
Abstract
Introduction
Every year, nearly 3 million patients suffer from facial trauma in the United States, with the most common causes being assaults, traffic accidents, and falls. 1 Many patients who present to the emergency department (ED) with a facial fracture require hospital admission and further treatment of their injuries. 2 Treatment for facial trauma can incur large costs, with one report showing mean hospitalization and emergency department charges adding up to $62,000. 2 Complication rates from facial trauma and procedures for fracture fixation vary by fracture site, with mandibular fracture complication rates reported to be greater than 25% in some cases. 3 Other fracture sites, such as zygomaticomaxillary complex fractures and midfacial fractures, report lower rates of complications at around 6.2% to 20%.4,5 Orbital and nasal fractures generally demonstrate lower rates of infection-related complications with several studies finding less than 1% complications in these fracture types.6,7 Common surgical complications include wound dehiscence, surgical site infection (SSI), and fracture nonunion.
Well-known risk factors for adverse outcomes following surgery include tobacco use and immunosuppression. 3 The definition of immunosuppression is broad but can include patients with human immunodeficiency virus (HIV), diabetes, chronic kidney disease (CKD), and those on immunosuppressive medications. Immunosuppression impairs wound healing and increases the risk of infections as the body’s immune system is not able to effectively combat pathogens. 8 These patients may require close titration of immunosuppressive drugs, empiric broad-spectrum antibiotic use, and multiple wound debridement procedures. Furthermore, complications can be masked in immunosuppressed patients necessitating a high index of suspicion and heightened clinical attention to these patients. 9 However, little is known about which populations of immunosuppressed patients are at higher risks of adverse postoperative complications that may require more attention. While etiologies of immunosuppression are varied, our group chose to analyze groups of patients with common etiologies of immunosuppression including CKD, liver disease, HIV, diabetes, and those on immunosuppressive therapy. These groups were chosen as they are well-known contributors of immunosuppression and are relatively common among patients in the United States.10-16 This study aims to investigate the relationship between immunosuppression and postoperative outcomes in patients with facial fractures.
Materials and Methods
