
Abstract
Sudden idiopathic hearing loss (SIHL) is defined as sensorineural hearing loss at 30 dB or more at 3 consecutive frequencies that begins within 72 hours, and the etiology of the disease is still unclear. Steroid treatment is used as systemic and local (intratympanic) in sudden hearing loss, and different results have been reported for both treatment modalities. This study aimed to compare the results of the treatment in patients who received systemic steroid (SS) therapy and in patients who received systemic and intratympanic steroid (ITS) therapy for SIHL. In all, 169 patients who were admitted to our clinic with the diagnosis of SIHL between January 2007 and June 2018 were randomly divided into 2 treatment groups according to their admittance day, such as patients who received only SSs and patients who received SSs and ITSs. The results of these 2 treatment protocols were investigated. Statistical analysis was performed for all patients by grouping many factors that could be effective in prognosis, such as age, sex, and time of initiation of treatment. No differences were found between the SS group and the combined systemic-ITS group in treatment success. It was determined that being under 15 years of age, over 60 years of age, starting treatment after 7 days, vertigo, high initial hearing loss, descendant type, and total loss type in the audiogram configuration are poor prognostic factors. Being between 16 and 59 years of age, starting treatment within 7 days, having no vertigo, mild hearing loss, and having ascendant and plateau type in audiogram configuration are good prognostic factors. We observed that adding ITS treatment to SS treatment as an initial treatment did not provide any extra benefit. However, prospective, randomized, controlled studies will clarify the topic.
Introduction
De Kleyn first described sudden idiopathic hearing loss (SIHL) in 1944. It is a condition of sensorineural-type hearing loss that begins within 72 hours and detects hearing loss of 30 dB or more at 3 consecutive frequencies.1,2
Etiology can be detected in only about 10% of SIHL, comprising approximately 1% of all sensorineural hearing losses. 3 Many factors, such as viral infections, vascular events, autoimmunity, and drugs, have been blamed for SIHL, whose etiology has yet to be elucidated.4,5 Although it constitutes 1% of all sensorineural hearing loss, SIHL is a critical pathology of the ears, nose, and throat because auditory functions are reversible with early diagnosis and treatment.
Although SIHL can occur at any age, it most commonly affects patients between 45 and 55 years of age, and both genders are affected equally.5,6 SIHL is very rare in childhood. It occurs between 5 and 77 per 100,000 people yearly. Unilateral hearing loss develops in most patients, but bilateral hearing loss may also occur in approximately 3% of cases. 7
Many prognostic factors have been reported in SIHL. Initial hearing loss level, advanced age, audiogram type, presence of chronic diseases such as diabetes and hypercholesterolemia, and accompanying vestibular symptoms such as tinnitus-vertigo change the prognosis positively or negatively. Although tinnitus occurs in 41%-93% of patients with SIHL, vertigo has been reported in 29%-56% of these patients.5-7
Since the etiopathogenesis of SIHL cannot be clearly explained, debates continue about treatment. Spontaneous recovery rates vary between 32% and 65% in studies.6,8 However, as a result of the survey by Wilson et al. 1 in 1980 and supported by other studies, steroids became the only agent with proven effectiveness. With the use of steroids, the recovery rate in SIHL increases to 49%-89%, exceeding spontaneous recovery rates. In addition, hyperbaric oxygen therapy, vasodilators (histamine, pentoxifylline, nifedipine, papaverine, etc.), antiviral agents (acyclovir, valacyclovir), vitamins (vitamin E), viscosity reducing agents (dextran, heparin, etc.), and other treatments can also be applied. 1
Steroids were initially administered systemically in treating SIHL, but later, they began intratympanic application. Intratympanic steroid (ITS) can be used in combination with systemic steroid (SS) as an alternative to SSs or as a rescue therapy at the end of SS treatment. 1
This study aimed to compare the results of treatment in patients who received SS therapy and in patients who received systemic and ITS therapy for SIHL.
Materials and Methods
This study was started after receiving the approval of the faculty ethics committee dated 06.06.2018 and numbered 24237859/368 at Karadeniz Technical University, Department of Ear, Nose, and Throat.
