
Abstract

Significance Statement
Venous hemangioma of the inferior turbinate has rarely been reported, and differential diagnosis from benign lesions such as nasal polyp, inverted papilloma, capillary hemangioma, cavernous hemangioma, and juvenile nasopharyngeal angiofibroma is required. Therefore, clinicians should consider venous hemangioma when a lesion showing a white polypoid mass is observed in the inferior turbinate, and histopathological confirmation is needed through excisional biopsy.
Benign masses in the sinonasal region are commonly encountered by otolaryngologists. They occur most frequently in the following order: nasal polyp, inverted papilloma, hemangioma, and juvenile nasopharyngeal angiofibroma. 1 The inferior turbinate is an important structure when evaluating patients with sinonasal lesions because it can be easily observed with anterior rhinoscopy or nasal endoscopy. Outpatient biopsies can be performed under local anesthesia because they are easily accessible. Early lesions are often asymptomatic and may be discovered incidentally during routine examinations. Primary symptoms that appear as the lesion progresses include nasal obstruction, rhinorrhea, epistaxis, and sinusitis. 2 Our patient presented with symptoms of nasal congestion and rhinorrhea due to an inferior turbinate mass.
A 57-year-old man with left-sided nasal congestion and watery rhinorrhea was referred to our hospital. The patient had no relevant medical history or history of intranasal trauma. Nasal endoscopy revealed a smooth, whitish, polypoid mass originating from the left inferior turbinate (Figure 1A). Computed tomography confirmed a 2 cm-sized soft tissue dense mass originating from the left inferior turbinate and extending to the nasal floor (Figure 1B). An endoscopic excisional biopsy was planned under general anesthesia, and a complete excision of a mass measuring 2.2 × 1.5 × 0.5 cm was performed. The mass was sent to the pathology department for histopathological examination, and