Data for this retrospective cohort study were collected from the TriNetX Research Network which includes electronic medical records from over 100 million patients and more than 70 health care organizations (HCOs) across the United States. The TriNetX Research Network provides users with clinical data, including demographics, diagnoses, imaging, laboratory results, medications, procedures, and other interventions. TriNetX is compliant with the Health Insurance Portability and Accountability Act (HIPAA). The Penn State Institutional Review Board reviewed and approved STUDY00018629 as exempt.
The database was queried using International Classification of Diseases (ICD-10) and current procedural terminology codes to identify patients who underwent facial fracture repair procedures. Patients were divided into 2 groups according to their immune status (immunosuppression vs no immunosuppression). Additional analyses were performed on subgroups of immunosuppression, including the use of immunosuppressive drugs, diabetes mellitus, CKD, liver disease, and HIV status to determine which groups were more at risk for postoperative complications. Patients were matched by demographic information and presence of comorbidities including cardiovascular diseases and use of anticoagulants. Each subgroup also underwent propensity score matching, with each treatment and control group having an equal number of participants. Corresponding diagnosis and procedure codes can be found in Supplemental Table 1, and a participant flow chart is located in Figure 1.
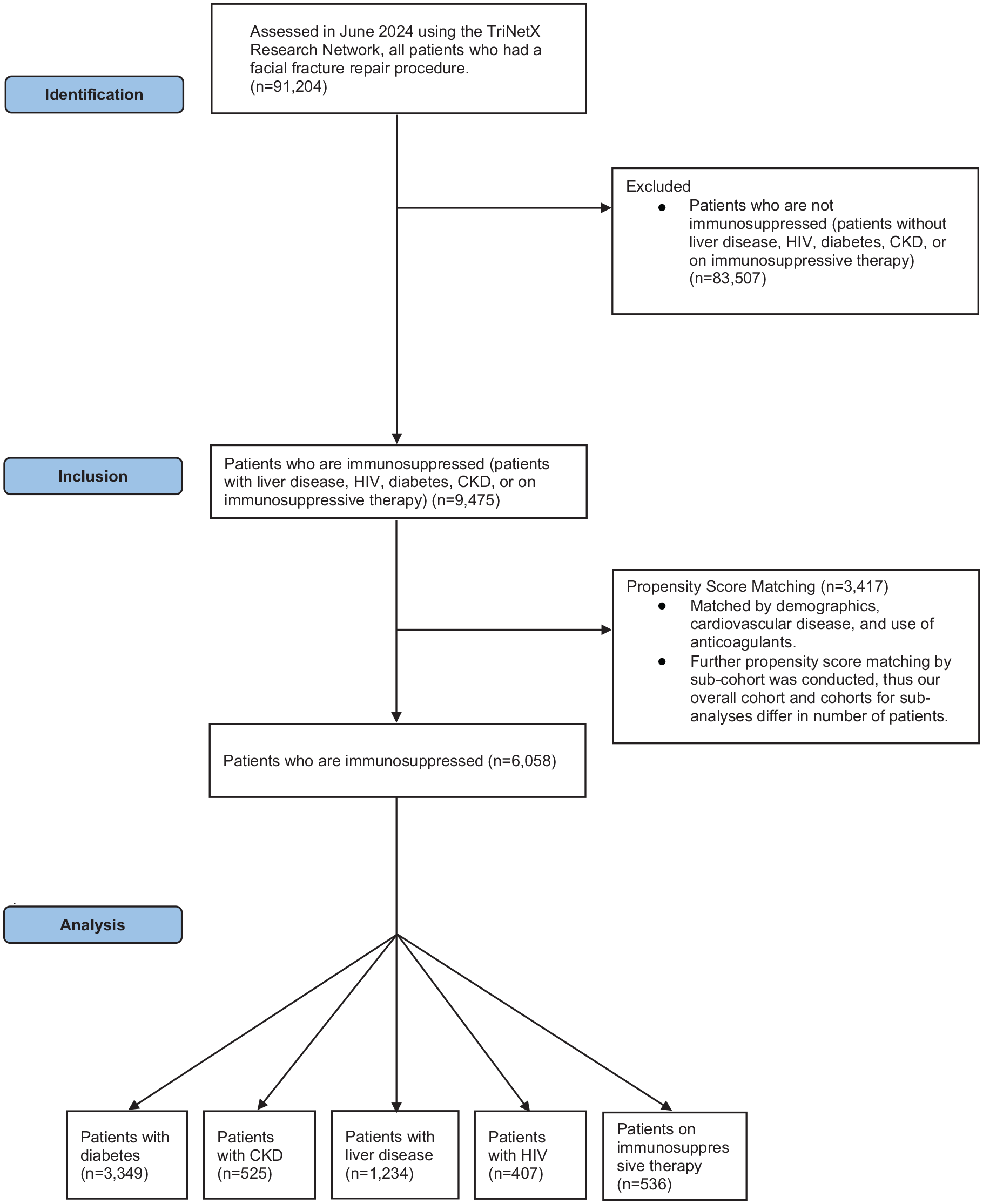
Strobe diagram.
Statistical analyses were performed within the TriNetX platform, which utilizes JAVA, R, and Python software. Relative risks and associated confidence intervals were used to calculate the risk of complications in patients with facial fracture procedures and concurrent immunosuppression. For outcomes or variables experienced by 1 to 9 patients, the TriNetX database rounds to 10. Therefore, analyses were not completed for outcomes with ≤10 patients.
Results
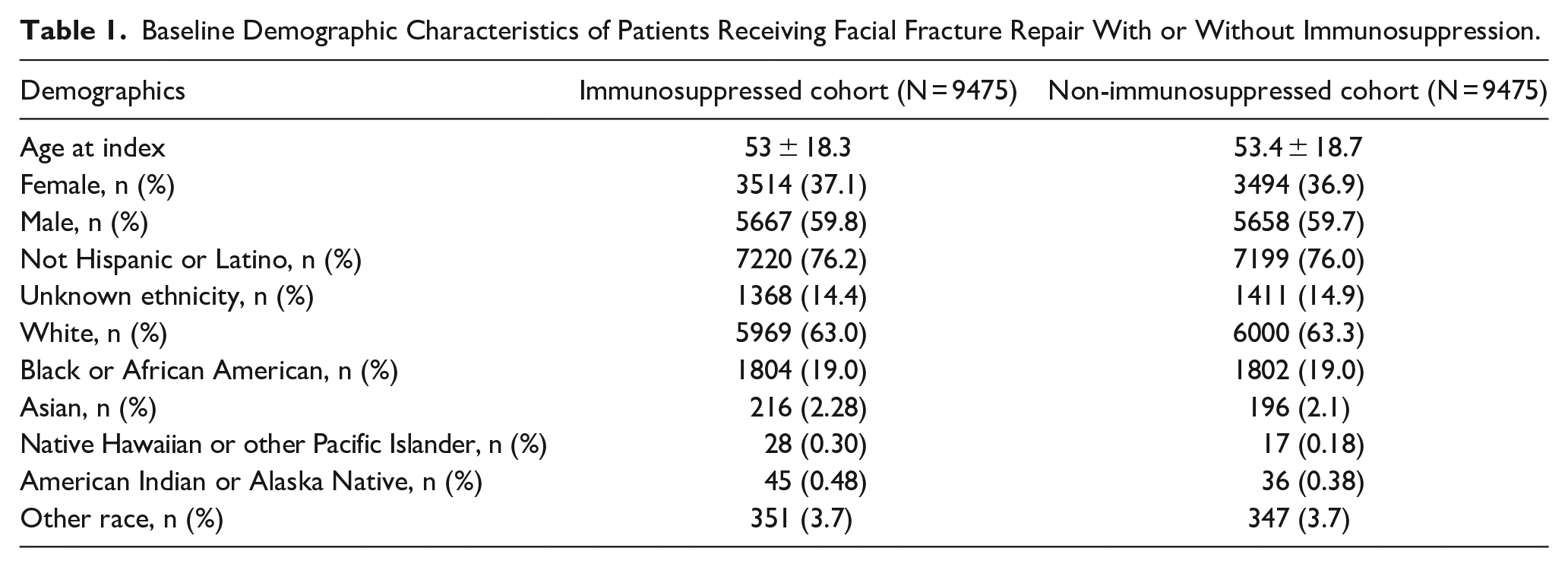
After propensity score matching, 9475 patients were identified for each cohort. Cohorts for subanalyses included 555 patients receiving immunosuppressive therapy, 429 patients with HIV, 619 patients with CKD, 1322 patients with liver disease, and 3133 patients with diabetes. Due to propensity score matching for each individual cohort, these numbers differ from our overall cohort. Mean ages at index were 53 ± 18.3 years of age in the immunosuppressed cohort, and 53.4 ± 18.7 years of age in the non-immunosuppressed cohort. The immunosuppressed cohort consisted of 59.8% males, and the non-immunosuppressed cohort consisted of 59.7% males. Baseline demographics and characteristics are shown in Table 1.