The study group consisted of patients hospitalized and treated in our ENT service diagnosed with “sudden idiopathic hearing loss” between January 2007 and June 2018. They were randomly divided into 2 groups related to their admittance day. Specialists (SA and BK) who were on duty every other day were used to apply different treatment protocols. Therefore, patients who applied on odd days received only SSs, whereas the patients who were admitted on even days received SSs and ITSs combined.
The patient’s age, the day of hearing loss when he applied to the clinic, and whether he has any other symptoms and comorbidities accompanying the hearing loss are recorded. Routine blood tests are performed during hospitalization, and biochemistry, complete blood count, coagulation parameters, blood lipid panel, thyroid function tests, vitamin B12, and folic acid levels are routinely studied. Patients are requested to have an ear magnetic resonance imaging as a radiological examination.
Intravenous sodium succinate (IV) methylprednisolone, which is adjusted according to weight (1 mg/kg), is administered as a treatment to patients hospitalized with a diagnosis of SIHL. In addition to SSs, 4 mg/ml of dexamethasone is administered to some of these patients by applying a volume of 0.5-1 ml to the tympanic cavity from the posteroinferior quadrant of the tympanic membrane with a dental injector under local anesthesia (Xylocaine) using an oto-microscope in the semifowler position. After application, patients are asked to wait 30 minutes. They are only asked to move or swallow once. In addition, all patients receiving hospitalized treatment in our clinic are routinely given intravenously magnesium sulfate for 5 days and daily enteral vitamin B and E preparations. Pure tone audiometry is performed on patients at 250-, 500-, 1000-, 2000-, 4000-, and 8000-Hertz (Hz) frequencies to check their pure tone thresholds. Audiograms are repeated on the 3rd, 5th, 7th, and 10th days of treatment, and the control audiograms are performed on the 1st month after discharge and on the 3rd month to evaluate the final hearing levels.
Although hearing loss that developed within the last 3 days is mentioned in the definition of SIHL, patients whose complaints started within the previous 7 days were evaluated in our study.
To examine the effect of gender on the course of SIHL, the patients were divided into 2 groups, male and female, and compared in terms of recovery rates after treatment.
The patients were grouped according to whether or not they had vestibular symptoms (tinnitus, vertigo) accompanying hearing loss. It was evaluated whether there was a relationship between the presence of these symptoms and recovery rates and which symptoms resulted in less recovery.
The ears in which hearing loss developed were grouped as right and left and compared concerning recovery rates. The patients’ audiogram types were divided into 4 groups: ascending, flat (plateau), descending, and total loss. The literature states that ascending and flat audiograms are better in terms of prognosis. The ascending and flat audiograms were divided into 1 group, and the descending and total loss audiograms were divided into the other. The groups were compared in terms of recovery rates. Furthermore, each group was compared individually in terms of recovery rates.
Patients were grouped according to their average pure tone at the time of admission: 20-39 dB for mild, 40-69 dB for moderate, 70-89 dB for severe, and 90 dB and above for very severe total hearing loss. These groups were then compared in terms of recovery rates.
Patients who received only intravenous SSs as treatment and patients who received SSs and ITSs were compared as 2 separate groups in terms of recovery rates after treatment.
In the evaluation of the response to treatment, patients were evaluated as having a hearing gain of less than 15 dB according to the first pure tone average (PTA) or “no improvement” if the final hearing level was greater than 75 dB in the final audiogram examinations taken in the third month after treatment. A hearing gain of more than 15 dB and “slight improvement” if the final hearing level is between 46 and 75 dB, “partial improvement” if the final hearing level is between 26 and 45 dB, and a hearing gain of more than 15 dB and “partial improvement” if the final hearing level is 25 dB and below were grouped as “complete recovery.” 9
The Statistical Package for Social Sciences (SPSS, INC, an IBM Company, Chicago, Illinois) version 23.0 program was used for statistical analysis. The “chi-square test” was used to compare qualitative data. The level of statistical significance was accepted as P < .05.
Results
When affected ears were evaluated, proper involvement of the ears was observed in 80 patients (47.3%), participation of the left ear was observed in 81 patients (47.9%), and bilateral involvement was observed in 8 patients (4.8%). The age distribution of patients who received treatment with a diagnosis of SIHL was between 6 and 74 years, and the average age of all patients was 41.44 (±16.79).
