
Abstract
Laryngeal hemangiomas are rare vascular tumors, mainly in children, and less common in adults. Giant lesions typically require multiple endoscopic procedures and temporary tracheostomy. Open surgery allows single-procedure removal with fewer complications. CO2 laser excision controls bleeding and minimizes tissue damage. This study evaluates this hybrid approach to manage adult giant supraglottic hemangiomas. A 54-year-old woman with a giant supraglottic hemangioma was successfully treated using a combination of open surgery and CO2 laser. Limited data on adult laryngeal hemangiomas result in a lack of established treatment protocols. For giant supraglottic hemangiomas, combining open surgery with CO2 laser resection offers distinct advantages: enhanced lesion visibility, optimal airway control, effective hemostasis, reduced tissue damage, and lower recurrence rates. This hybrid approach also supports rapid recovery and favorable clinical outcomes. Combining open surgical excision with CO2 laser is effective for managing giant supraglottic hemangiomas in adults.
Introduction
Laryngeal hemangiomas are rare vascular tumors that predominantly present in children. 1 These benign congenital tumors are most frequently diagnosed in the head and neck region, with approximately 60% of cases occurring there. 1 In children, hemangiomas typically occur in the subglottic area, whereas in adults, they are more often located in the supraglottis. 2 In adults, these lesions are uncommon and often discovered incidentally during endoscopic procedures. 3
The clinical presentation of laryngeal hemangiomas varies significantly based on the size and location of the lesion. 4 Symptoms such as stridor, dyspnea, dysphonia, dysphagia, a foreign body sensation, and rarely, hemoptysis, reflect the severity of airway obstruction and involvement of surrounding laryngeal structures. 1 Imaging techniques, including computed tomography and magnetic resonance imaging (MRI), are essential for assessing the size, shape, and extent of hemangiomas. 5
Currently, there is limited data on adult laryngeal hemangiomas, leading to a lack of well-established treatmentprotocols. 6 Small lesions are often managed with regular monitoring, while larger symptomatic lesions typically require intervention. 7 Traditional management primarily involves minimally invasive endoscopic surgery using microscissors or laser. 7 However, these methods often necessitate repeated procedures and may require protective measures such as a temporary tracheostomy to secure the airway.8,9
Open surgery allows the complete excision of the hemangioma in a single procedure, with short-term intubation and precise resection with minimal postoperative complications. 8 Furthermore, CO2 laser excision offers precise removal with minimal bleeding, facilitating controlled tissue destruction and effective cauterization, making it particularly successful in treating supraglottic hemangiomas with minimal morbidity. 10 We present a case involving a 54-year-old woman successfully treated with a combination of open surgical resection and CO2 laser for a giant supraglottic hemangioma. It highlights the efficacy and advantages of this combined approach.
Case Report
We present the case of a 54-year-old female patient with controlled hypertension and gastroesophageal reflux disease, who has been experiencing chronic globus pharyngeus, dyspnea, and dysphagia for 7 years, with worsening symptoms over the past 2 years. She denies any history of substance abuse, smoking, allergies, or transfusions. Initially managed for sinusopathy on an outpatient basis by the Otolaryngology service, she was referred to Head and Neck Surgery due to persistent symptoms and lack of improvement.
Fibronasolaryngoscopy revealed a large, violaceous lesion originating from the hypopharynx, obstructing 2/3 of the posterior glottis and supraglottis, thus obscuring visualization of the vocal cords (Figure 1A and B). Subsequent MRI characterization of the lesion showed a lobulated mass measuring approximately 20 × 21 × 37 mm in the supraglottic and hypopharyngeal regions. The mass appeared hyperintense on T2-weighted images and exhibited patchy enhancement on post-contrast images. It extended posteriorly into the hypopharyngeal space and protruded into the piriform recesses, causing significant narrowing of the laryngeal vestibule and airway lumen, consistent with findings suggestive of supraglottic hemangioma (Figure 1C).
