
Abstract
Keywords
Introduction
Head and neck cancer patients are known difficult airways among anesthesiologists and can pose as problematic intubation scenarios.1-3 The anatomical alterations resulting from tumors, coupled with the repercussions of prior treatments like radiation therapy, introduce complexities in intubation and ventilation during anesthesia. Consequently, patients with head and neck pathology are at an increased risk of facing challenging airways and major complications. 4 Standard of care practice instructs thorough evaluation and examination by the anesthesia care team to identify the potential for a difficult airway prior to intubation including when applicable, flexible fiberoptic laryngoscopy examinations (FFL).5,6
FFL is routinely performed in head and neck oncology clinics to assess and clinically stage tumors of the oropharynx, larynx, and hypopharynx and provides a crucial and dynamic assessment of patients’ airways. Despite being a well-established examination within otolaryngology, FFL is not commonly incorporated into the preoperative airway assessment algorithm by anesthesiologists at our institution and others. 7 Several studies within the anesthesiology literature have proposed multivariable indices to predict a difficult airway during the preoperative airway assessment. Most of these indices include factors such as mouth opening, thyromental distance, Mallampati grade, neck movement, and others without including assessment of the larynx itself.8-11
The integration of FFL into the preoperative assessment could provide anesthesiologists with valuable information about the airway’s condition, potentially leading to better preparation and a more tailored intubation plan. This could minimize the risk of encountering unforeseen difficulties during intubation, reduce the need for emergency surgical airway access, and enhance overall patient safety.1,12 To our knowledge, this is the first study to analyze the subjective and objective utility of FFL, as performed by otolaryngologists, in forming the intubation plans of anesthesiologists for patients with head and neck cancer. It seeks to determine whether incorporating FFL into the preoperative airway assessment algorithm can improve the prediction of difficult airways and reduce the incidence of complications during intubation. This could potentially lead to a new paradigm in airway management for this high-risk patient population.
Methods
Participants
All research was conducted at a single tertiary care hospital after obtaining exemption by the University of Arkansas for Medical Sciences Institutional Review Board (IRB: 273909). Patients with primary or recurrent clinical stage T2 and greater squamous cell carcinoma cancers of the oropharynx, hypopharynx, or larynx who underwent orotracheal or nasotracheal intubation by the anesthesia department at a single tertiary referral center were included in the study. Patients who presented through the emergency department (ED) or the head and neck oncology clinic between May 2022 and April 2023 were included. Patients who underwent intubation within the last 12 months at our institution were excluded due to concerns of potential bias related to thorough documentation of the previous intubation method and its details in the electronic medical record. The patients who were planned to undergo awake tracheotomy by the otolaryngology provider were excluded from the study. Those with an established tracheostomy were also excluded. Patient records were excluded if pathology was negative for squamous cell carcinoma or if the collected objective data were incomplete. All data were collected by the first author (A.C.G). Data extracted for each patient included: demographic data, date of FFL, date of surgery, surgery performed, clinical stage and, if applicable, pathological stage of the cancer, location and laterality of the tumor, and recurrence status. 13
Data Collection
The FFL was performed by either the otolaryngology resident, fellow, or attending fielding the consult or referral. The FFL video was recorded on the portable FFL consult tower if seen through the ED or on one of the clinic towers. Video recordings from the portable FFL consult tower are stored on the device itself and can be uploaded and viewed. The video recording was shared with the anesthesia care team day-of-surgery via an encrypted email. If the patient was seen through the clinic, the FFL videos were stored through an encrypted database only accessible through the hospital computer system. These videos were collected by the first author (A.C.G) and emailed to the anesthesia care team day-of-surgery. All FFL recordings were shared with the anesthesia care team after their pre-FFL intubation plan was established. The anesthesia care team’s standard preoperative evaluation at our institution includes both a chart review of notes and imaging and physical exam of the following categories: anesthesia history/precautions, cardiovascular, pulmonary, neurology/psychiatric, gastroenterology/hepatic/renal, endocrine, and any other extraneous categories. After the anesthesia care team completed their standard preoperative evaluation, the FFL was shared with them. No patient underwent unnecessary preoperative FFL as these examinations are routinely performed when evaluating a patient with an upper aerodigestive tract tumor at our institution.
