
Abstract
Significance Statement
Extraoral fistulas of odontogenic origin may be misdiagnosed and confused with furuncles, bacterial infections, foreign bodies, traumatic injuries, congenital fistulas, and carcinomas. Due to these complex diagnostic possibilities, treatments performed without determining the correct differential diagnosis are failure. Delay in diagnosis of these lesions may result in inappropriate and ineffective treatment. It is estimated that almost half of these patients are exposed to long-term antibiotic treatment and dermatological surgery due to misdiagnosis. 1
A 35-year-old male patient was admitted to our hospital with a complaint of skin discharge in the left neck region. The patient had a long-lasting toothache and swelling, redness and effluence in his left cheek. The patient’s vital parameters were within normal limits at admission. Laboratory tests revealed leukocytosis (16 × 109/L), elevated sediment C-reactive protein (85 mg/L). Magnetic resonance imaging (MRI) was performed. Axial T2-weighted images showed a hyperintense signal at the dental root level (Figure 1A). The axial post-contrast T1-weighted image showed a contrast enhancement around the dental root (Figure 1B). Coronal oblique T2-weighted images showed hyperintense fistula tract (Figure 2A). In coronal oblique and sagittal post-contrast T1-weighted images, the fistula tract showed a significant contrast enhancement (Figure 2B and C). Three-dimensional volume surface-rendering image (Figure 2D) showed the mouth of the fistula tract in the left submandibular space.
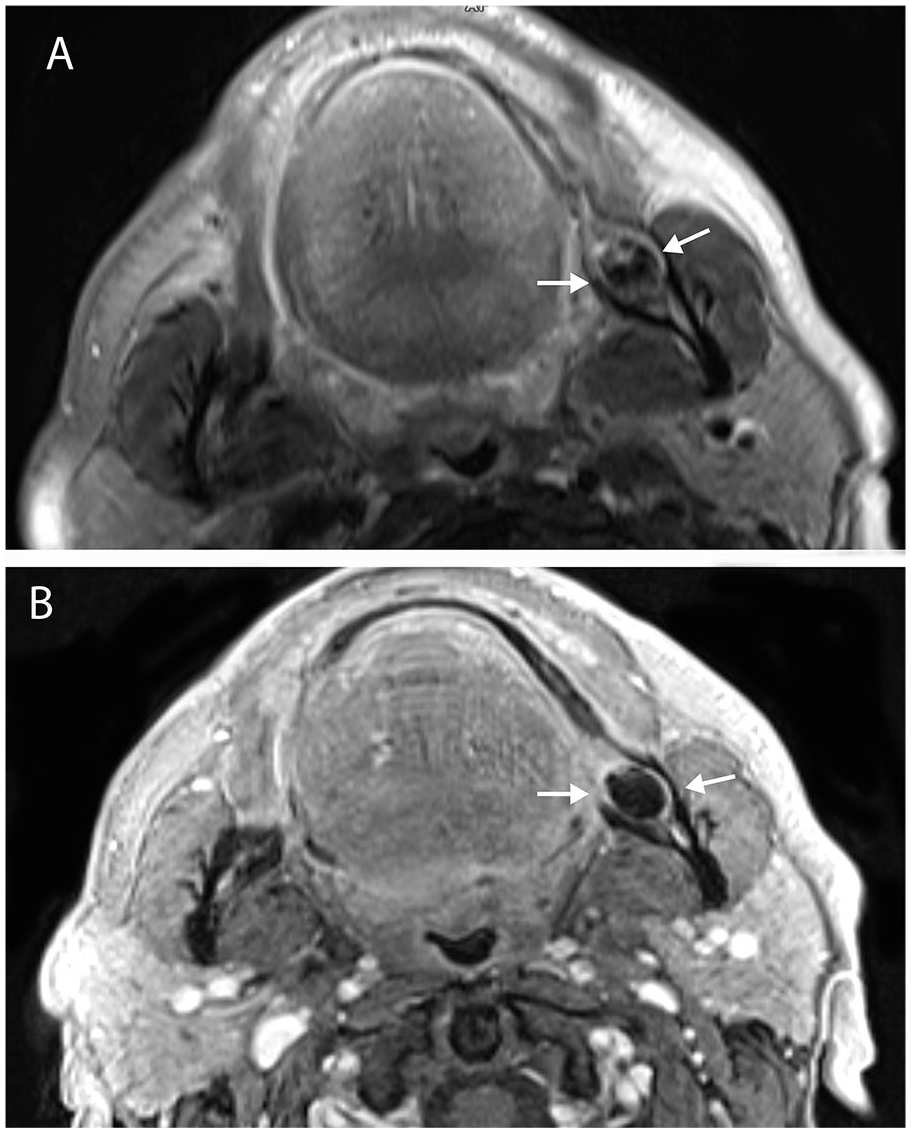
Axial T2-weighted (A) and axial post-contrast T1-weighted (B) images show inflammatory tissue with enhancement at the level of the dental root (arrows).