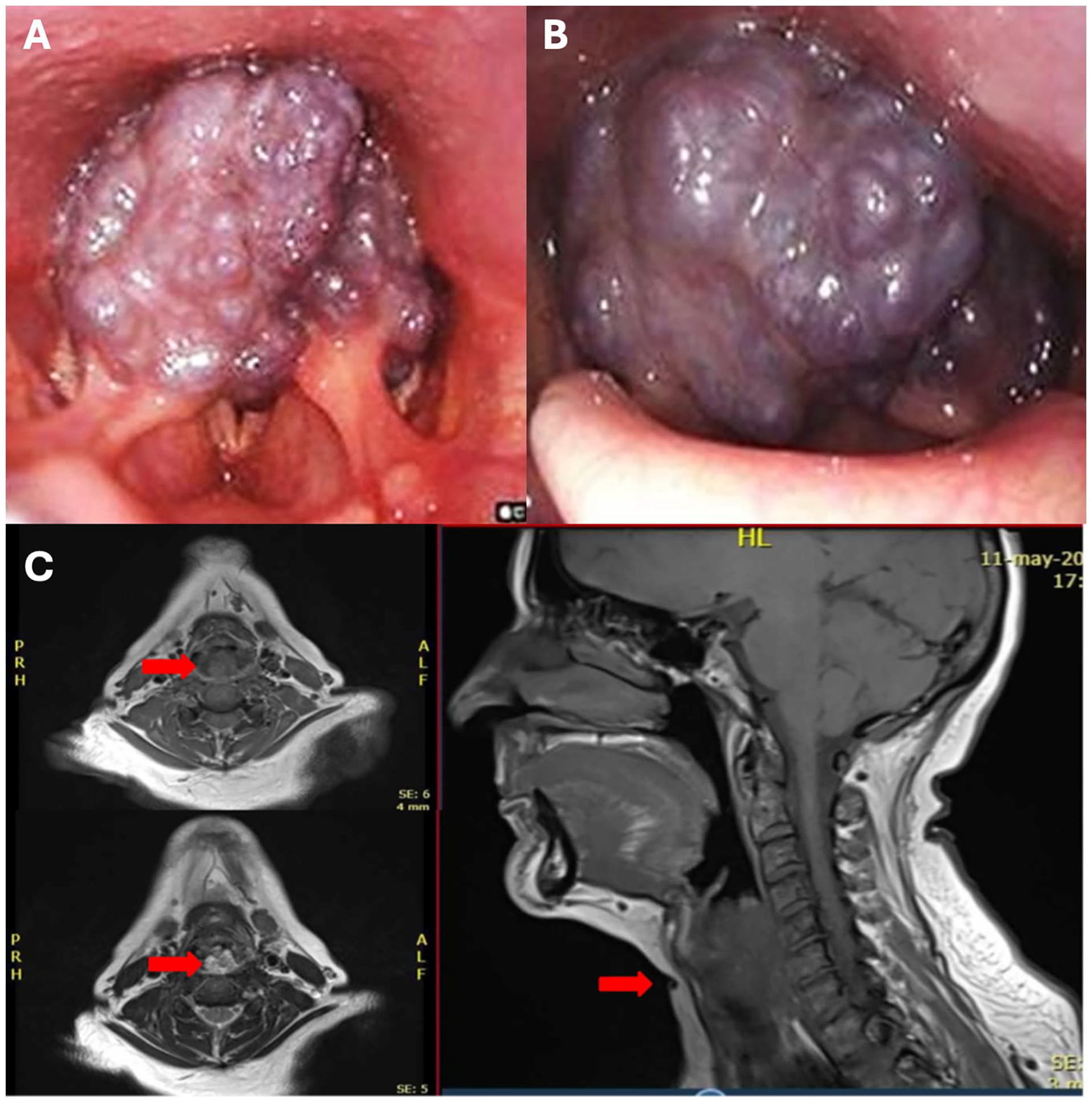
Supraglottic hemangioma. (A and B) Preoperative fibronasolaryngoscopy. (C) Magnetic resonance imaging. Red arrow: Lobulated mass, occupying the supraglottic and hypopharyngeal regions, apparently arising from the interarytenoid region.