Main Outcome Measures
Preoperative and postoperative surveys completed by the anesthesia care team for each eligible patient were collected. The surveys were filled out by the attending anesthesiologist and either the certified registered nurse anesthetist or the anesthesia resident physician assigned to the case. These assignments are made one day prior to the case. The preoperative survey included the anesthesia care team’s intubation plan, before and after reviewing the recorded FFL. The preintubation section collected information on the anesthesia team’s pertinent patient’s history/exam, their interpretation of the level of obstruction from reading the FFL findings in clinic notes, and whether they could view any diagnostic imaging of the airway. Data pertaining to their intubation plan included plan/method for intubation, sedation plan, and patient state of respiration. Data on specific laryngoscope, endotracheal tube size, and use of paralysis were also collected (Figure 1). The team that filled out the survey proceeded with their planned intubation after reviewing the FFL. If the anesthesia team changed day-of-surgery, a new form was filled out by the attending anesthesiologist and either the certified registered nurse anesthetist and/or the anesthesia resident physician performing the intubation. Postoperative data were collected on the details of the intubation performed and complications. Information was collected for cases where the intubation performed did not correlate with the planned intubation. These scenarios are discussed further in the discussion. Subjective satisfaction postoperative surveys were obtained to assess the subjective utility of FFL in creating anesthesia’s intubation plan. The postoperative subjective feedback surveys were always filled out by the attending anesthesiologist. Chi-square analysis was used for the comparison of categorical variables, with use of Fisher’s exact test in cases of low numbers.
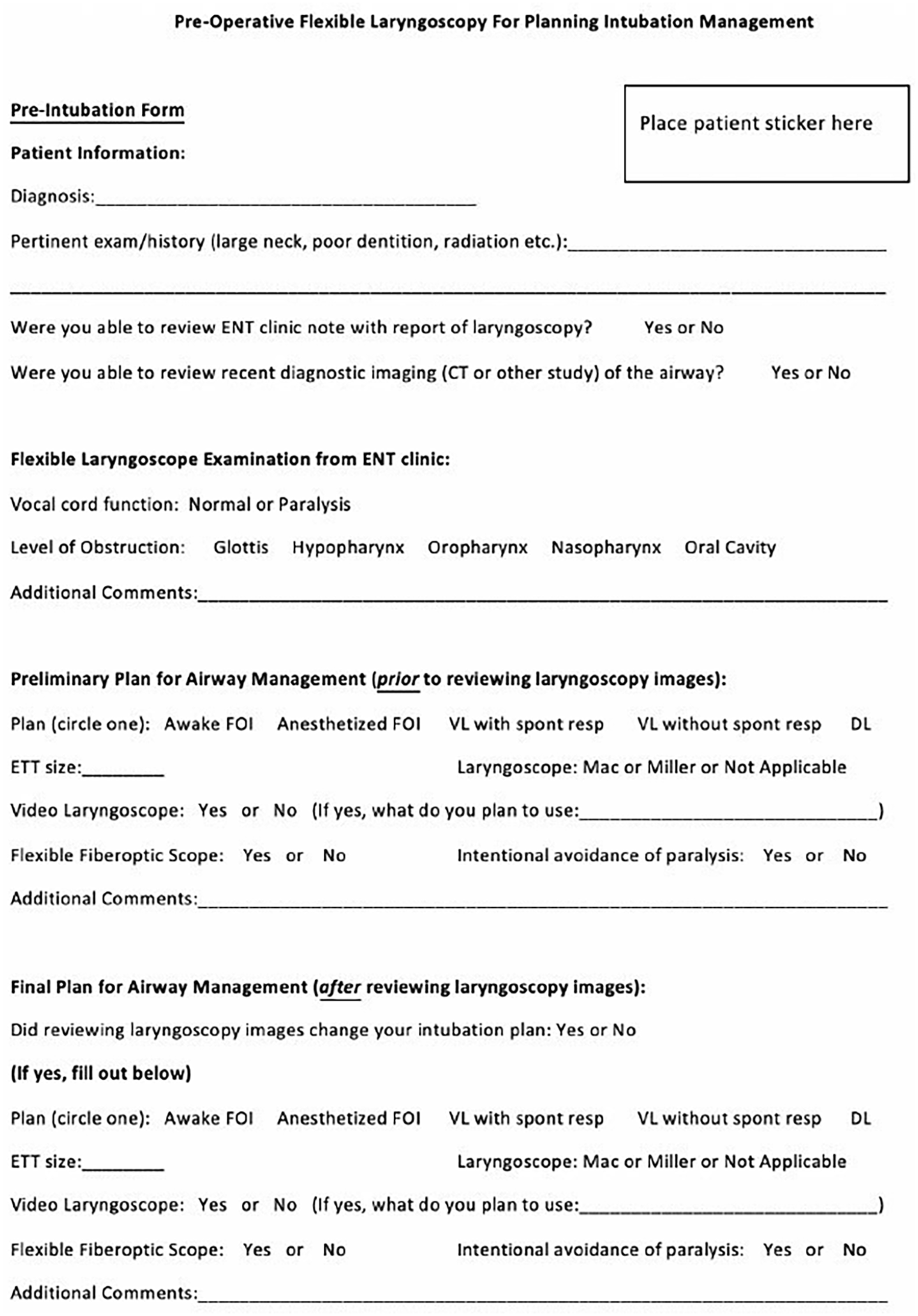
Anesthesia’s preoperative intubation survey.
Results
After the preoperative exclusion criteria noted above, 44 consecutive patient cases were deemed eligible. Ten of the cases were excluded, 8 due to pathology not resulting in carcinoma and 2 due to surveys being filled out incorrectly. Thirty-four patient cases were, therefore, included in the final analysis. The 34 patients (49-87 years of age) were majority male (79%, n = 27). The tumors were primarily oropharyngeal in location (50%, n = 17) and clinical stage T2 (44%, n = 15). Most of the patients were presenting for direct laryngoscopy (DL) and biopsy (70%, n = 24). The average number of days between when the FFL was recorded by the otolaryngologist and the intubation/surgery date was 12.82 (SD = 9.22) 95% CI. Demographic details of the patients are summarized in Table 1.
Patient Demographic Information.
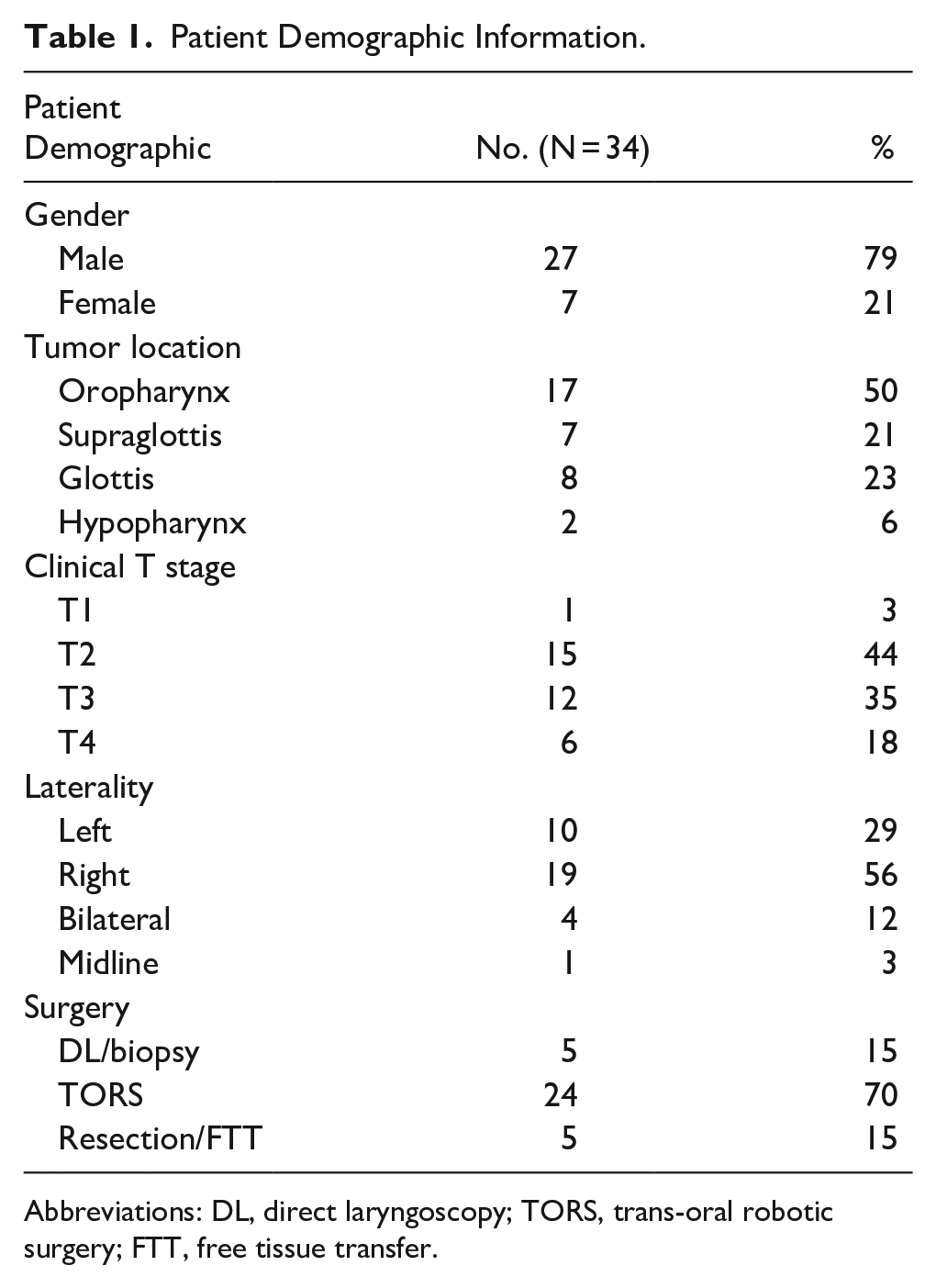
Abbreviations: DL, direct laryngoscopy; TORS, trans-oral robotic surgery; FTT, free tissue transfer.
Of the 34 patient intubation plans, 23 plans were not changed, while 11 plans (32%) were changed after the anesthesia care team reviewed the FFL. Assuming 32% of the subjects in the population have the factor of interest (change in intubation plan), the study would require a sample size of 335 for estimating the expected proportion with 5% absolute precision and 95% confidence. Regarding the 34 completed intubations, 9 (26%) were executed based on the plan after reviewing the FFL (after-scope plan), 21 had no changes after reviewing FFL and were executed accordingly (before-scope plan), and 4 used neither plan. All of the plans were made by the anesthesia care team which included the attending anesthesiologist and either the anesthesia resident or the nurse anesthetist.