Baseline Demographic Characteristics of Patients Receiving Facial Fracture Repair With or Without Immunosuppression.
Overall, immunosuppressed patients were more likely to experience postoperative infections [odds ratio (OR) 1.37 (1.9-1.54), P < .001], thromboembolic events [OR 1.71 (1.33-2.20), P < .001], hemorrhage [OR 1.46 (1.10-1.92), P = .0087], hospital readmission [OR 1.36 (1.28-1.44), P < .001], subsequent emergency department encounters [OR 1.08 (1.01-1.15), P = .0249], and wound disruptions [OR 1.52 (1.17-1.97), P = .0017]. Separate analyses comparing outcomes by type of immunosuppression found increased rates of infection [OR 1.59 (1.25-2.01), P < .001], thromboembolic events [OR 1.56 (1.07-2.26), P = .0196], wound disruption [OR 1.57 (1.03-2.39), P = .0357], and hospital readmission [OR 1.28 (1.16-1.42), P < .001] in patients with diabetes. Patients on immunosuppressive therapy demonstrated lower rates of subsequent emergency department encounters [OR 0.54 (0.39-0.74), P < .001]. Patients with CKD demonstrated higher rates of infection [OR 2.02 (1.18-3.46), P = .0092] and readmission [OR 1.43 (1.14-1.79), P = .0017]. Patients with liver disease had higher rates of infection [OR 1.54 (1.07-2.23), P = .0210], thromboembolic events [OR 2.84 (1.37-5.87), P = .0033], and readmission [OR 2.14 (1.83-2.51), P < .001]. No significant differences were found between groups for death, fracture nonunion, or subsequent encounters for treatment of the fracture. The rates of postoperative complications following surgery in each cohort are listed in Tables 2 to 7.
Adjusted ORs and 95% CIs of Complications After Facial Fracture Repair Procedures.
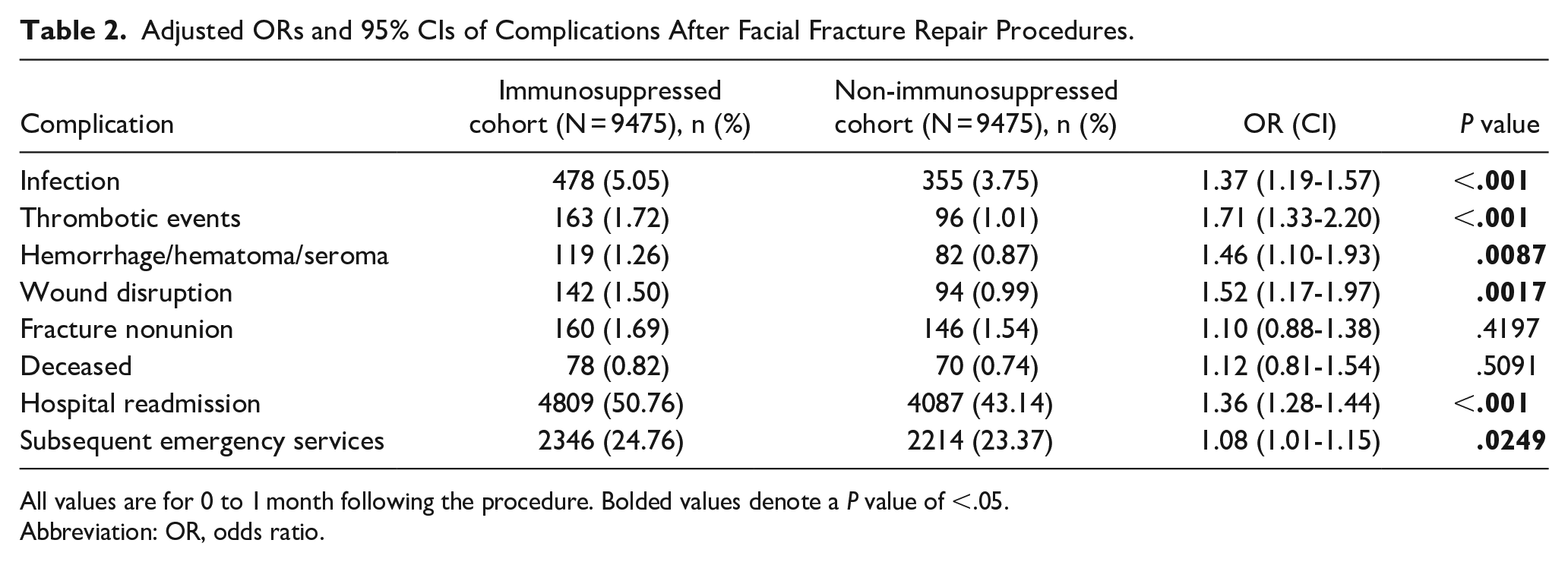
All values are for 0 to 1 month following the procedure. Bolded values denote a P value of <.05.