surgery was completed after hemostasis at the excision site. The histopathological examination revealed dilated vessel proliferation into the stroma (Figure 2A) and a thickened vessel wall with collagen deposition, confirming findings suitable for venous hemangioma (Figure 2B). The patient was discharged the day after surgery without complications. During the six-month follow-up, there was no recurrence at the surgical site, and the uncomfortable symptoms had resolved.
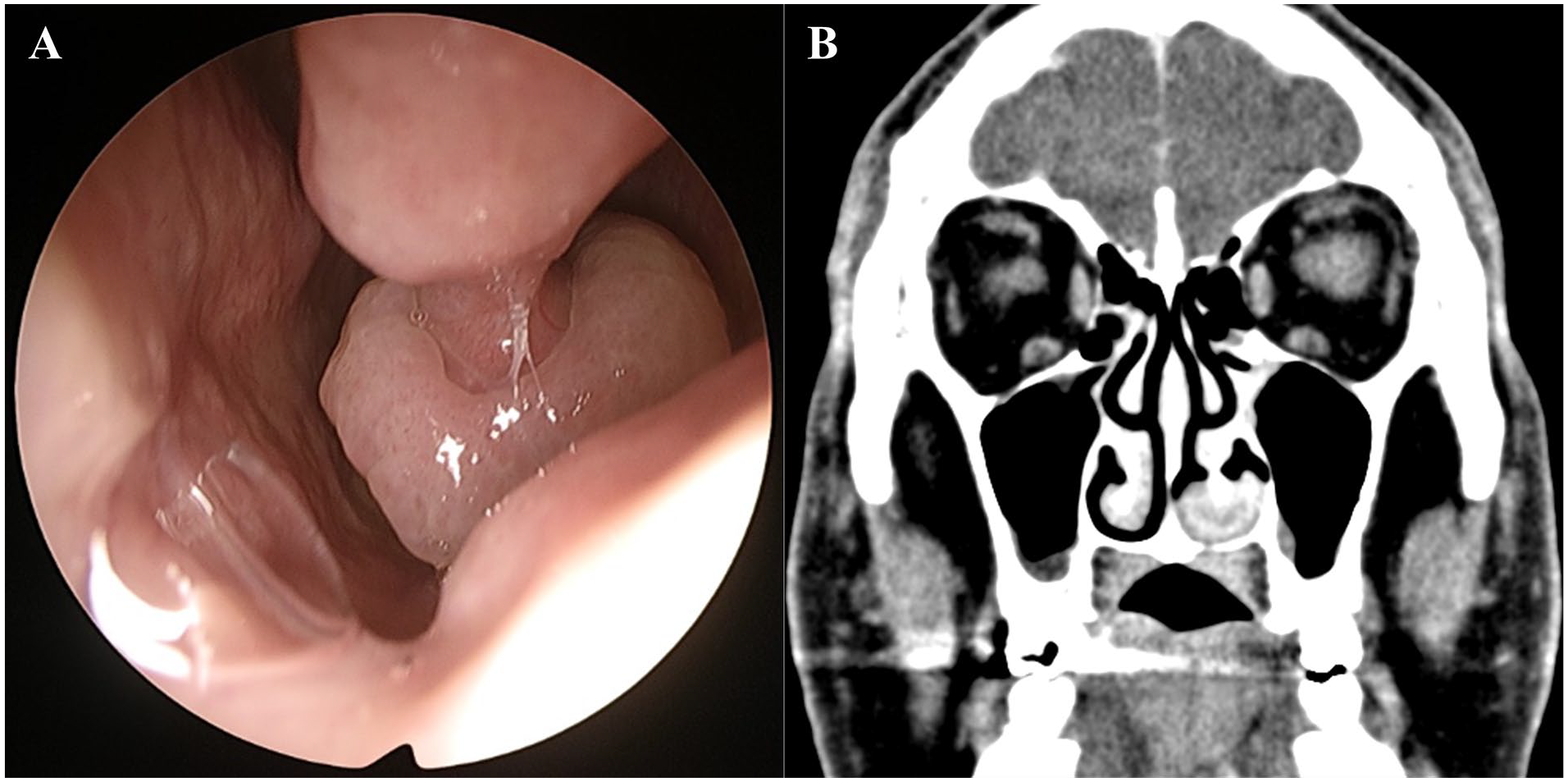
(A) Polypoid whitish mass on the inferior turbinate. (B) A coronal view of the computed tomography scan of the paranasal sinus showing a soft tissue density mass on the left inferior turbinate.
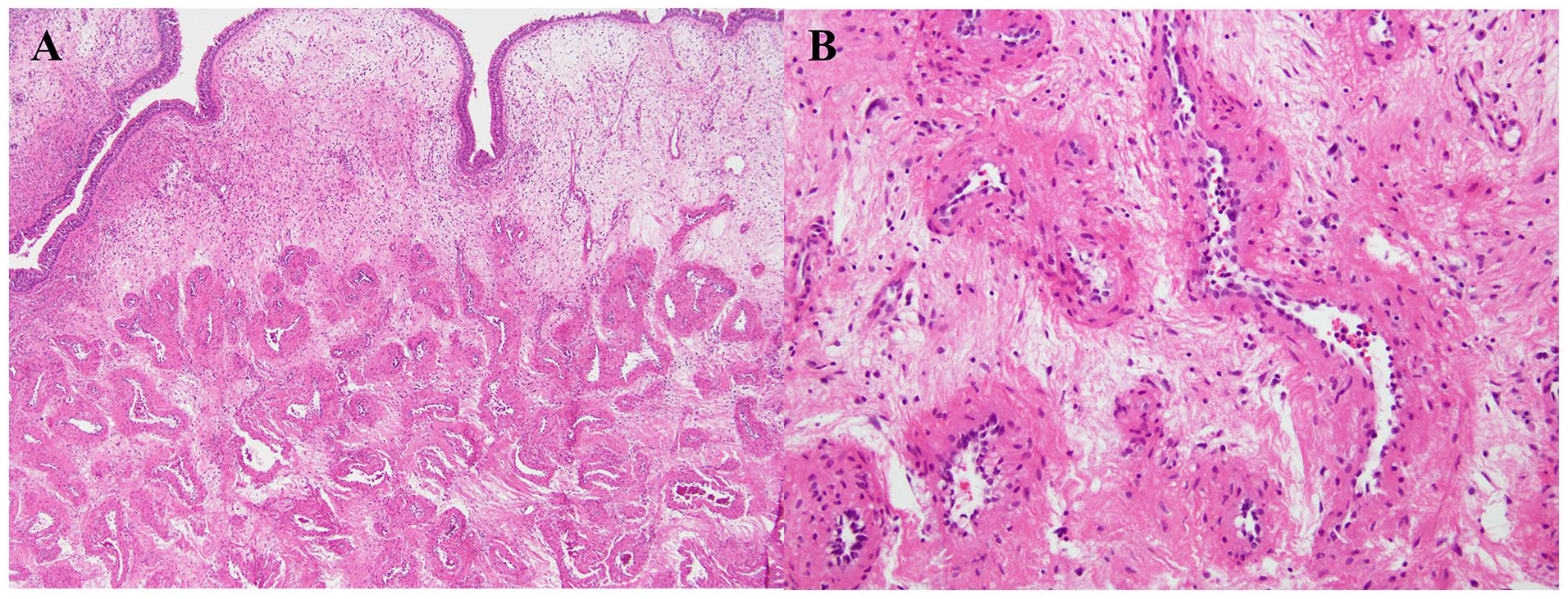
(A) Proliferation of dilated vessels in the stroma (40×, H&E). (B) Thick vessel wall with collagen deposition and the erythrocytes were shown in lumen of the vessel (100×, H&E).
Benign lesions in the inferior turbinate vary and can be classified as infectious, inflammatory, neoplastic, or vascular. Inflammatory polyps, which are mass lesions of the inferior turbinate, account for approximately 70% of all benign lesions. Inverted papillomas occur frequently (approximately 7%). Other reported lesions include osteomas, aneurysmal bone cysts, ectopic teeth, schwannomas, and fibrous tumors. 3 Various vascular lesions can also occur in the inferior turbinate, with angiofibroma, hemangioma, lobular capillary hemangioma, and angioleiomyoma being common.
Although the exact mechanism by which hemangioma occurs among vascular lesions is unknown, trauma, infection, hormonal influence, viral oncogene, underlying microscopic arteriovenous malformation, and the production of angiogenic growth factors are considered important in the pathogenesis. 4 Among traumatic factors, nasal packing following habitual picking is considered important, and the predominance of the origin of the lesion in the anterior segment highlights the relationship between the occurrence of hemangioma and trauma. 5
