
Abstract

In the crowded slums of New York, diphtheria was an epidemic in the late 19th century—leading to death in nearly half of the infected children (2.23 deaths per 1000 in 1875). 1 Most of these children slowly suffocated as sloughed bacterial pseudomembranes clogged their airways. A few physicians resorted to tracheotomy, advocated by Trousseau in Paris for extreme cases. However, even when performed competently, death frequently followed. Into this world came a young physician, Joseph O’Dwyer, who devoted his life to battling this scourge.
Joseph O’Dwyer was born on October 12, 1841, in Cleveland, Ohio. He received his medical degree from the New York College of Physicians and Surgeons in 1866 and took his first job at the Charity Hospital of New York on Blackwell’s Island. In 1872, the focus of his work shifted to children as he was appointed physician to the Foundling Asylum of the Sisters of Charity in New York. Diphtheria raged through the city taking a terrible toll upon the orphans in his care. Tracheotomy saved none of them.
Joseph O’Dwyer began his intubation work in 1880. His initial idea was to deploy a wire spring within the larynx. He quickly realized the diphtheria pseudomembrane would form around the spring and continue to occlude the airway. Next, O’Dwyer developed a bivalve laryngeal speculum, which was composed of 2 portions of tubes cut longitudinally and fastened together so that the ends could be forced apart. 2 While more successful than the original wire spring, the inflamed mucous membrane could still force itself into a slit between the 2 portions of the speculum. Continuing his experimentation, O’Dwyer developed a tube that was longer than the speculum and had a collar at its upper end. It was with this device that he achieved his first successful treatment of diphtheria in 1884.
O’Dwyer continued to adjust his tube designs to improve retention and minimize aspiration. Using wax molds of cadaver larynges as models, he constructed tubes of various sizes each with a collar resting just above the vocal folds and a “retaining swell” in the middle part of the tube (Figures 1 and 2). 3 He tried tubes of brass, hard rubber, and gold plate to resist occlusion and crusting. He refined the tube inserter, an angulated instrument with a lever to release the tube once inserted. Despite these improvements, intubation of an awake, struggling child remained a technical challenge (Figure 3).
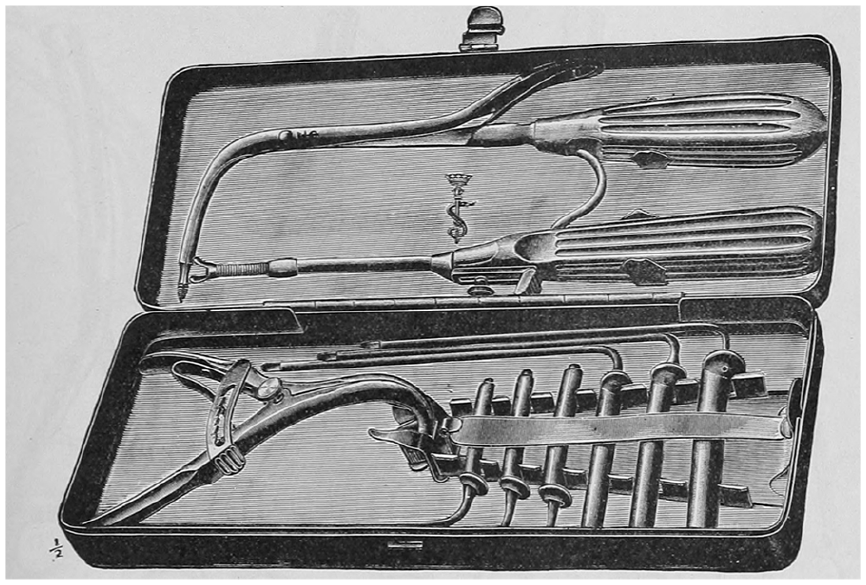
An O’Dwyer intubation set with angled tube inserter (top), mouth gag, and tubes of various sizes (from the 1915 Kny-Scheerer catalog). 4

O’Dwyer laryngeal tube with collar, central retaining swell, and removable obturator.