Abbreviation: OR, odds ratio.
Adjusted ORs and 95% CIs of Complications After Facial Fracture Repair Procedures in Patients With Diabetes.
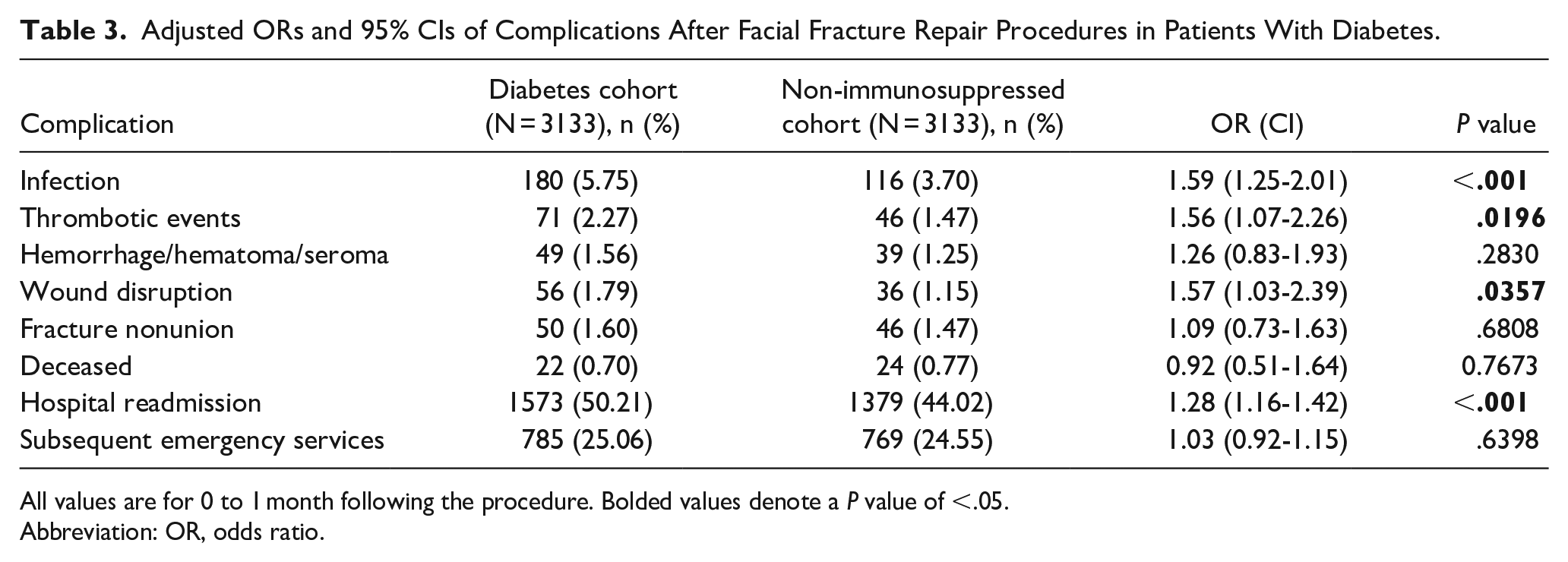
All values are for 0 to 1 month following the procedure. Bolded values denote a P value of <.05.
Abbreviation: OR, odds ratio.
Adjusted ORs and 95% CIs of Complications After Facial Fracture Repair Procedures in Patients With CKD.
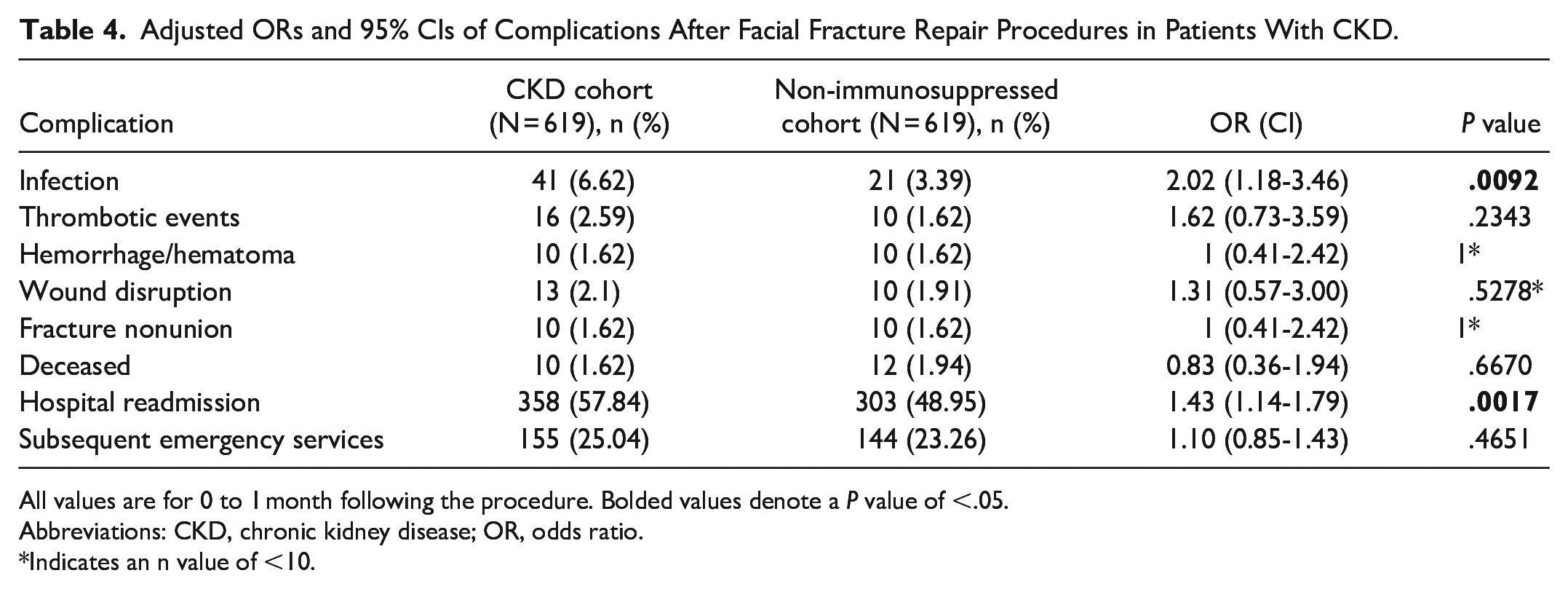
All values are for 0 to 1 month following the procedure. Bolded values denote a P value of <.05.