Based on these imaging findings, we planned a surgical resection using a laryngofissure approach. The procedure involved a laryngofissure incision with laryngeal and tracheal sliding, representing a complex resection surgery. During the surgery, a vascularized mass compromising the supraglottis and obstructing both the glottis and hypopharynx was identified. This mass was successfully resected using a CO2 laser, resulting in minimal bleeding.
The procedure was uneventful, and the resected mass was sent for pathological examination. Postoperatively, the patient was transferred to the intensive care unit, intubated but in stable condition. She remained stable without complications or recurrence during follow-up. Extubation was successfully performed at 48 hours without any issues.
One month after the surgery, fibronasolaryngoscopy revealed mobile and symmetric vocal cords. The laryngopharyngeal region exhibited grade II/VI edema but remained patent, with minimal residual inflammatory tissue (Figure 2).
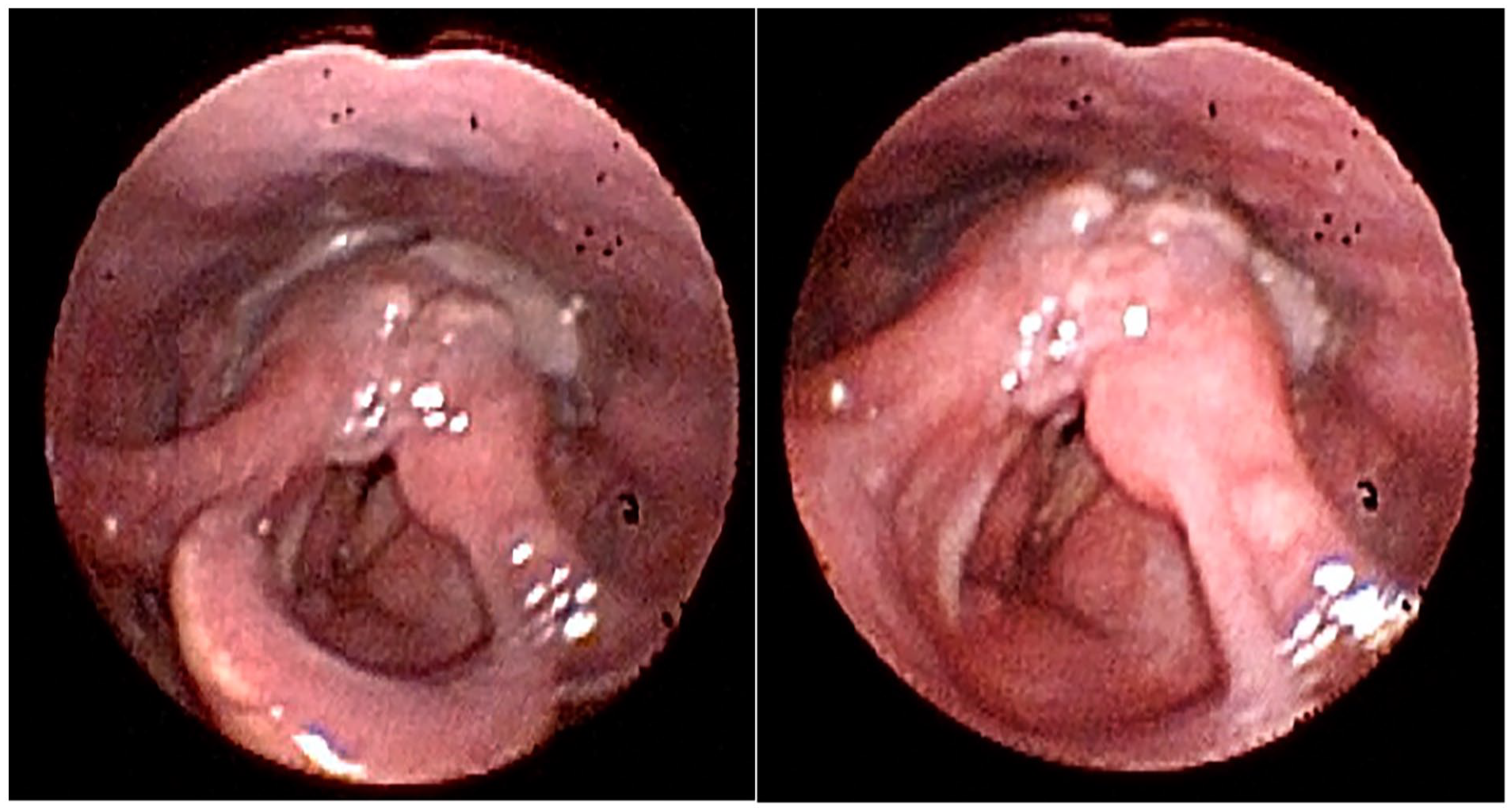
Postoperative fibronasolaryngoscopy.