The 9 after-scope intubation plans had 12 total changes: 3 were considered de-escalations of the intubation plans while the other 9 were considered tumor-related escalations of the intubation plans. The 3 de-escalation modifications were change from video laryngoscopy (VL) to DL, change from awake fiberoptic intubation (FOI) to VL, and upsizing of the endotracheal tube (ETT). Interestingly, the change from VL to DL was the only clinically staged T2 but pathologically staged T1 tumor in the series. The 9 escalations of the intubation plans included 4 changes from DL to VL, 1 change in type of VL to a thinner blade, more agile (i.e., cordless) model, 2 downsizing of the ETT, 1 conversion to spontaneous breathing from use of paralysis, and 1 escalation to a higher acuity operating room (OR) in case of an emergency. Two of the 11 intubations were changed but did not follow through with the after-scope intubation plan. One chose DL (with VL on standby) from VL after reviewing the FFL. In this case, there was a grade 1 view on DL; however, the view was noted to be distant so it was decided to proceed with VL.
There were 4 intubations that used neither the before- or after-scope plans. One of 4 did change the plan after reviewing the FFL but used a different intubation plan. In this case, the after-scope intubation plan intended to proceed with an awake FOI with a size 6.0 ETT. The intubation was successful with a combination awake FOI and video laryngoscope method with a 6.0 ETT. The 3 other intubations that used neither the before- or after-scope plan had intended to use the before-scope plan but used an alternative one: one upsized the ETT for an unknown reason, one required a bougie due to difficulty with positioning of the nasotracheal tube, and the third resulted in an emergent surgical airway after failure to pass an ETT, without any further complication. This last case highlights that even with the addition of FFL, these emergent events are still possible with the difficult airway. These results are summarized in Figure 2.