Abbreviations: CKD, chronic kidney disease; OR, odds ratio.
Indicates an n value of <10.
Adjusted ORs and 95% CIs of Complications After Facial Fracture Repair Procedures in Patients on Immunosuppressive Therapy.
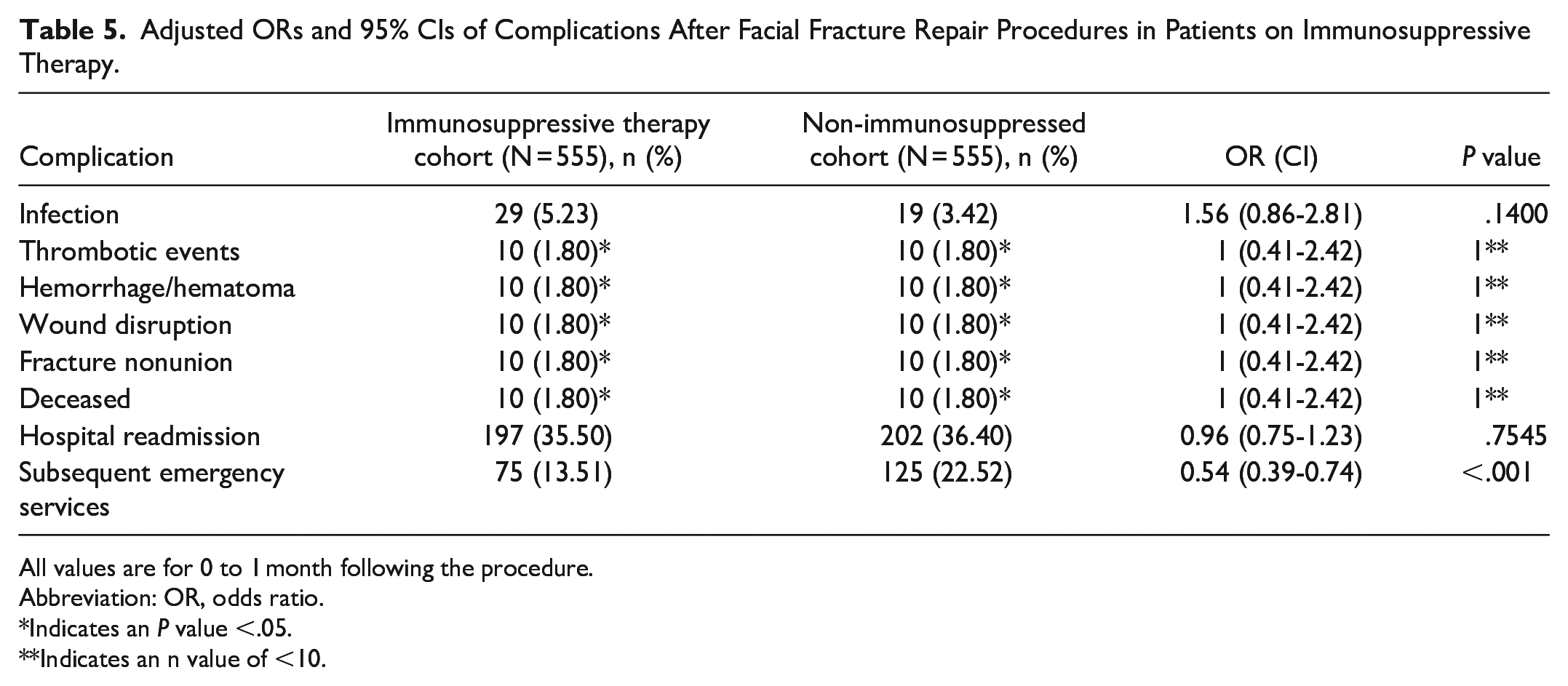
All values are for 0 to 1 month following the procedure.