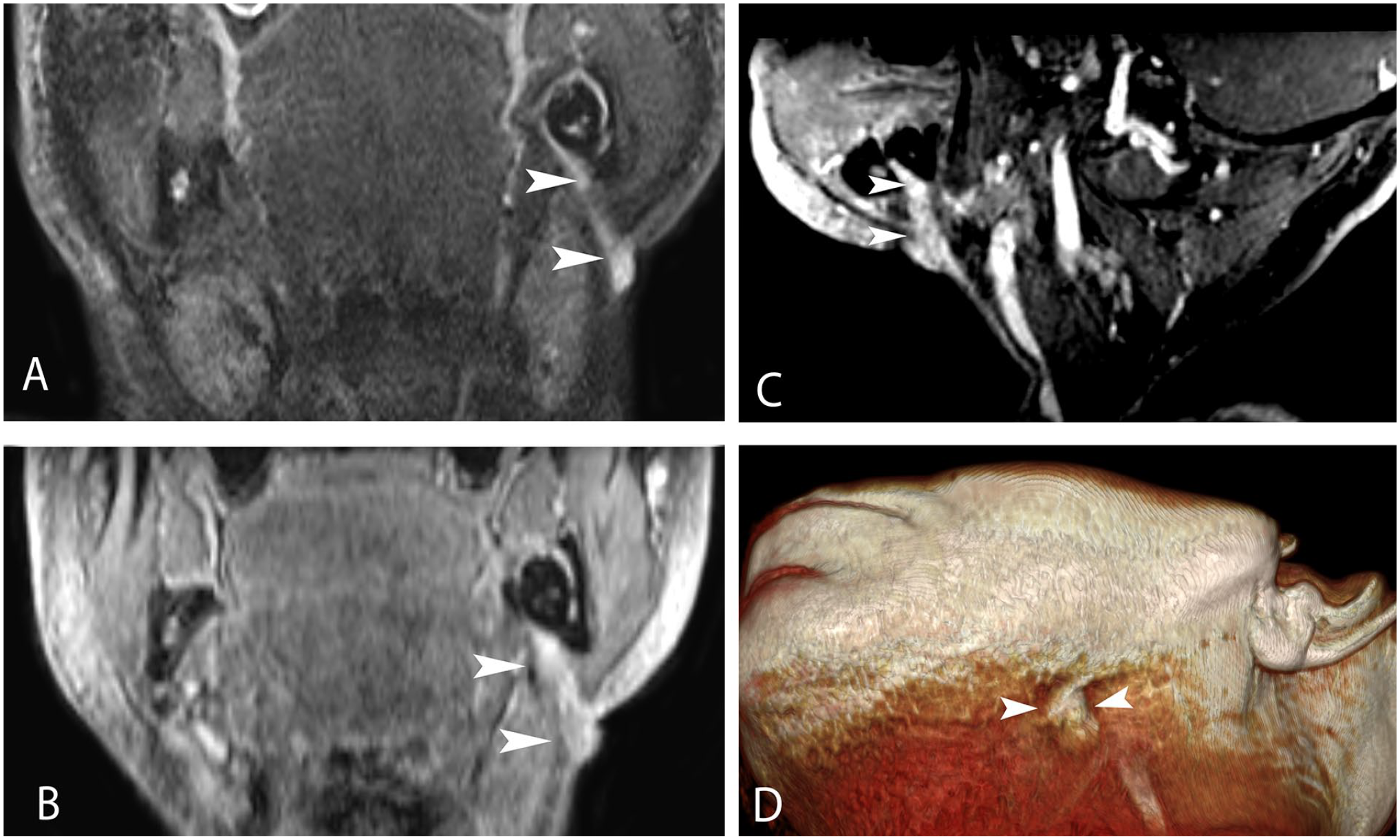
Coronal oblique T2 (A), coronal (B), and sagittal (C) oblique post-contrast T1-weighted images show the fistula tract to the skin from the dental root (arrowheads). The 3D volume rendering image (D) showed the cutaneous mouth of the fistula tract (arrowheads).
An odontogenic abscess is an acute infection of the dental tissue around the tooth root. Odontogenic infections are a common clinical problem in patients of all ages. The presence of inflammatory products resulting from dental caries, trauma, and/or periodontal disease can spread directly to the maxilla and mandible. Although odontogenic infections are generally limited to the alveolar ridge area, they can spread into deep fascial spaces and the skin. Dental abscess is a common manifestation and often requires urgent treatment. The most commonly affected areas are the chin and submental regions. 2 Patients can present clinically with or without fever, cervical lymphadenopathy, or localized pain, edema, and purulent discharge to the pathology area. The cutaneous fistula is often misdiagnosed as a dermatological infection when a drainage lesion is observed on the skin of the face; an endodontic origin should always be considered in the differential diagnosis. Dental abscess, congenital fistula, salivary gland fistula, infected cyst, and osteomyelitis should be included in the differential diagnosis of the skin-drained fistula tract. 3 Skin lesions such as foreign body lesions, pustules, furuncles, granulomatous disorders, squamous cell carcinoma, and basal cell face carcinomas are similar to fistulized dental diseases on the skin. 4 As the treatment approach for these entities is different, it is important to make an accurate diagnosis. At this point, imaging techniques are very important to show the path of the dental abscess and fistula. Multidetector computed tomography (CT) of neck soft tissues is considered the standard imaging modality for acute odontogenic infections. 5 Although MRI is considered time consuming and challenging for these patients, neck MRI has been shown to be feasible and have better diagnostic accuracy than previously reported for CT. A study has shown that MRI has high diagnostic accuracy for odontogenic abscesses, MRI findings can predict clinical severity and surgical approach, and MRI is highly successful in showing the path and source of the fistula. 5
Footnotes
Author Contributions
Mustafa Yeşilyurt and Gökhan Polat contributed to the design of the case and the creation of images. Mustafa Yeşilyurt wrote the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors declare that informed written consent was obtained from the patient for this case.