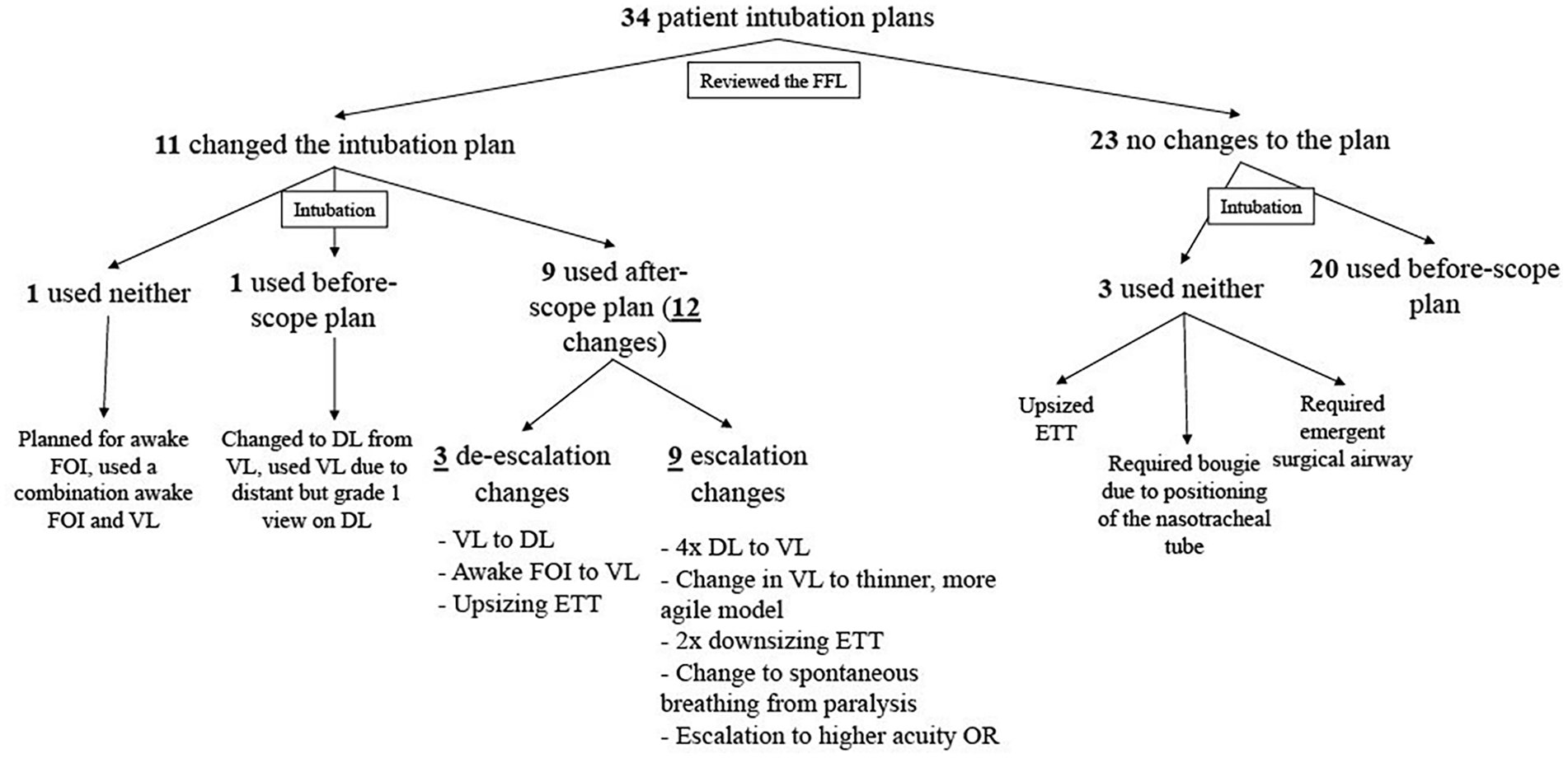
Intubation flow chart.
While this was a small pilot study, no significant associations were seen between change in intubation plan or intubation plan used and tumor location or stage. In 26 of the cases, the attending anesthesiologist filled out the subjective satisfaction postoperative survey. Seventy-seven percent (n = 20) of the attending anesthesiologists agreed or strongly agreed that seeing the FFL was more helpful than reading the findings in the clinic notes, while 88% (n = 23) of them agreed or strongly agreed that reviewing the FFL was helpful in creating the intubation plan. Ninety-two percent (n = 24) agreed or strongly agreed that they would want to review the FFL for all future difficult airways (Figure 3).
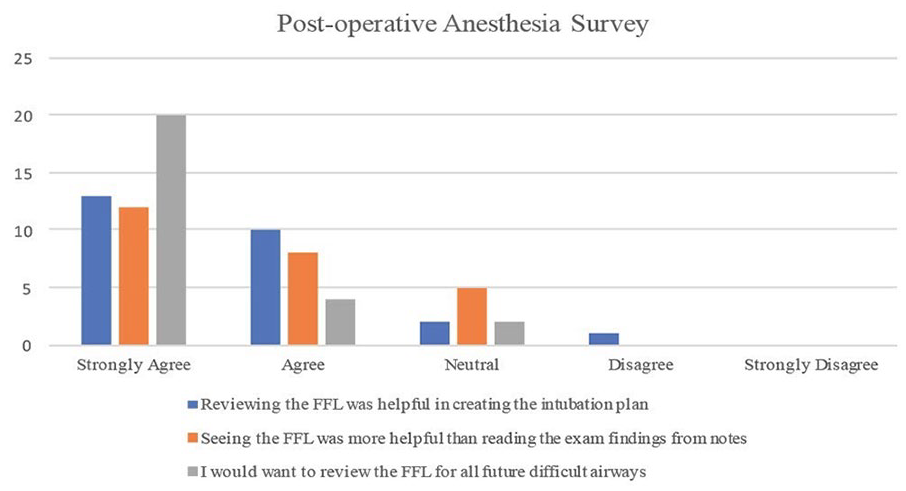
Anesthesia’s postoperative subjective feedback survey.
Discussion
The difficult airway is a subject that is thoroughly discussed and researched within both the anesthesiology and otolaryngology literature. A difficult airway, as described by the 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway, refers to a clinical scenario where an a physician trained in anesthesia care encounters expected or unexpected challenges or failures in performing tasks such as facemask ventilation, laryngoscopy, ventilation with a supraglottic airway, tracheal intubation, extubation, or using an invasive airway technique. 14 Despite the introduction of advanced technologies and strategies, patients with head and neck cancer still present challenges during intubation, encountering a higher frequency of adverse events. Their susceptibility to adverse intubation outcomes is increased due to the likelihood of having friable and bleeding tissue, along with limited mouth opening resulting from their head and neck pathology.