Abbreviation: OR, odds ratio.
Indicates an P value <.05.
Indicates an n value of <10.
Adjusted ORs and 95% CIs of Complications After Facial Fracture Repair Procedures in HIV Positive Patients.
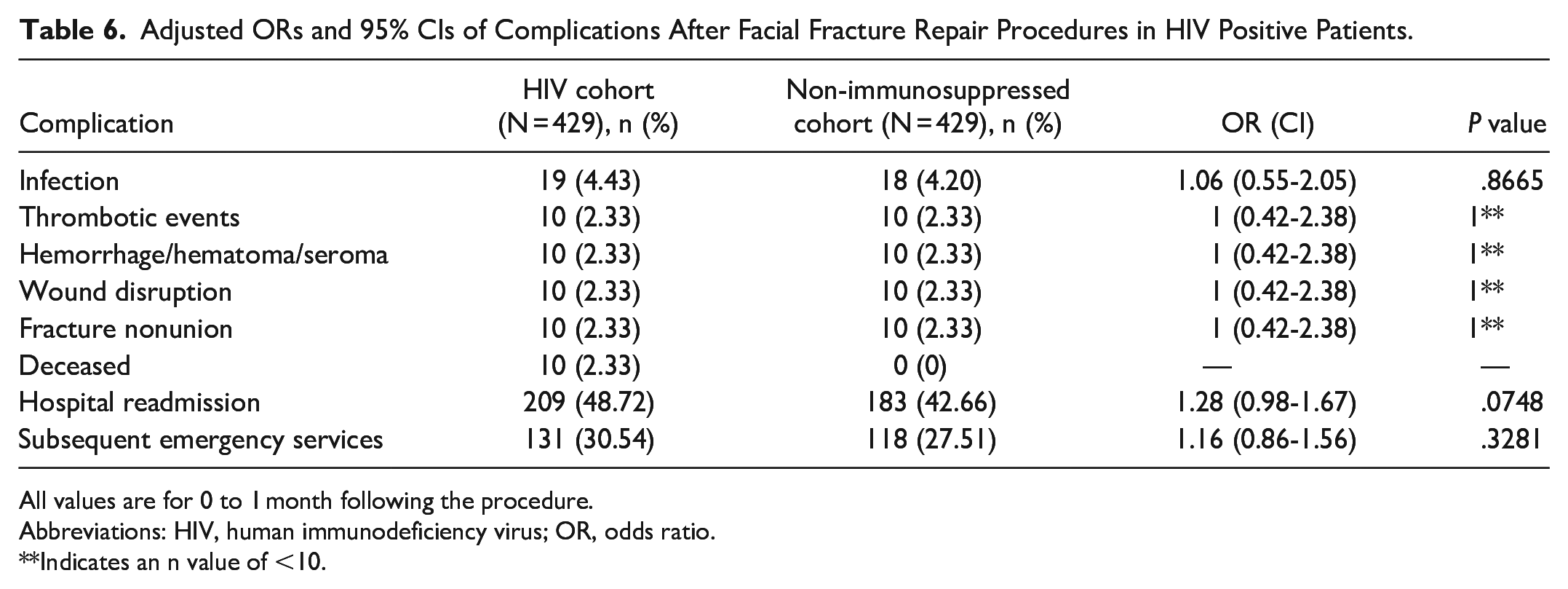
All values are for 0 to 1 month following the procedure.
Abbreviations: HIV, human immunodeficiency virus; OR, odds ratio.
Indicates an n value of <10.
Adjusted ORs and 95% CIs of Complications After Facial Fracture Repair Procedures in Patients With Liver Disease.