The patient’s audiograms at admission are also calculated by taking the arithmetic mean of the hearing thresholds at 500, 1000, 2000, and 4000 Hz. Those with pure tone averages (PTA) between 20 and 39 dB have mild hearing loss; those with 40-69 dB have moderate hearing loss; and those with 70-89 dB have moderate hearing loss. Those with a hearing loss of 90 dB or greater were grouped as having severe hearing loss. The numerical data of these groups are shown in Table 1.
Distribution of Patients According to Degree of Hearing Loss at Presentation.
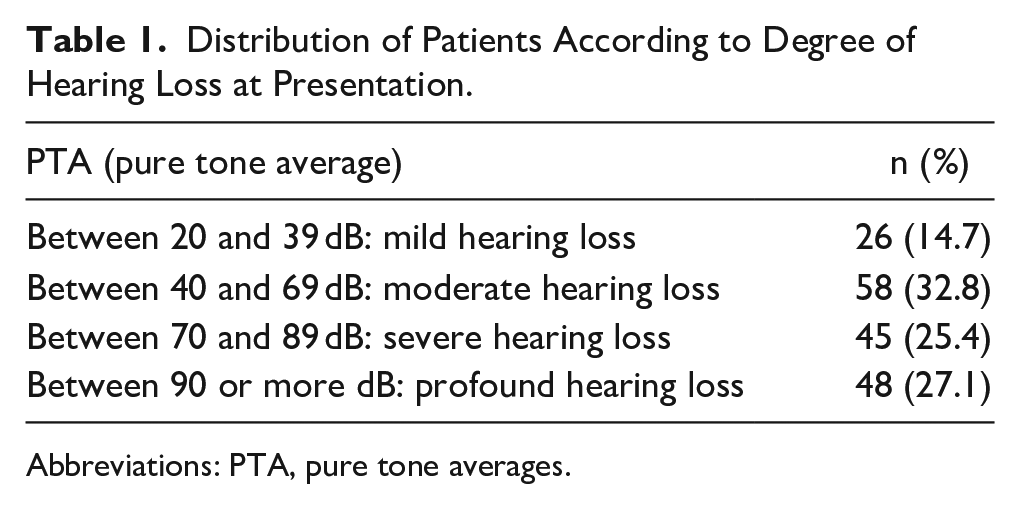
Abbreviations: PTA, pure tone averages.
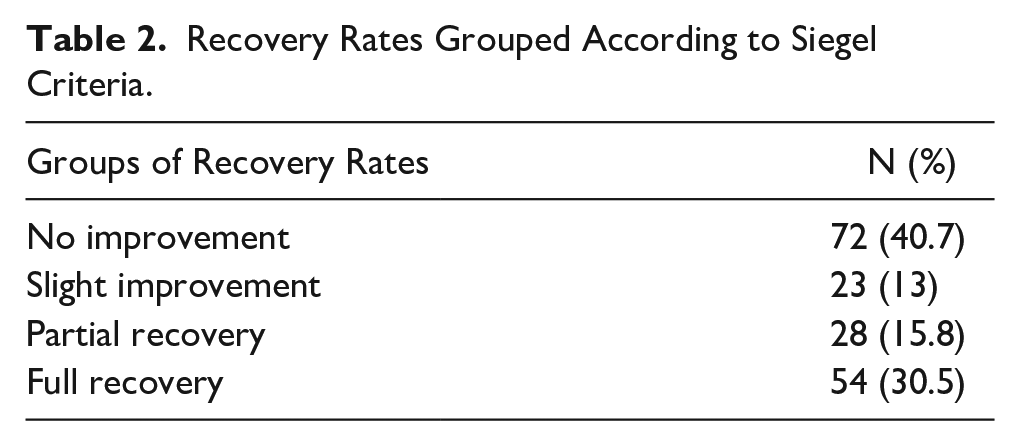
The patients were classified into 4 groups according to the improvement criteria defined by Siegel et al. in 1975 concerning the change rates between their first audiogram at the time of admission and their audiogram at the third month after treatment when they reached their final hearing level. According to the Siegel criteria, if the PTA in the last audiogram improved by less than 15 dB compared to the PTA in the first audiogram or if the PTA in the previous examination was worse than 75 dB, it was accepted as no improvement. There was a slight improvement if this difference was more than 15 dB, and the PTA in the last audiogram was between 46 and 75 dB. It was considered a partial improvement if the difference was greater than 15 dB and the previous PTA was between 26 and 45 dB. If the PTA in the last audiogram was better than 25 dB, full recovery was supposed to exist. The recovery rates of the patients according to Siegel criteria are given in Table 2.
