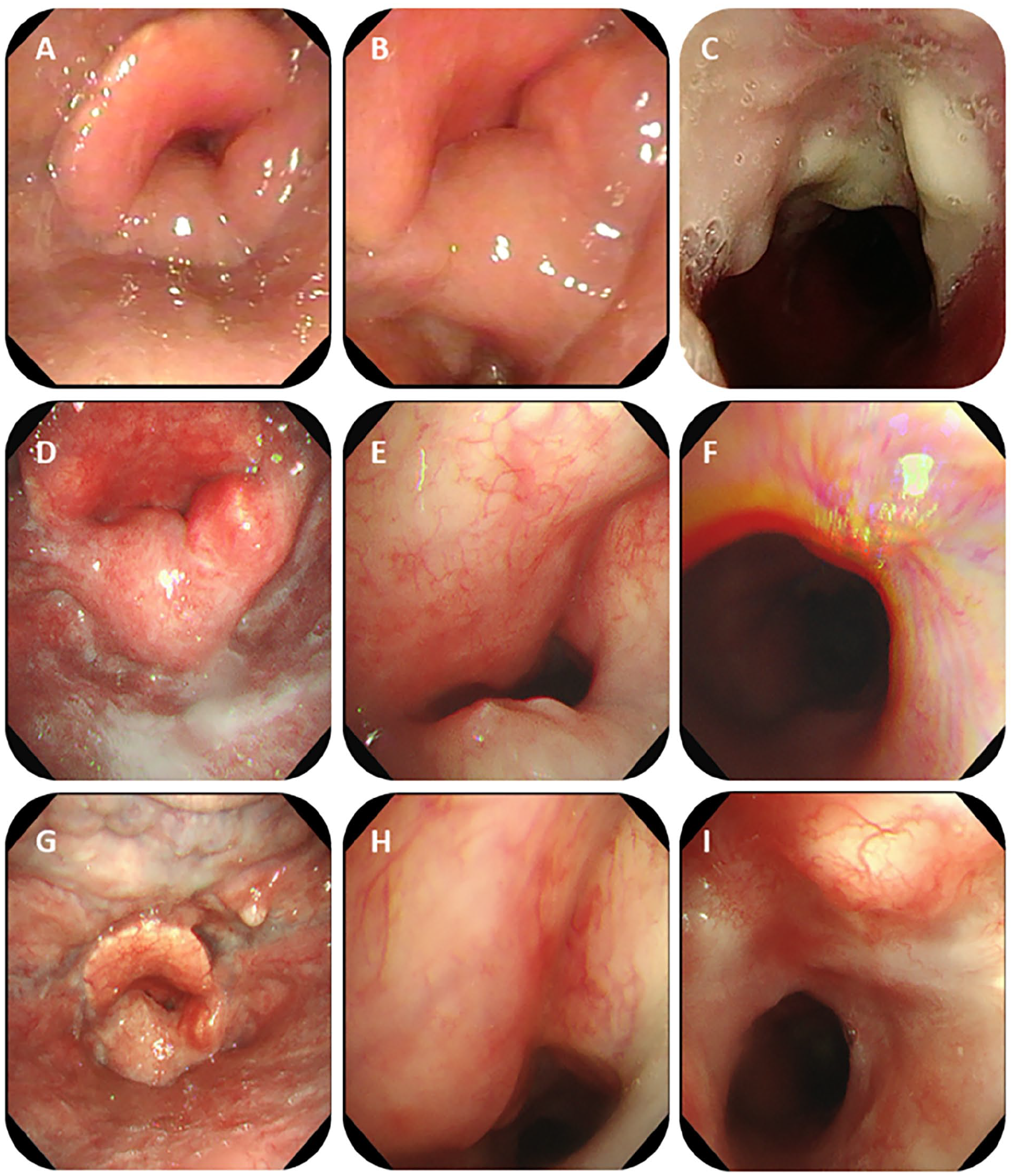
Postoperative laryngoscopy at 1-month (A-C), 6-month (D-F), 1-year follow-up (G-I).
Discussion
Among nontumor recurrence factors, radiation is a likely contributor to the development of postoperative laryngeal stenosis. 4 Radiation-induced fibrosis and surrounding tissue adhesion can present significant surgical challenges. 5 In the present case, significant adhesive cervical tissue contributed to the initial failure of CHEP surgery. However, after dissection of the preepiglottic space and mobilization of the tongue root, sufficient mobility was achieved to allow successful epiglottis-tongue root flap reconstruction, which was subsequently fixed to the cricoid cartilage.
During flap reconstruction, several considerations must be taken into account. Dissection and mobilization of the tongue root should be performed at the middle portion of the hyoid bone to avoid injuring the hypoglossal nerve, which could affect tongue movement. Additionally, it is crucial to protect the lingual artery to prevent bleeding and ensure the blood supply to the tongue root. Excessive mobilization of the tongue root-epiglottis flap should be avoided, and low-tension sutures with the cricoid cartilage are recommended to maintain the blood supply to the flap and prevent necrosis. Dissection at the junction between the tongue root and epiglottis should be done carefully to avoid separation of the tongue root from the epiglottis, which could compromise the blood supply to the epiglottis. It is also important to consider the patient’s overall condition, including cardio-pulmonary function and history of severe pneumonia, due to the risk of postoperative aspiration, which can be lethal in patients with poor general health. Patients who have undergone prior tongue surgery, particularly tongue root surgery, may not be suitable candidates for this procedure. Therefore, a comprehensive evaluation of the patient’s overall condition, degree of stenosis, tongue-to-tongue root status, and the adhesion of cervical tissue is necessary to determine the suitability of the procedure.
Conclusion
Modified CHEP can be a viable option for patients with postoperative laryngeal stenosis following radiotherapy. Comprehensive preoperative evaluation and the use of appropriate surgical techniques are crucial to achieving a favorable prognosis for these patients.
Footnotes
Acknowledgements
We are grateful to the nursing team of our Otolaryngology, Head and Neck surgery department for their data collection.
Data Availability Statement
The data of this study will be supplied upon proper request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study has been approved by the Institutional Review Board of the West China Hospital with a reference number of 2019-510.
Informed Consent Statement
Written informed consent for publication of this article was obtained from The Institutional Review Board of the West China Hospital as well as directly from the patient.