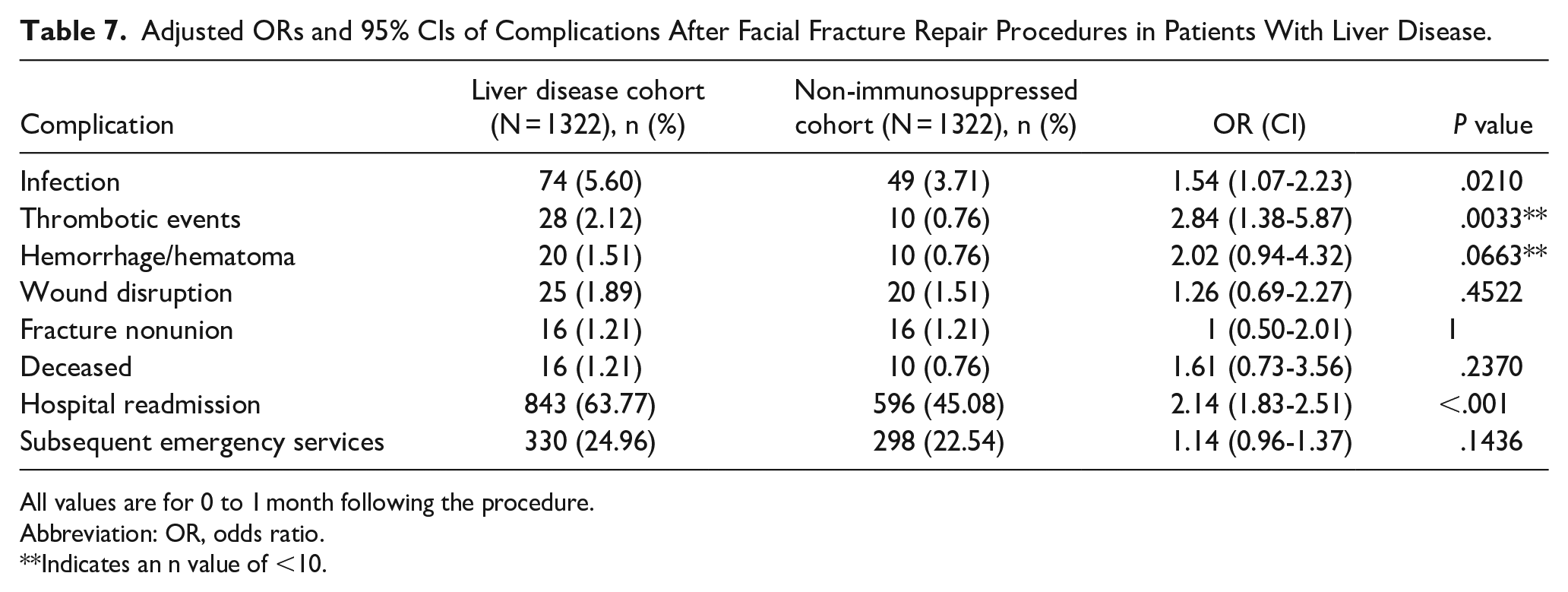
All values are for 0 to 1 month following the procedure.
Abbreviation: OR, odds ratio.
Indicates an n value of <10.
Discussion
To the best of our knowledge, there is no previously published data regarding postoperative complications after facial fracture repair in patients based on their immune status. Our study showed that immunosuppressed patients overall were more likely to experience postoperative infection, thromboembolic events, hemorrhage, wound disruption, hospital readmission, and subsequent emergency department encounters within 30 days following facial fracture repair. Patients with diabetes, CKD, and liver disease were more likely to experience postoperative infections. Rates of other complications such as wound disruption and hospital readmission were also higher in several of the immunosuppressed cohorts.
Facial fractures are common sequelae of trauma and often require surgical repair. Though the reported percentage of patients who experience postoperative complications after facial fracture repair is as low as 1%, the large volume of patients warrants exploration into the etiology and management of these complications. 17 In the United States, the prevalence of SSIs after open reduction and internal fixation for mandibular fractures has been reported to be around 4.2% with high heterogeneity. 18 SSI may contribute to significant patient morbidity and increased healthcare costs. 19 Our results included an analysis of hospital readmission and subsequent emergency department utilization, showing that immunosuppressed patients being treated for facial trauma had higher rates of both these outcomes within 30 days. Further characterization of postoperative complications may allow clinicians to better treat these patients and improve patient quality of life and morbidity.
The relationship between diabetes and postoperative complications has been well studied. One study from 2007 reported an increased risk of postoperative infection following treatment for mandibular fractures in patients with diabetes, HIV, and substance use disorder.20,21 Other studies have previously shown that patients in the United States who smoke tobacco and patients with diabetes were at increased risk of postoperative complications within 30 days of a facial fracture repair.17,22 Another large retrospective cohort study of over 8 million hospitalizations for facial fracture repair nationwide demonstrated that there was a significant association between diabetes and greater length of stay, increased hospital charges, and risk of postoperative complications. 7 These results are consistent with our analysis showing increased risk of SSI, thromboembolic events, wound disruption, and hospital readmission in patients with diabetes. Diabetes has been shown to have negative impacts on general surgical outcomes due to vascular, neuropathic, immune-mediated, and biochemical abnormalities as a result of hyperglycemia leading to impaired wound healing.23,24
Underlying liver conditions have been shown to increase the risk of patient mortality. Our study demonstrated that patients with liver disease had higher rates of infection, thromboembolic events, and readmission, which is generally consistent with the literature. One study examining patients receiving emergency general surgery showed that individuals with any form of underlying liver disease experienced increased mortality risk due to numerous factors such as sepsis, dialysis, ascites, and respiratory failure. 25 Similar outcomes have been seen in patients with liver disease undergoing various other procedures including spinal deformity surgery, craniotomy, and carotid endarterectomy.26-28 However, patients with liver disease generally have a greater likelihood of having preexisting comorbidities that could contribute to increased rates of wound disruption or infection, including advanced age, obesity, type 2 diabetes, and environmental risk factors such as substance abuse, risky sexual behaviors, and exposure to contaminants in food and water. 29 Our study controlled for these factors, which could lead to underrepresentation of complications. Furthermore, the increased rates of hospital readmission may have been explained by these risk factors.
Interestingly, our study did not see a similar difference in postoperative complications in patients with HIV based on immune status. HIV is a chronic inflammatory state leading to increased endothelial cell dysfunction, atherosclerosis, and thrombosis. 30 Therefore, a patient with a lower CD4 cell count (and therefore more progressive disease) may be more likely to experience a thrombotic event. Since patients with HIV have hindered immune systems, infections are more common, including at the surgical site. One study found that the CD4/CD8 ratio in a patient with HIV was helpful in assessing the risk of SSI, showing that there was an inverse relationship between CD4 count and risk of SSI. 31 The CD4/CD8 ratios were not known for the patients in our study. Further studies are needed to determine the risk of postoperative complications in patients with HIV, especially considering the severity of disease.