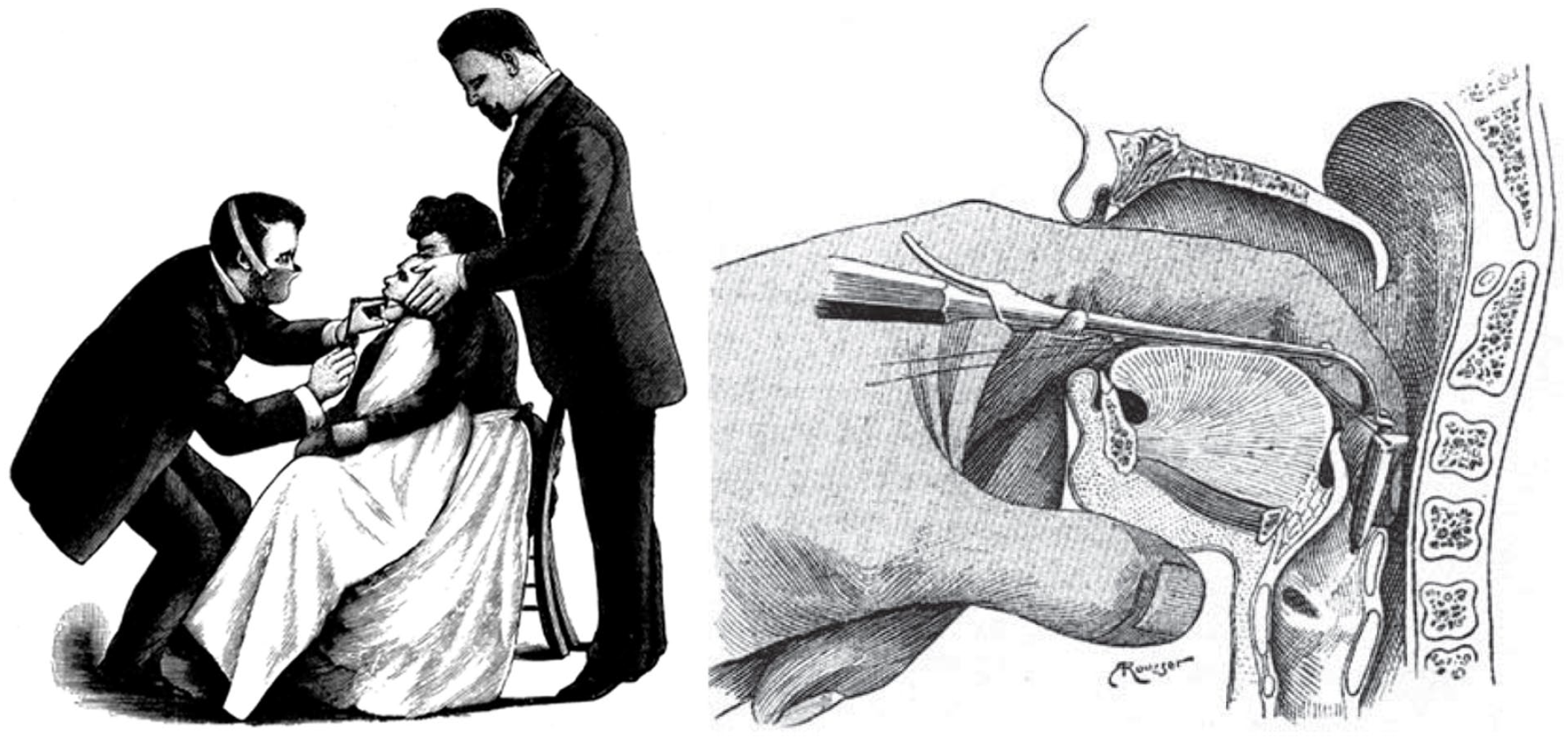
O’Dwyer intubation. Left—positioning and restraint. Right—anatomy of insertion (modified after Laurens G. Chirurgie de l’oreille, du nez, du pharynx et du larynx. Paris: Masson; 1924. pp. 852-881).
O’Dwyer intubation met with much initial resistance from physicians who still favored tracheotomy. 5 O’Dwyer wore down his opponents, presenting his favorable results at conferences and teaching his technique to others around the region. By 1889, the procedure was recognized as life-saving and O’Dwyer’s tubes were widely available from several instrument manufacturers.
While O’Dwyer intubation made a significant contribution to diphtheria care, advances in microbiology led to the conquest of the disease. The identification of Corynebacterium diphtheriae in 1884 by Friedrich Loeffler and Edwin Klebs and the subsequent development of antitoxin by Emil von Behring in 1891 6 produced the first effective medical treatment. Conversion of the diphtheria toxin to immunogenic toxoid with formaldehyde in 1921 allowed diphtheria vaccination and the gradual disappearance of the disease from the developed world. 3
O’Dwyer’s triumph over diphtheria did not save him from personal tragedy. He lost 2 of his 8 sons to diphtheria. After surviving both cholera and typhus in his early career, O’Dwyer lapsed into a coma and died at age 57 from a lateral sinus thrombosis secondary to a facial abscess after treating a patient with a similar infection. 7
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.