Depending on the vessel type, hemangiomas are classified into capillary, cavernous, and venous forms. 6 The lesion patterns vary depending on the evolution stage. In the early stages, they appear as cellular lesions with small vascular lumens and solid endothelial cell nests. In the established stage, various capillary-shaped, flat, and well-differentiated endothelial cells are observed. In the involuting stage, the lumen closes, capillary wall fibrosis and hyalinization increase, and the cavernous hemangioma consists of sinusoids or large, thin-walled vessels. 7
The treatment of venous hemangiomas involves complete surgical excision. Venous hemangiomas are usually large and do not tend to shrink, thus requiring surgery and pathological confirmation. 8 Therefore, venous hemangioma of the inferior turbinate in the nasal cavity requires complete endoscopic excision, including the origin and surrounding areas, and adequate hemostasis. 2
Venous hemangioma originating from the inferior turbinate is a rare benign lesion, with only one case previously reported. 2 Therefore, when differentiating tumors occurring in the inferior turbinate, clinicians should consider venous hemangioma as a differential diagnosis if it presents with similar features to those observed in our patient, despite its rarity.
Footnotes
Acknowledgements
The authors of this manuscript certify that they comply with the ethical guidelines for authorship and publishing.
Authors’ Note
We declare that this manuscript is original, has not been previously published, and is not currently being considered for publication elsewhere.
Author Contributions
J.L. and S.W.C designed the research; B.S.P. and S.W.C. analyzed the data; J.L. drafted the manuscript. B.S.P. and S.W.C. revised the manuscript. S.W.C. had the primary responsibility for the final content. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patient provided us written informed consent for the publication of this case report.