A study from the United Kingdom completed a 1-year audit of the major complications of airway management in anesthesia. Of the 133 major airway-related events (defined as death, brain damage, emergency surgical airway or unanticipated intensive care unit admission) in the peri-operative period, 55 (41%) were associated with head and neck pathology. 15 FFL have been implemented in head and neck oncology clinics for decades to visualize and stage tumors of the upper aerodigestive tract. 16 However, FFL is not frequently used as a preoperative airway assessment technique by anesthesiologists at our institution and others.7-11 In one study by Guo et al, predictive factors for difficult intubation were studied in 994 patients; the study found that flexible fiberoptic laryngoscopy, as a predictive factor, had a higher sensitivity, specificity, and positive predictive value than the Mallampati Test or the Wilson Risk-Sum score. 17
A study conducted by Rosenblatt et al studied the association of a preoperative FFL and unnecessary awake FOI. One hundred thirty-eight patients with head and neck pathology underwent FFL by the anesthesia team in the preoperative suite. Twenty-eight airway plans changed from awake FOI to induced direct laryngoscopy/video laryngoscopy (DL/VL) and 8 plans changed from induced DL/VL to awake FOI. 18 Further, Moorthy et al describes in their article, published in the Journal of Clinical Anesthesia, a systematic approach to securing the airway in patients with laryngeal tumors. Their multidisciplinary approach incorporates a preinduction day-of-surgery otolaryngologist’s FFL in their intubation algorithm. 19 While a day-of-surgery FFL could influence anesthesia’s intubation plan, as described by Rosenblatt et al and Moorthy et al, it is not always feasible.
The objective of our pilot study was to evaluate the subjective and objective impact of FFL, conducted as a routine assessment by otolaryngologists, on patients with stage T2 and greater cancers of the upper aerodigestive tract. The goal was to provide the anesthesia care team with a quick and convenient method to improve patient safety in a population prone to adverse events, without incurring additional costs or morbidity to the patient. Our pilot study found that FFL changed the anesthesia team’s intubation plans 32% of the time (n = 11) and that the anesthesia team executed the plan made after reviewing the FFL 26% of the time (n = 9). The majority of the changes made from reviewing the FFL were tumor-influenced escalations (n = 9) including upgrading laryngoscope type, downsizing endotracheal tube size, avoiding paralysis and escalation to a higher acuity OR. One of the de-escalations made after reviewing the FFL changed the plan from awake FOI to induced VL in a poor awake FOI candidate. These de-escalation changes have been shown to be of equal merit in the literature. 20 While some have guarded against using the FFL to reduce the number of awake FOI, the goal of our study was to observe the use of the FFL in our anesthesia teams’ intubation algorithm for a quality improvement measure. 21 Further, some question using the otolaryngologist’s FFL to help guide airway management due to the delay between when the FFL was recorded by the otolaryngologist and time of intubation. One could argue that there could be potential change in tumor features if there is too much time between when the exam was performed and recorded in clinic and when the intubation or surgery is planned. This would make the FFL less than helpful or even misleading. However, our study shows that the average number of days between the two was 12.82 (SD = 9.22). This average included the patients who presented through both the head and neck clinic and the emergency department.
In addition to objective data, we wanted to gather subjective satisfaction feedback on the usefulness of the FFL. The overwhelming majority of attending anesthesiologists agreed or strongly agreed that reviewing the FFL was more helpful than reading findings of the FFL in our clinic notes (77%, n = 20), the FFL was helpful in creating the intubation plan (88%, n = 23), and that they would want to review FFL for all future difficult airways (92%, n = 24). In cases where the FFL did not alter the intubation plan, anesthesia care team members noted that the information obtained from the FFL was consistent with their preexisting assessment based on clinical notes and imaging, thus not providing additional value. Additionally, for certain attending anesthesiologists, the routine reliance on their established intubation protocols and experience may have overshadowed the perceived necessity of the FFL.