Recovery Rates Grouped According to Siegel Criteria.
The treatment results of our 2 groups of patients receiving SS and SS + ITS treatment were compared and grouped by age or gender. The improvement rates of the patients in total, or according to sex or age, were statistically evaluated with the chi-square test, and no significant differences were observed between the 2 treatment groups (P = .0572).
The patients were divided into 2 groups according to whether the affected ear was right or left and the recovery rates after treatment were compared between these groups. While no improvement was observed in 41 (46.6%) of the 88 right ears diagnosed with SIHL, there was a slight improvement in 12 (13.6%), partial improvement in 11 (12.5%), and 24 (27%). Complete recovery was observed in 3. Furthermore, no improvement was observed in 31 of 89 pathological left ears (34.8%), a mild improvement in 11 (12.4%), a partial improvement in 17 (19.1%), and a partial improvement in 30 (33%). Complete recovery was observed. No statistically significant differences existed between the right and left ear recovery rates (P = .052) (Table 3).
Comparison of Systemic Steroid Versus Combined Systemic-Intratympanic Steroid Treatment Groups (P = .0572, P > .05).
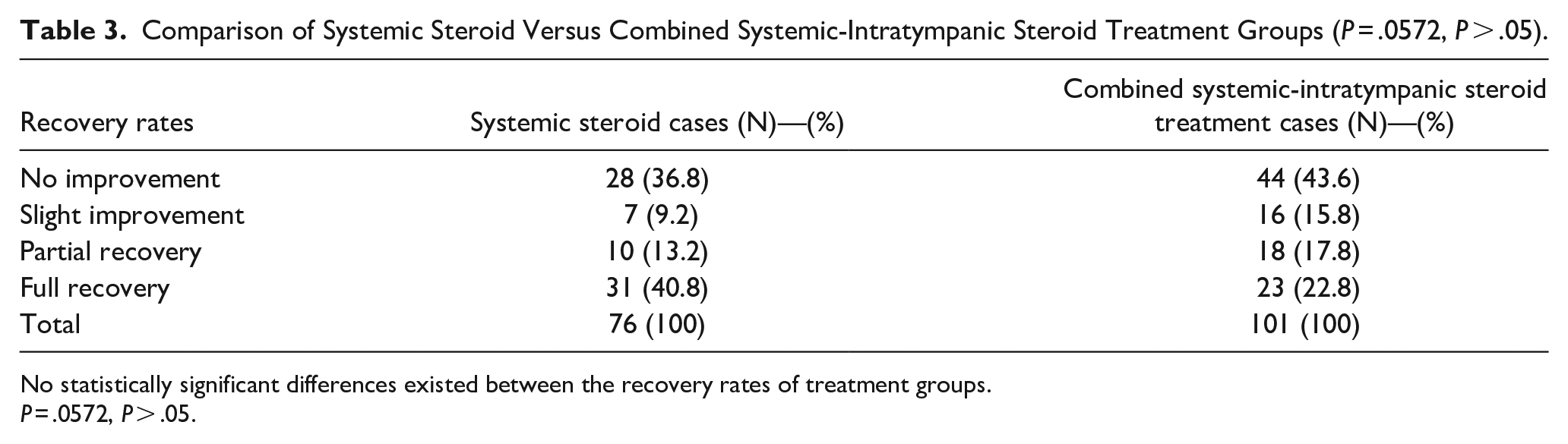
No statistically significant differences existed between the recovery rates of treatment groups.
P = .0572, P > .05.
When patients were evaluated according to age, the recovery rate was higher in patients between 16 and 59 years compared to those under 16 and over 60 (P = .043).
There was also no correlation between recovery level and accompanying vertigo or tinnitus.
Discussion
Steroids are currently the only drug group whose effectiveness in the treatment of SIHL is widely accepted. However, there are many studies and many different recommendations on the dosage and method of administration of steroids. In addition to systemically administered steroids, local application has also been applied in the last few decades to reduce side effects and increase treatment effectiveness. We investigated the effect of ITS treatment on treatment results when we added ITS treatment as a local steroid application to SS treatment. We found that applying ITS treatment simultaneously with SS treatment did not increase treatment success.1,9
In the SIHL clinic, many factors that affect the prognosis are emphasized. In our study, we focused on the factors that could be effective. According to the study results, being in the childhood age group (under 15 years of age) and over 60 years of age, the presence of vertigo, starting treatment after 7 days from the onset of the clinical picture, and the presence of severe hearing loss (70-89 dB) and very severe (90 dB and above), we can say that audiogram configuration in descending and total hearing loss types are poor prognostic factors.