Discussion
Adult-onset laryngeal hemangiomas typically occur in the supraglottic region and present with varying symptoms depending on their location. 1 In our case, the prominent symptoms included dysphonia, dysphagia, and a sensation of a foreign body. The etiology and predisposing factors of adult laryngeal hemangiomas remain poorly understood but are often speculated to include smoking, vocal abuse, intubation, and laryngeal trauma, 11 none of which were present in our patient.
Diagnostic evaluation usually begins with nasopharyngolaryngoscopy, revealing characteristic signs such as bluish discoloration or the Menzel phonation sign—marked by increased firmness, erection, and deeper coloration of the lesion during phonation. 12 Further imaging, including MRI, was necessary to fully characterize and delineate the extent of the lesion in our patient. The MRI findings were consistent with a hemangioma, showing homogeneous hyperintensity on T2-weighted images. 5
Treatment decisions are guided by factors such as age, location, size, and type of hemangioma. 13 While smaller lesions may be managed with observation or minimally invasive procedures, giant hemangiomas that compromise the airway, as in our patient’s case, typically require surgical intervention. 7 Open surgery provides the advantage of complete excision in a single-stage procedure with optimal airway control through short-term intubation and minimal morbility. 8
Moreover, the use of a CO2 laser during the resection provided superior control of bleeding and minimized trauma to adjacent tissues, thereby reducing the risk of postoperative synechiae or granulomas. 14 This approach also lowers the likelihood of recurrence, a benefit that has been documented in other case reports.15,16 Our combined approach allowed for the patient’s discharge on the 12th postoperative day without the need for a temporary tracheostomy. Although we are aware that the follow-up is short, at 1-month post-surgery the patient demonstrated favorable clinical recovery, with mobile and symmetric vocal cords and minimal residual inflammatory tissue.
Laryngeal hemangiomas, rare benign vascular tumors in adults, can lead to significant symptoms such as hemorrhage or airway-digestive tract stenosis. 4 Due to the lack of standardized treatment protocols, it is crucial to individualize the management plan based on the patient’s clinical presentation and the available therapeutic options. In our case, considering the lesion’s size, characteristics, and its impact on the airway, we opted for open surgical intervention with CO2 laser. This approach resulted in the complete removal of the hemangioma and favorable postoperative outcomes.
Conclusion
The combined approach of open surgical excision and CO2 laser offers a dual and effective strategy for managing giant supraglottic hemangiomas in adults. Open surgery ensures comprehensive lesion visibility for complete excision and optimal airway control through short-term intubation. CO2 laser excision enhances hemostatic control with minimal bleeding and reduces damage to adjacent tissues that could lead to postoperative complications. Both approaches facilitate rapid postoperative recovery and favorable clinical outcomes.
Footnotes
Consent to Participate
We declare that written informed consent for patient information and images to be published was provided by the patient.
Data Availability
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Institutional review board approval (IRB:2024.182) was obtained.