Detailed case descriptions highlight how the identification of specific oropharyngeal-laryngeal lesions via FFL led to modifications in the anesthesia plan. For example, a lesion causing significant airway narrowing prompted an escalation from DL to VL, ensuring better visualization and control during intubation. In another case, a large obstructive mass influenced the decision to downsize the ETT to facilitate smoother passage through the airway. These targeted adjustments underscore the practical utility of FFL in optimizing intubation strategies tailored to individual patient anatomy and pathology. While the literature on FFL and intubation plans is sparse, we believe FFL offers important information when creating intubation plans for patients with head and neck cancer and can even change plans in approximately a third of the cases.
Limitations and Future Directions
This pilot study has limitations, with the primary constraint being the sample size and selection criteria. The study included a relatively small number of patients, which mean the results may not fully represent the broader population of patients with these cancers. This limitation potentially affects the robustness of the study’s conclusions and limits the generalizability of the findings. Furthermore, we elected to limit the eligibility to T2 and greater cancers of the oropharynx, hypopharynx, and larynx in this study. Including T1 tumors would have likely decreased change in intubation plan percentiles. For example, there was one clinical T1 versus T2 tumor of the 34 patient cases in which the FFL did not change the intubation plan. For the sake of focusing on a patient population with known difficult intubations, only patients with squamous cell carcinoma of the upper aerodigestive tract were included in the study. However, future studies could include any airway obstruction and a control group to make comparisons. Grouping all patients who presented through the ED and the outpatient clinics has its limitations. The heterogeneity and severity of conditions treated in the ED can lead to a more varied study population and potentially to higher stage tumors, complicating data control and analysis. Additionally, the fast-paced ED environment may result in rushed assessments and incomplete data, thereby compromising data quality. Furthermore, due to the study being a prospective, observational study, the anesthesia care team could have biased changes in their intubation plans after reviewing the FFL. Asking for feedback only after the anesthesiologist had seen the video and intubated the patient may have influenced how they recorded their initial intubation plan. Future studies could focus further on decision-making regarding changed plans.
Conclusions
Head and neck cancer can increase the difficulty of airway management for anesthesiologists and can increase the morbidity and mortality associated with undergoing general anesthesia for patients. Maximizing patient safety in this patient population during intubation necessitates the imperative utilization of all available resources by the providers. FFL are an essential part of the work up of an oropharynx, hypopharynx, or larynx tumor for the otolaryngologist and provide a unique and dynamic examination of the airway. FFL examinations provide important information to the anesthesia team’s intubation plan and may change that plan in up to a third of cases.
Footnotes
Authors’ Note
This study was presented at the American Head & Neck Society International Conference on Head & Neck Cancer in Montreal, Canada, July 9, 2023. There are no prior published, posted or submitted papers from this same study.
Author Contributions
A.C.G. contributed to the conception, design, and implementation of the research, to the analysis of the results, writing of the manuscript and presentation of the research; S.F. contributed to writing, editing and submission of the manuscript; K.D. contributed to the conception, design, and implementation of the research, to the analysis of the results and to the writing of the manuscript; D.K. contributed to the design and implementation of the research, to the analysis of the results, and to the writing of the manuscript; M.M. contributed to the design and implementation of the research, to the analysis of the results, and to the writing of the manuscript; J.S. contributed to the design and implementation of the research, to the analysis of the results, and to the writing of the manuscript; E.V. contributed to the conception, design, and implementation of the research, to the analysis of the results, writing of the manuscript and presentation of the research.
Data Availability
The data presented in this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Approved by the University of Arkansas for Medical Sciences Institutional Review Board: IRB# 273909