Very few articles mention that gender impacts the prognosis. In 2004, Samim et al mentioned that male sex is a poor prognostic factor. 10 On the contrary, in 2007, Ceylan et al 11 mentioned that the female gender is a poor prognostic factor for SIHL.
As in other diseases, age has been studied as a natural evaluation criterion in the SD clinic. The most common age is observed to be between the ages of 45 and 55. 12 In our study, the average age was found to be 41.44. Furthermore, the effect of age on prognosis has also been studied. Among all patients with SIHL, the average number of pediatric patients is 6.6%. 11 It is generally known that the prognosis is worse in the childhood and older age groups. Our study divided patients into 3 groups: young patients under 15, elderly patients over 60 and middle age, and the middle age group. Patients in these 3 age groups were evaluated regarding recovery rates after treatment. Recovery rates were found to be lowest in the young patient group, aged 15 and under, and the recovery rates were highest in the middle-aged group. In other words, our study supports the idea that age is an influential prognostic factor in the SIHL clinic, consistent with the general literature. 13
Hearing results have been reported to be poor in patients under 14-15 and over 60. 14 Nakashima et al 15 mentioned that SIHL development in the childhood age group progresses with more advanced hearing loss. 15 These data are supported by current articles on childhood patients published in the last few years.16,17 However, contrary to these data, a study stated that treatment results in pediatric patients are more successful than in adults. 14 In addition, many published studies mention that advanced age (over 60) is a poor prognostic factor.15-17 Increased cellular degeneration specific to the aging process and low metabolic and cellular regeneration potential may explain the poor prognostic effect in older age. Young age may be effective in a poor prognosis because the immune system is not fully developed and does not function optimally. Furthermore, studies in the literature state that age does not affect prognosis in SIHL. 17
The benefit rates of patients who applied in the first 3 days and those who applied between 4 and 7 days were significantly higher than those who applied in 8 and above days. Early initiation of treatment is considered one of the most effective positive prognostic factors. Similarly, many studies have reported that early-onset treatment positively affects final hearing thresholds. 18
Tinnitus in our patients was determined to have no positive or negative effect on their treatment success. When we look at the literature, some studies assess tinnitus as a favorable prognostic factor, while others evaluate it as an adverse prognostic factor. Acute tinnitus is believed to occur due to impaired cochlear activity. It is thought that impaired cochlear functions cause decreased signal transmission in auditory pathways, and as a result, increased spontaneous signal production occurs in neurons in this pathway. As a result, it is stated that this causes the perception of tinnitus in the auditory cortex.16-18 Tinnitus indicates that the inner ear’s hair cells are still alive and that tinnitus is a favorable prognostic factor for SIHL. Similarly, many studies support this hypothesis.16-18
ITS has been used as a follow-up rescue therapy, combined therapy with SSs, and primary therapy alone in patients who do not benefit from SSs. In our study, patients receiving IV SS and those receiving combined SS and ITS were evaluated regarding the results and effectiveness of the treatment. As a result of our comparison, no statistically significant differences were detected between combined treatment and SS treatment alone (P = .067 compared to 4 groups: no improvement, mild, partial, and complete; P = .367 compared to 2 groups without improvement and present).
As a result, it was concluded that combined treatment continues to be used in some centers, even though it is not evidence based, to use all the treatment options available to us, as there is no chance of replanning the treatment for a sensory loss whose etiology is unknown.
Footnotes
Acknowledgements
None.
Author Contributions
All authors contributed to the planning, designing, literature survey, and active intellectual support, writing, and editing.
Availability of Data and Materials
The rest of the data may be sent to academic inquiries.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Committee Approval
Ethics committee approval was taken from Karadeniz Technical University, Non-Invasive Clinical Research Ethics Committee, at 06.06.2018 and numbered 24237859/368.
Informed Consent
There is no need for informed consent because the data were evaluated retrospectively.