Our study showed that patients with CKD had an increased rate of postoperative infections. Patients with CKD are at an increased risk of having low serum albumin levels due to increased loss of albumin in the urine. This contributes to the loss of essential proteins needed to help promote wound repair. Older patients with decreased serum levels of albumin are more likely to develop complications such as early SSI. 32 Immunosuppression in CKD is also due to the significant loss of protein and other essential inflammatory molecules in the urine. 9 The current literature on this topic is mixed. One study on patients receiving bariatric surgery demonstrated an increased risk of postoperative complications in patients with CKD, 33 while another study showed that there was no difference between patients with CKD and those without kidney disease and their risk of SSI and other complications. 34 The extent or staging of CKD was not known in our cohort. Previous studies have shown that postsurgical outcomes such as flap failures are associated with late-stage renal disease and renal transplantation. It is possible that our results did not adequately capture the full spectrum of renal failure, which may have skewed our results. Due to inconsistencies in the literature, further studies are needed to determine the risk of postoperative complications in patients with CKD.
Another finding in our study was that patients taking chronic immunosuppressive medications had increased rates of postoperative complications. The impact of immunosuppressive treatment, encompassing monoclonal antibodies (MABs), biologics, and other immunosuppressants, has been researched in the context of patients undergoing treatment for common immunosuppressive conditions. Transplant recipients often receive similar medications, resulting in chronic immunosuppression in both patient groups. For this reason, we did not include a separate group of patients who had undergone organ transplantation. Several studies examining patients with inflammatory bowl disease (IBD) and psoriasis reported that these patients had worse postoperative outcomes, including SSIs, sepsis, and procedural complications.35,36 However, other research suggests that specific drugs such as vedolizumab may exert more significant effects on surgical complication rates compared to others. 37 Other medications that suppress the immune system include MABs. MABs were found to increase the risks of all SSIs in a meta-analysis regarding patients with inflammatory bowel disease. 38 These results support our findings and emphasize that there is a balancing act between suppressing the immune system and avoiding operative complications. In our analysis, we did not focus on individual drugs but aimed to comprehend the impact of immunosuppressive medications as a class. Furthermore, the relationship between biologics and postoperative morbidity remains poorly understood, especially in the context of facial trauma.
This study is not without limitations. The definition of immunosuppression is broad and variable. Another limitation to this study is that it is a database study which relies on the accuracy of charting, which may not be consistent between HCOs in TriNetX. However, our analysis included multiple institutions thereby improving the generalizability of our results. Furthermore, due to the fairly low rate of complications in these patients in clinical practice, our propensity score matched outcomes may be inflated due to the small cohorts. However, we determined that it was important to recognize and control for confounding variables due to the heterogeneity of this population. We also recognize that prolonged use of glucocorticoid medications may also suppress the immune system; however, these medications were not included in our analysis as the database did not allow us to differentiate between short-term and long-term steroid use. Last, TriNetX does not provide information regarding the exact dose of a medication, the route in which a medication was administered, and the severity of a patient’s disease which may affect outcomes in patients who sustained facial fractures.
Surgeons may consider measures to decrease postoperative risk in these patients. Such measures could include close monitoring of perioperative antibiotic use and counseling of patients with diabetes, CKD, those on immunosuppressive medications, and other comorbidities that make any postoperative complication more likely. Although studies show that prophylactic antibiotic administration is common when managing traumatic mandibular fractures, there is significant variability in clinical practice. 39 A recent consensus on postoperative antibiotic prophylaxis in patients with facial fractures determined that postoperative antibiotic prophylaxis is likely unnecessary in healthy patients. 40 However, other studies have found some benefits to short courses of antibiotics to prevent sequelae while avoiding complications associated with antibiotic use such as Clostridium difficile colonization.41,42 Based on our results, it may be worthwhile to utilize a short course of postoperative antibiotics in immunosuppressed patients, as well as continue close monitoring and follow up for these patients. Further large studies on specific subtypes of immunosuppression may be useful to understand optimal patient management in these cohorts.
Conclusion
Based on our findings, patients with diabetes mellitus, CKD, and liver disease may benefit from measures to decrease postoperative complications, including short courses of prophylactic antibiotics, extra attention and planning regarding treatment, and more frequent follow-up. Future studies should aim to implement these changes and compare the rates of postoperative complications to previous years where these practices were not as widely implemented.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241275257 – Supplemental material for The Role of Immunosuppression on Postoperative Outcomes in Facial Fracture Repair
Supplemental material, sj-docx-1-ear-10.1177_01455613241275257 for The Role of Immunosuppression on Postoperative Outcomes in Facial Fracture Repair by Hänel W. Eberly, Andrew J. Rothka, Bao Y. Sciscent and Jessyka G. Lighthall in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
None.
Data Availability Statement
Data are available on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1 TR002014. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Ethical Approval
This study was approved by the Pennsylvania State University Institutional Review Board (STUDY00018629).
Informed Consent
The need to obtain informed consent was waived for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this noninterventional study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.